
Abstract
Background:
Medically intractable ascites causes substantial distress in patients with palliative disease. Tunneled peritoneal catheters have been established as a feasible treatment option allowing patient-controlled paracentesis in a homecare setting. However, while a range of complications is associated with these drainages, risk factors for complications have not been identified so far.
Objectives:
To explore potential risk factors associated with complications of tunneled peritoneal catheters.
Design:
Retrospective observational cohort study.
Methods:
Single-center cohort comprising 49 patients with palliative disease receiving 57 tunneled peritoneal catheters at a tertiary care hospital.
Results:
Catheter placement was successful in all patients and associated with low numbers of severe complications. Our data suggest a higher risk for severe late complications in patients with benign disease, with drainage replacement, and when performed by less experienced physicians.
Conclusion:
Tunneled peritoneal catheters are an effective and safe option to treat symptomatic ascites in patients with end-stage palliative disease. The indication should be carefully considered in patients with benign disease and after removal or dislocation of a previous catheter.
Introduction
Peritoneal carcinosis with malignant ascites is a frequent finding in patients with advanced cancers1,2 and substantially impairs these patients’ quality of life by causing symptoms such as abdominal distension, pain, shortness of breath, or vomiting. 3 Moreover, several benign conditions can also lead to recurrent and causally intractable ascites. 4
In many cases, conservative measures cannot sufficiently control such ascites, and palliative interventional drainage is required. 5 Since repetitive paracentesis may also compromise the patient’s quality of life due to procedure-related pain, frequent contact with the healthcare system, or complications,6–8 tunneled peritoneal catheters have been successfully used for patient-controlled long-term drainage at home. 9
While the feasibility of this approach has been demonstrated in various reports,10–14 adverse events during placement and long-term use of tunneled peritoneal catheters have also been reported, for instance, including bleeding, infection, or dislocation.15,16 However, risk factors for the emergence of such events have only been poorly investigated.
Here, we aimed to identify patient, disease, and intervention characteristics associated with long-term favorable and unfavorable outcomes of tunneled peritoneal catheters in a retrospective single-center cohort study.
Materials and methods
Patients and study design
This study is based on the retrospective analysis of a total of 57 consecutive tunneled peritoneal catheters implanted in 49 patients with otherwise intractable symptomatic ascites in a palliative setting at the Department of Medicine 1 of the University Hospital Erlangen, Germany, between July 2020 and May 2024.
Follow-up data were collected from the patient’s electronic medical records by a single investigator. Cases were followed from the time of catheter placement until death, catheter removal/dislocation, or loss to follow-up. General patient characteristics, technical success, and potential complications associated with catheter placement and use were collected. Investigators were categorized as experienced or inexperienced based on whether they had previously performed more or less than 20 tunneled peritoneal catheter placements, respectively.
Technical success was defined as the correct placement of a functional catheter into the peritoneal cavity. Complications were graded according to the Society of Interventional Radiology adverse event (AE) classification system. 17 Grade 3 or higher complications were considered severe. Early complications probably associated with the procedure itself were defined as appearing within less than 5 days of catheter placement. Catheter-associated peritonitis was defined as the presence of general clinical and/or laboratory signs of infection with evidence of peritonitis as documented by an increase in ascites neutrophil count (>250/µL) and/or positive microbial cultures. Catheter-associated relevant bleeding was defined as any evidence of bleeding that required medical or interventional treatment. Catheter-associated volume depletion was defined as a new-onset systolic blood pressure <100 mmHg requiring a specific intervention and/or new-onset renal failure. Catheter-associated structural injury was defined as the perforation of adjacent organs or structures. Catheter-associated pain was defined as local discomfort at the catheter insertion site or a post-intervention increase of two points or more on the numeric rating scale.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 18
Peritoneal catheter placement
Tunneled peritoneal catheters (PeritX™, ewimed, Hechingen, Germany) were placed independently of this study as part of clinical routine care and according to a standard protocol in patients providing informed written consent and showing no clinical signs of active infection. A single shot of 3 g ampicillin/sulbactam or, in case of allergy, 1.5 g cefuroxime was given iv 60 min prior to the intervention. Briefly, after the identification of a feasible insertion site and the exclusion of intervening vessels by ultrasound, the procedures were performed under sterile conditions and with ultrasound guidance. Local anesthesia with 30–40 mL 1% scandicain was applied and, if preferred by the patients, additional analgesia and/or sedation was provided with midazolam, pethidine, or pritramide. Using the material provided in the PeritX™ set, the ascites was punctured and a guidewire was inserted. A subcutaneous tunnel of approximately 8 cm ending at the guidewire insertion site was prepared with the blunt device provided and the catheter was placed into the tunnel so that the cuff was located approximately 1 cm from the orifice. Using a 16 French split dilator system, the access to the peritoneal cavity was dilated via the guidewire. Upon removal of the core bougie and guidewire, the catheter was advanced into the peritoneum via the sheath, which was gradually split and removed. One to two sutures were placed and a sterile dressing was applied.
