
Abstract
Background:
Crohn’s disease (CD) exhibits variability in colorectal cancer (CRC) incidence and prognostic factors due to diverse clinical and behavioral characteristics, presenting inconsistencies between Western and Eastern patients.
Objectives:
This study compared clinical characteristics between CD patients with CRC from the US and Korean tertiary referral centers and defined the prognostic factors related to mortality.
Design:
Retrospective study.
Methods:
We reviewed the electronic medical records of 236 adult CD patients with colorectal adenocarcinoma evaluated at Mayo Clinic Rochester, Florida, or Arizona (N = 200) and Asan Medical Center in Korea (N = 36) between January 1989 and August 2022.
Results:
Asan patients had a younger age, shorter CD duration, more colonic involvement (L2 plus L3), penetrating behavior, perianal fistula, and shorter biological treatment duration before CRC diagnosis than Mayo patients. Furthermore, despite significant differences in body mass index, smoking status, primary sclerosing cholangitis, immunomodulators, CRC diagnosis period, clinical presentation, CRC location, surgery, and some histopathological details between the two groups, overall survival was not statistically different (p value, 0.29, log-rank test). Advanced age (adjusted hazard ratio (aHR), 1.03 per year; 95% confidence interval (CI), 1.01–1.04; p value, <0.01), unresectable CRC (aHR, 5.02; 95% CI, 2.49–10.12; p value, <0.01), and advanced CRC stage (aHR, 1.45 per stage; 95% CI, 1.07–1.97; p value, 0.02) were significantly associated with increased risk of death. CD remission at CRC diagnosis (aHR, 0.26; 95% CI, 0.08–0.91; p value, 0.04), CRC diagnosis period of 2011–2022 (aHR relative to 1989–2000, 0.46; 95% CI, 0.25–0.87; p value, 0.02), and CRC diagnosis by surveillance (aHR, 0.56; 95% CI, 0.32–0.98; p value, 0.04) were significantly associated with decreased risk of death.
Conclusion:
Notably, some clinical features of CD with CRC differed between Asan and Mayo patients; however, overall survival was not different. CD remission, CRC surveillance, and more recent diagnosis of CRC were associated with a reduced risk of death.
Introduction
Colorectal cancer (CRC) is a significant concern in patients with inflammatory bowel disease (IBD), as these patients have a higher risk, approximately two- to threefold, of developing CRC and poorer overall survival than the general population.1–3 The exact mechanism is unclear, but it is thought to be related to the chronic inflammation of the colon and rectum. 4 A systematic review and meta-analysis of prognostic variables for high-grade dysplasia and CRC in IBD revealed that extensive disease, post-inflammatory polyps, dysplasia, perianal disease, stricture, primary sclerosing cholangitis (PSC), family history of CRC, and appendectomy were strongly associated with advanced colorectal neoplasia in IBD patients. 5 Recent studies reported a decrease in the incidence of IBD-related CRC over time due to increased use of medication to reduce inflammation, such as immunomodulators (IMMs) and biologic agents, as well as advanced endoscopic surveillance for early detection and resection.1,6–8
Compared to ulcerative colitis (UC)-associated CRC, Crohn’s disease (CD) patients with CRC had poorer overall survival.3,9 Moreover, CRC incidence, risk factors, and factors affecting its prognosis in CD patients vary significantly due to its diverse clinical and behavioral characteristics, such as the severity and duration of the disease and the extent of inflammation in the colon. There may be differences between regions and hospital-based studies compared to population-based studies.5,10–13 A systematic review and meta-analysis showed a similar risk of CRC in Asian patients with UC compared to Western patients. 14 However, the standardized incidence ratios of CRC in CD were inconsistent between Eastern and Western patients. Asian patients tend to have more anorectal cancer than Western patients because of more perianal involvement in this population.15–17 This study aimed to compare CD patients’ characteristics and clinical outcomes with CRC between US and Korean tertiary referral centers and define the prognostic factors related to death. By understanding the differences and similarities between the two populations, healthcare providers can improve the management of this complex disease.