Homecare was arranged individually. Materials were provided by ewimed directly to the patients. In addition, most patients were enrolled in a specialized outpatient palliative care program.
Statistical analyses
Statistical analysis was performed using GraphPad Prism v10 (Graphpad Software Inc.). Descriptive analysis was used to assess general patient characteristics and the long-term catheter performance and complications. For patients receiving more than one drainage, patient characteristics consider the time point of the first catheter implantation. Data are presented as mean with range and/or standard deviation for continuous variables and percentages for categorical variables. Patient and catheter survival were plotted using the Kaplan–Meier method.
In the univariable analyses, categorical variables were compared using Fisher’s exact test (for frequencies < 5 and contingency tables >2 × 2) or the Chi-square test (other cases). Continuous variables were compared using the Mann–Whitney-U test for nonparametric data or unpaired t-test for parametric data. All tests were two-tailed and p < 0.05 was considered significant.
In the second step, we built multivariable logistic regression prediction models for late complications. Parameters with a p-value < 0.15 on univariable analysis were included 1 after assessment for collinearity.
Results
Baseline characteristics
From July 2020 to May 2024, a total of 57 tunneled peritoneal catheters were placed in 49 patients. A total of seven patients had two catheter implantations and two patients had three catheter implantations. The patients had a mean age of 62 years (range 33–94), and 63.3% were female. The mean Eastern Cooperative Oncology Group (ECOG) performance status was 2.3 (range 0–4) and the mean BMI was 25.2 (range 15.2–42.5). 8.2% of the patients were underweight, while 44.8% were overweight or obese (Table 1).
Baseline characteristics.

All patients suffered from an incurable disease and were treated in a palliative setting. The majority (81.6%) had an underlying malignant condition, whereas 18.4% suffered from benign disease (Table 2). All malignant diseases were Union international contre le cancer (UICC) stage IV with hepatobiliary cancer (34.7%), gynecological cancer (28.5%), and gastrointestinal cancer (10.2%) being the most prevalent indications. The most frequent benign condition was end-stage hepatic cirrhosis (10.2%). Around two-thirds of the patients (62.5%) still received active treatment (e.g., chemotherapy), while 37.5% received best supportive care.
Indications for tunneled peritoneal catheter placement.

Technical and long-term success
All procedures (100%) were technically successful (Figure 1). A mean of 3.9 L of ascites was drained within 24 h after catheter insertion.

Representative ultrasound images demonstrating symptomatic ascites (left) and a correctly placed tunneled peritoneal catheter (right).
The mean documented catheter days per patient were 43.0 ± 76.3 days (range 1–396; Figure 2) in all patients and 64.1 ± 88.6 days in those patients followed up until death, catheter removal, or under continued follow-up. The mean documented overall survival after catheter insertion was 60.8 ± 98.5 days (range 1–478) in all patients and 91.4 ± 111.8 days in patients followed up until death, catheter removal, or under continued follow-up. In 14 patients, the drainage was removed or dislocated.
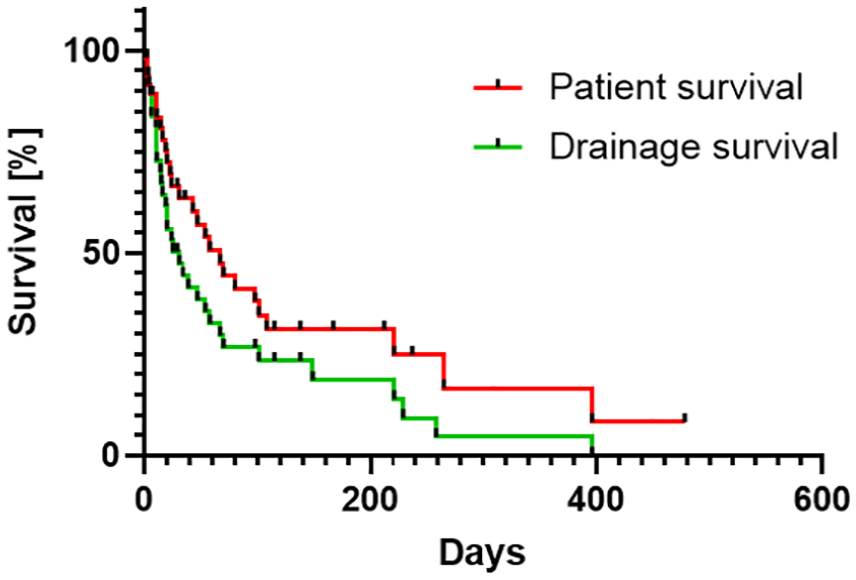
Kaplan–Meier plot of catheter survival and overall patient survival after implantation of the tunneled peritoneal catheters.
Early complications
In general, most early AEs were mild and could be managed with temporary conservative measures (Table 3). We did not observe any injury of adjacent organs, allergic reactions, or infections within the first 5 days after placement of the tunneled peritoneal catheters. Bleeding occurred in two patients (3.5%), in one of them (1.8%) this was considered severe as it required intensive care unit observation and red blood cell transfusion. A total of 24 patients (42.1%) reported pain at the catheter insertion site or a general increase in pain shortly after catheter placement. However, only five of them required a temporary increase or addition of analgetics. Volume depletion with signs of acute kidney failure and/or hypotension was noted in a total of three patients (5.4%) following catheter placement and was managed with fluid and albumin replacement.
Early complications.

Late complications
Later complications (i.e., 6 days or more after catheter placement) were observed in 12 patients (21.1%). In general, these were mostly also mild and could be managed conservatively (Table 4). Five patients experienced secondary infectious complications after a mean of 26.6 days including cellulitis (n = 1, 1.8%) and peritonitis (n = 4, 7.0%). These were considered severe AEs since they required hospital admission. All of them received antibiotic therapy, in four of these cases, the catheter was removed. In four patients (7.0%), accidental dislocation of the drainage occurred after a mean of 71.3 days. Three of them later received a new tunneled catheter. Further two patients (3.5%) experienced transient peri-catheter leakage of fluid after a mean of 26 days. In one refractory case, this was successfully managed by applying two annular sutures around the subcutaneous tunnel of the catheter for 2 weeks. In addition, one case (1.8%) of acute kidney failure and hypotension was recorded after 62 days and required transient volume replacement therapy.
Late complications.

Risk factors for early and late complications
While these numbers showed that tunneled peritoneal catheters rarely lead to severe complications, we further aimed to interrogate whether baseline patient- or disease-related factors might be associated with a higher or lower risk of the emergence of early and late complications.