Materials and methods
This study was a retrospective chart-based review conducted after approval by the Institutional Review Board. Patients’ medical records whose research authorization was withdrawn were not examined. The electronic medical records of adult CD patients (aged 18 years or older) with colorectal adenocarcinoma who were evaluated at Mayo Clinic Rochester, Florida, or Arizona and Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea, between January 1, 1989, and August 31, 2022, were assessed. Mayo Data Explorer was utilized to identify potential Mayo Clinic patients. The diagnosis of CD was based on clinical, endoscopic, histopathologic, and/or radiologic criteria. The diagnosis of colorectal adenocarcinoma was confirmed through histopathology. Patients were excluded if they developed CD after establishing colorectal adenocarcinoma or were diagnosed with hereditary cancer syndrome.
Data on the patient’s basic demographics, cigarette smoking habits, PSC, IBD in the patient’s family, and CRC in first-degree relatives were obtained. Clinical details of CD include the date of diagnosis, disease duration, location and behavior, the presence of perianal disease or fistula, CD medication usage, and surgical history, and endoscopic factors such as post-inflammatory polyps, strictures, scars, and dysplasia before CRC diagnosis were retrieved. Clinical information of colorectal adenocarcinoma, including the date of diagnosis, clinical presentation, location, carcinoembryonic antigen (CEA) level, American Joint Committee on Cancer (AJCC) Tumor Node Metastasis (TNM) stage using the 8th Edition AJCC Cancer Staging Manual, 18 treatment, status at last follow-up, date of endpoint, and histopathological details such as microsatellite instability (MSI), differentiation, mucinous component, signet ring cell component, lymphovascular invasion, perineural invasion, and tumor bud score were collected.
This study’s reporting conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 19
Statistical analysis
Descriptive statistics provided an overview of the demographic data, characteristics, and outcomes. The two groups were compared using the Wilcoxon rank-sum test or Pearson’s Chi-squared test. The log-rank test was used to compare the survival curves that the Kaplan–Meier method produced. Univariate and multivariate Cox-proportional hazard regression models were applied to determine the hazard ratios of death-related variables. Statistical significance was considered as a p value, <0.05. The statistical analysis utilized BlueSky Statistics software v. 7.40 (BlueSky Statistics LLC, Chicago, IL, USA).
Results
A total of 236 CD patients with CRC were identified during the 33-year study period, including 200 patients from the USA and 36 from Korea. Figure 1 displays the flowchart depicting all patients included in the study. Demographic characteristics, clinical data, and outcomes for the study patients were presented in Table 1. There was no significant difference in gender or family history of IBD or CRC in first-degree relatives between the two groups. Fifty-six percent of patients were male. Approximately 13% and 9% of patients had a family history of IBD and CRC in first-degree relatives, respectively. The median age at CRC diagnosis (56.0 vs 35.1 years; p value, <0.01), body mass index (BMI; 25.3 vs 20.5 kg/m2; p value, <0.01), and prevalence of PSC (11.5% vs 0%; p value, 0.03) were significantly higher in Mayo patients compared with Asan patients. Approximately 60% of all patients never smoked cigarettes. Notably, 19.4% of Asan patients currently smoked, and 19.4% were ex-smokers. In contrast, 5.5% of the Mayo patients currently smoked, and 35.0% were ex-smokers (p value, 0.01).

Flowchart of the study population.
Demographic characteristics, clinical data, and outcomes of colorectal cancer in patients with Crohn’s disease.

p values were calculated using the Wilcoxon rank-sum test or Pearson’s Chi-squared test.
CD location and behavior were classified according to the Montreal classification (L1, terminal ileum; L2, colon; L3, ileocolon; L4, upper GI; B1, nonstricturing nonpenetrating; B2, stricturing; B3, penetrating; p, perianal diseases include perianal fistulas, abscesses, rectovaginal fistulas, anal fissures).
Right-sided, cecum to the transverse colon; left-sided, splenic flexure to the rectum.