To this end, we performed univariable analyses for the overall complication rate, the overall rate of severe late complications (i.e., infections), early complications, and the rate of volume depletion. We considered patient characteristics (age, performance status, BMI), disease characteristics (dignity of the underlying disease), interventional aspects (experience of the physician, first or further drainage, pre-interventional antibiotic prophylaxis, pre-interventional C-reactive protein), and post-interventional aspects (drainage volume within the first 24 h, type of homecare) as potential impact factors.
Surprisingly, patients experiencing any early complications were younger than those without early complications (Supplemental Table 1). Otherwise, as for early volume depletion (Supplemental Table 2), none of the factors investigated was associated with a clearly higher or lower risk for complications. Importantly, there was also no association of drainage volume within the first 24 h and early volume depletion.
Late complications were significantly more frequent in patients with benign disease compared with those with malignant disease. Importantly, this was not related to the exposure time since we observed one late complication per 123 catheter days in patients with malignant disease and one late complication per 57 catheter days in patients with benign disease. Moreover, an increased rate of late complications was observed in patients receiving their second or third drainage compared to insertion of the first drainage (Table 5). Surprisingly, pre-intervention C-reactive protein (CRP) was lower in patients without than in patients with any late complications. Moreover, there were trends toward poorer performance status, higher BMI, and procedure performance by less experienced physicians in patients with late complications. When focusing on severe late complications (i.e., in our cohort, infections), there was a substantially higher rate of such events in patients receiving a second or third drainage than in patients receiving a first tunneled catheter (Table 6). In fact, we observed only one infection upon primary drainage (2.2%), while all the others occurred during second or third drainage (36.4%). Moreover, significant differences were noted for the dignity of the underlying disease (higher rate of benign disease in patients with complications) and physician experience (higher complication rate, when performed by physicians with less than 20 interventions). A trend was observed for BMI (lower in patients with complications) and specialized palliative care (less prevalent in patients with complications).
Univariable analysis of factors associated with any late complication.

Univariable analysis of factors associated with any severe late complication.

On multivariable logistic regression for any late complication (Supplemental Table 3) or severe late complications (Supplemental Table 4), none of the factors identified remained a significant independent predictor. However, in both analyses, there was a clear trend for an increased complication risk upon catheter replacement (second or third tunneled drainage) and when performed by less experienced physicians with the nominal Odd’s ratios reaching 10.7 and 11.3, respectively, for severe complications.
Discussion
Symptomatic ascites heavily impacts the quality of life of patients with incurable malignant or benign diseases and, thus, drainage is frequently required. Tunneled peritoneal catheters are an established device to allow permanent ascites drainage in a homecare setting. Although the feasibility and overall low risks of this approach as well as cost-effectiveness compared to repeated large-volume paracentesis2–4 have been demonstrated in several studies, the severe condition of the patients requires careful consideration of the indication.
Main findings
The technical success rate and complication rates described in our study are overall well compatible with previously published literature and confirm that tunneled peritoneal catheters are an effective and safe treatment option for otherwise intractable ascites in patients with incurable underlying disease.10,12,14,19
However, the main focus of our study was to identify patient-, disease- or intervention-inherent factors that might predispose to AEs associated with tunneled permanent ascites drainage. Our analyses did not identify any relevant risk factor for early complications but suggest that a higher risk for late complications and particularly infections exists in patients with benign disease, when the catheter is placed after previous removal or dislocation of another catheter and when performed by less experienced physicians.