AJCC TNM, American Joint Committee on Cancer Tumor Node Metastasis; AWC, alive with CRC; BMI, body mass index; CD, Crohn’s disease; CEA, carcinoembryonic antigen; CRC, colorectal cancer; DOC, died of other cause; DOD, died of CRC; DUC, died of unknown cause; GI, gastrointestinal; IBD, inflammatory bowel disease; IMM, immunomodulator; NED, no evidence of disease; PSC, primary sclerosing cholangitis.
Clinical information on CD, treatments, and endoscopic factors before CRC diagnosis
The median duration from initial CD to CRC diagnosis in the Mayo patients was significantly longer than that of Asan patients (21.6 vs 12.6 years; p value, <0.01). Both at initial CD and CRC diagnoses, there were significant differences between the two groups regarding CD location, behavior, and perianal fistula. The colon was the most common CD location for Mayo patients (44.9% at initial CD diagnosis and 47.5% at CRC diagnosis). In contrast, the ileocolonic CD was most commonly noted in Asan patients at the initial CD and CRC diagnosis (79.4% and 85.7%, respectively). Only 1.5% of the Mayo patients had upper gastrointestinal (GI) CD, and 5.0% had no active disease at the time of CRC diagnosis. Upper GI CD, or no active disease, however, was not found in any Asan patients. At the time of the initial CD diagnosis, most patients had nonstricturing and nonpenetrating behavior (65.2% of the Mayo patients and 76.5% of Asan patients); Mayo patients had more stricturing behavior (25.8% of Mayo patients vs 5.9% of Asan patients), whereas Asan patients had more penetrating behavior (17.6% of Asan patients vs 9.1% of Mayo patients). At the time of CRC diagnosis, most Mayo patients had nonstricturing and nonpenetrating behavior (55.0%, 37.5%, and 7.5% for nonstricturing and nonpenetrating, stricturing, and penetrating, respectively). In comparison, most Asan patients progressed more to penetrating and stricturing behavior (28.6%, 31.4%, and 40.0% for nonstricturing and nonpenetrating, stricturing, and penetrating, respectively). Asan patients had a significant prevalence of perianal fistula than Mayo patients at initial CD (52.8% vs 10.1%; p value, <0.01) and CRC diagnosis (69.4% vs 25.0%; p value, <0.01).
In terms of CD treatments before CRC diagnosis, Asan patients received IMMs significantly more often than Mayo patients (88.9% vs 53.5%; p value, <0.01). The most commonly used IMMs were azathioprine and 6-mercaptopurine. The median exposure time to IMM did not differ significantly (7.0 years). The median exposure time to biological therapies of the Mayo patients was substantially longer than that of Asan patients (5.2 vs 4.4 years, p value, 0.03); however, the rate of biological treatment was not significantly different (49.5% vs 63.9%, p value, 0.11). Infliximab and adalimumab were the two biological medications that were utilized most frequently. There was also no significant difference in the rate of bowel resection before CRC diagnosis (43.0% of Mayo patients vs 33.3% of Asan patients; p value, 0.28).
Approximately 20% of the endoscopic information before CRC diagnosis was missing. Asan patients had more post-inflammatory pseudopolyps (64.7% vs 40.4%; p value, 0.01) and colonic scars (94.1% vs 11.0%; p value, <0.01) than Mayo patients, while Mayo patients had more colonic strictures (42.9% vs 17.6%; p value, 0.01) and colonic dysplasia (62.4% vs 8.8%; p value, <0.01) than Asan patients.
Clinical information of CRC, treatments, and status at the last follow-up
Only 3% of patients had a prior history of CRC, and the two groups had no significant difference. Most patients were diagnosed with CRC in 2011–2022. None of the Asan patients were diagnosed with CRC between 1989 and 2000. The two groups had significant differences in clinical presentation before CRC diagnosis (p value, <0.01). The most common presentation of CRC cases in Mayo patients was through surveillance (38.5%); however, the most frequent presentations in Asan patients were perianal fistula or anal pain (33.3%). There was also a significant difference in CRC location between the two groups (p value, <0.01). Asan patients had more rectal and left-sided colon involvement (86.1% vs 42.5% and 91.7% vs 57.0%, respectively). However, Mayo patients had a higher rate of more than one location simultaneously (5.5% vs 2.8%). In addition, the prevalence of elevated CEA levels in Mayo patients was greater than in Asan patients at both cutoffs of 3 and 5 ng/mL (41.8% vs 19.4%; p value, 0.03 and 28.6% vs 9.7%; p value, 0.03, respectively).
There were no significant differences in CRC resectability, AJCC TNM stage, and treatments, except for Mayo patients’ overall CRC surgery rate, which seemed higher than that of Asan patients (92.0% vs 80.6%; p value, 0.03). A total of 87.2% of patients had resectable CRC. The stages of CRC included stage I (25.0%), II (33.6%), III (28.0%), and IV (13.4%). Cancer treatments included curative surgery (40.5%), curative surgery with adjuvant chemotherapy (20.7%), curative surgery with adjuvant radiochemotherapy (9.1%), etc.
There were no significant differences between the two groups for status at the last follow-up (p value, 0.37). Approximately half of the patients were alive with no evidence of disease, 4.2% of patients were alive with CRC, 8.1% of patients died of CRC, 7.6% of patients died of other causes, 21.6% of patients died of unknown causes, and 9.3% of patients were lost to follow-up.
Histopathological information of colorectal adenocarcinoma
The two groups had significant differences in cancer differentiation and mucinous component (Table 2). Mayo patients more often had poorly differentiated or undifferentiated cancers, which were classified as high grade, than Asan patients (42.9% vs 8.7%; p value, <0.01); however, Asan patients had mucinous adenocarcinoma more often (47.2% vs 18.0%; p value, <0.01). There was no significant difference in signet ring cell component between the two groups (p value, 0.35). Information on MSI status, lymphovascular invasion, perineural invasion, and tumor bud score data was often missing, and these variables did not significantly differ between the two groups.
Histopathological information of colorectal adenocarcinoma in patients with Crohn’s disease.

p values were calculated using Pearson’s Chi-squared test.
MSI, microsatellite instability; MSS, microsatellite stable
Survival and prognostic factors
The overall survival of all patients in the study is shown in Figure 2. The median overall survival time was 12.5 years (range, 0–27.6 years), and the median follow-up time was 5.6 years after CRC diagnosis. The 1-, 3-, 5-, and 10-year survival rates were 87.2% (95% CI, 82.8%–91.7%), 71.2% (65.1%–77.8%), 64.5% (57.9%–71.9%), and 55.3% (47.8%–63.9%), respectively.

Overall survival among 236 cases of colorectal cancer in patients with Crohn’s disease with the median overall survival time of 12.5 years (range, 0–27.6 years) and the median follow-up time of 5.6 years after CRC diagnosis. The 1-, 3-, 5-, and 10-year survival rates were 87.2% (95% CI, 82.8%–91.7%), 71.2% (95% CI, 65.1%–77.8%), 64.5% (95% CI, 57.9%–71.9%), and 55.3% (95% CI, 47.8%–63.9%), respectively.
There was no significant difference in overall survival between Asan and Mayo patients (p value, 0.29; Figure 3), with the median survival time of not available (range, 0–20.7 years) and 12.0 years (range, 0–27.6 years), respectively. The median follow-up time after CRC diagnosis of Asan and Mayo patients was 7.2 and 5.4 years, respectively. The 5-year survival rates of Asan and Mayo patients were 63.7% (95% CI, 47.7%–85.0%) and 64.7% (57.6%–72.7%), respectively. Univariate Cox regression analysis also showed that institution was not significantly associated with the risk of death (crude hazard ratio, 1.42; 95% CI, 0.74–2.75; p value, 0.29, Table 3).

Overall survival among 236 cases of colorectal cancer in patients with Crohn’s disease stratified by the institution (p value, 0.29, log-rank test). The median survival time of Asan and Mayo patients was unavailable (range, 0–20.7 years) and 12.0 years (range, 0–27.6 years), respectively. The median follow-up time after CRC diagnosis of Asan and Mayo patients was 7.2 and 5.4 years, respectively. The 5-year overall survival rates of Asan and Mayo patients were 63.7% (95% CI, 47.7%–85.0%) and 64.7% (95% CI, 57.6%–72.7%), respectively.