What this study adds
Numerous single-center cohorts reporting patients receiving tunneled peritoneal catheters have been published. Overall, technical success rates below 100% have rarely been described and only a few procedure-related severe complications have been reported.9,12,20 However, complications may occur—time-sensitive overall complication risks of 3.7% per week 2 and 43% per year 5 have been calculated—and, in particular, infection of the indwelling catheters is a concern. Accordingly, bacterial colonization is a frequent event and peritonitis has been reported in up to 33%. 6 In most studies, infection rates vary between 2% and 13%,5,7–13 although definitions and grading differ. Further complications reported in the literature include obstruction, dislocation, fluid leakage at the entry site, and hypotension. Yet, risk factors for such AEs have been rarely reported and, thus, guided strategies for considering the indication and for long-term patient management are lacking. In one study, pancreatic cancer was significantly associated with more frequent drainage obstruction 5 and another group reported that catheter days in patients with active treatment are higher than in those on best supportive care. 13
In this regard, our data are the first to show that, while there seems to be no relevant risk factor for early complications, a number of aspects need to be considered when envisioning the risk of late complications. In particular, we show for the first time that the risk of infection is substantially increased after placement of a second or third drainage reaching 36.4% as opposed to 2.2% after primary drainage. This is not surprising, since manipulation during catheter removal or dislocation as well as the temporary fistula may provide entry sites for subclinical superinfection that may later lead to overt infectious complications. Thus, patients should actively be counseled to avoid inadvertent dislocation and the indication for a second or further drainage should be carefully made. Moreover, we show that the long-term complication risk is increased in patients with benign disease, which was surprisingly not associated with exposure time. Third, although only reaching borderline significance, the findings suggest that fewer complications are observed, when placement is performed by more experienced physicians, which indicates that a training curve exists. Importantly, since we found that pre-intervention CRP was lower in patients with late complications than in patients without late complications, high CRP may not be considered a feasible biomarker of increased infection risk in patients eligible for tunneled peritoneal catheters. One explanation for this phenomenon might be that many patients with end-stage malignant disease show high CRP levels without infection. It should also be mentioned that the patient’s BMI was associated with the emergence of late complications. However, while patients with any late complication had, on average, a higher BMI, the opposite was the case in patients with severe late complications as compared to those without complications. Thus, this observation needs to be interpreted with caution and we do currently not see any clear consequence for clinical practice.
Limitations
Our study has a number of limitations that need to be considered when interpreting the results. First, it is a retrospective study and, thus, reporting bias might be an issue. Moreover, it is a single-center study reporting data from a tertiary center in Germany and local specifics might contribute to the findings and limit their generalizability. With a total of 49 patients and 57 drainages, our cohort is of substantial size, but may, however, be too small to identify rare adverse events (AEs). Moreover, the multivariable analyses for risk factors underlying these AEs might be underpowered since none of the aspects reached statistical significance despite showing clear differences in univariable analyses. It must be noted, however, that one or the other of these caveats applies to almost all published cohorts. While only a few of them report prospective data, 13 only one cohort is sufficiently larger than ours. 5
Strengths
On the other hand, a number of strengths have to be underscored: Importantly, our study is the first to systematically investigate the association of baseline parameters and AEs. Thus, it provides substantial novelty of clear clinical relevance and implications for patients under palliative therapy.
Conclusion
Overall, we conclude that our findings support the concept that tunneled peritoneal catheters should be considered early on in the management of malignant ascites since interventional risks are low and patient comfort is high. On the contrary, in benign ascites, tunneled peritoneal catheters should be reserved for selected cases, where other options such as transjugular portosystemic shunt placement are not an option and which are refractory to diuretics. In general, placement of another drainage after a previous infectious complication should be well justified.
Larger and prospective multi-center trials are warranted to follow up on our findings and to further improve the pre- and post-procedural management of patients with intractable ascites eligible for permanent tunneled peritoneal catheters.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241310183 – Supplemental material for Risk factors associated with complications of palliative drainage of ascites with tunneled peritoneal catheters
Supplemental material, sj-docx-1-tag-10.1177_17562848241310183 for Risk factors associated with complications of palliative drainage of ascites with tunneled peritoneal catheters by Domenique Machnik, Sarah Fischer, Marcel Vetter, Ricarda Lamprecht-Bailer, Rachel Rouse-Merkel, Daniel Klett, Markus F. Neurath, Deike Strobel, Sebastian Zundler and Sophie Haberkamp in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.