Prognostic factors related to the death of colorectal cancer in patients with Crohn’s disease.

AJCC TNM, American Joint Committee on Cancer Tumor Node Metastasis; BMI, body mass index; CD, Crohn’s disease; CI, confidence interval; CRC, colorectal cancer; HR, hazard ratio.
No significant differences in patients’ overall survival were stratified by the CRC diagnosis calendar period (p value, 0.07; Figure 4). The 5-year survival rates of patients diagnosed with CRC in 1989–2000, 2001–2010, and 2011–2022 were 54.6% (95% CI, 37.3%–79.9%), 58.7% (47.4%–72.7%), and 70.1% (61.8%–79.6%), respectively. There were significant differences in overall survival when stratified by AJCC TNM stage (p value, <0.01; Figure 5). The 5-year survival rates of stage I, II, III, and IV CRC were 83.1% (95% CI, 72.8%–94.8%), 69.9% (59.3%–82.4%), 63.0% (51.2%–77.6%), and 19.5% (7.2%–52.9%), respectively.

Overall survival among 236 CRC cases in patients with Crohn’s disease stratified by the calendar period of CRC diagnosis (p value, 0.07, log-rank test). The 5-year survival rates of patients diagnosed with CRC in 1989–2000, 2001–2010, and 2011–2022 were 54.6% (95% CI, 37.3%–79.9%), 58.7% (95% CI, 47.4%–72.7%), and 70.1% (95% CI, 61.8%–79.6%), respectively.
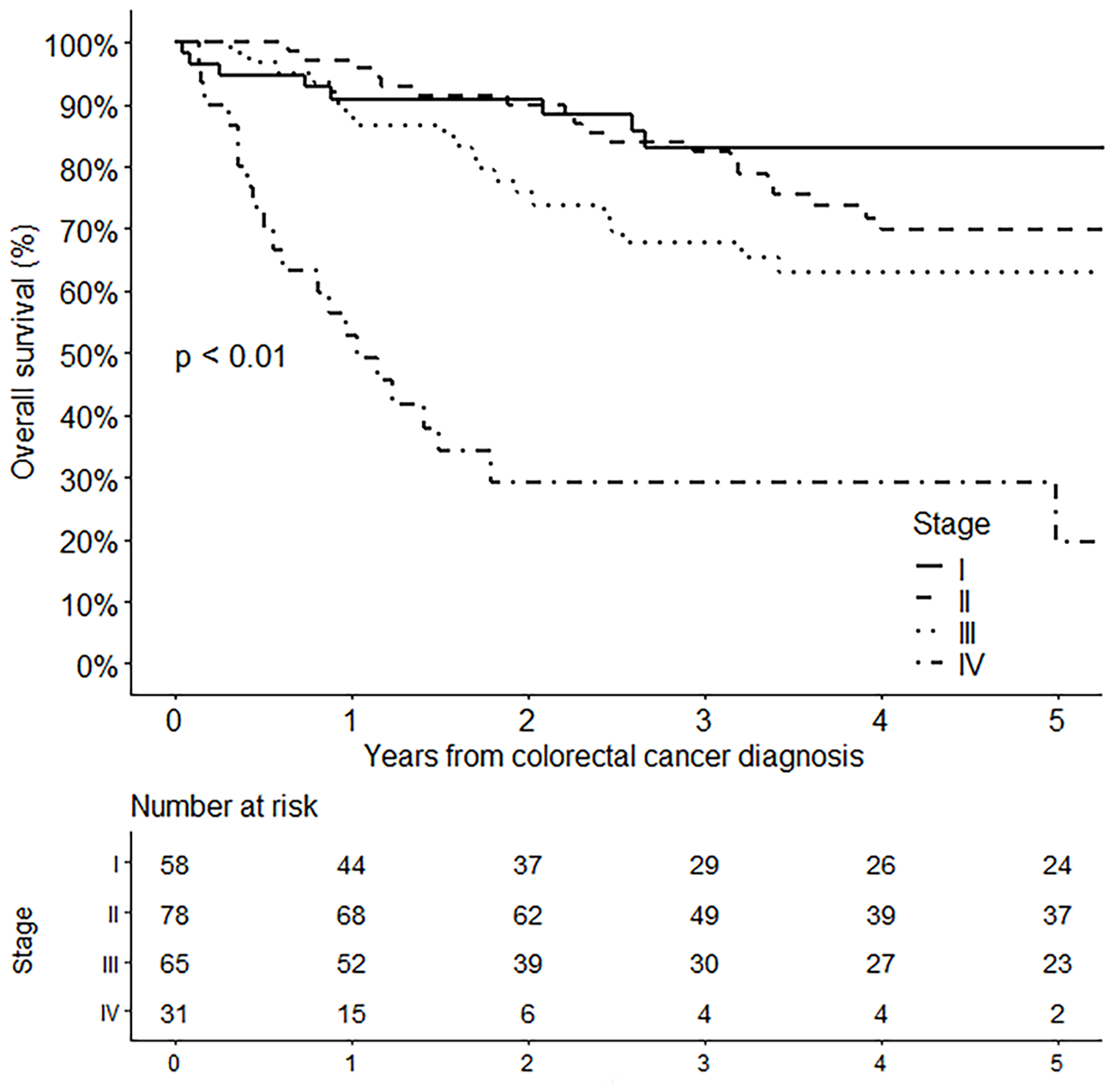
Overall survival among 236 cases of colorectal cancer in patients with Crohn’s disease stratified by AJCC TNM stage (p value, <0.01, log-rank test). The 5-year survival rates of stage I, II, III, and IV were 83.1% (95% CI, 72.8%–94.8%), 69.9% (95% CI, 59.3%–82.4%), 63.0% (95% CI, 51.2%–77.6%), and 19.5% (95% CI, 7.2%–52.9%), respectively.
Multivariate Cox regression analysis revealed that advanced age (adjusted hazard ratio (aHR), 1.03 per year; 95% CI, 1.01–1.04; p value, <0.01), unresectable CRC (aHR, 5.02; 95% CI, 2.49–10.12; p value, <0.01), and advanced CRC stage (aHR, 1.45 per stage; 95% CI, 1.07–1.97; p value, 0.02) were significantly associated with increased risk of death. On the other hand, CD remission at CRC diagnosis (aHR, 0.26; 95% CI, 0.08–0.91; p value, 0.04), calendar period of CRC diagnosis of 2011–2022 (aHR relative to 1989–2000, 0.46; 95% CI, 0.25–0.87; p value, 0.02), and CRC diagnosis by surveillance (aHR, 0.56; 95% CI, 0.32–0.98; p value, 0.04) were significantly associated with decreased risk of death (Table 3).
Discussion
This retrospective study compared demographic characteristics, clinical data, outcomes, and survival of 236 CD patients with CRC who were evaluated at US and Korean tertiary referral centers and assessed prognostic factors related to mortality. Mayo patients could represent Western patients; however, Asan patients might reflect Eastern or Asian patients. Despite some variable differences between the two groups, the mortality risk and overall survival were similar. The 5-year survival rate of all patients in our study was comparable to the general (i.e., non-IBD) CRC population, 20 64.5% versus 65.1%, respectively. The findings of our study differ from those of a study conducted in Japan, which had a larger sample of Asian CD-CRC patients (n = 233). This study found that the 5-year overall survival rates were lower for CD-CRC in comparison to sporadic CRC (54.0% vs 71.2%, p value, <0.01). 21
Asan patients had a significantly younger age at CRC diagnosis compared to Mayo patients (35.1 vs 56.0 years). These findings align with those of a study conducted in Japan, which reported a cancer diagnosis age of 46.9 years. 21 Additionally, Asan patients had a significantly shorter duration from initial CD to CRC diagnosis (12.6 vs 21.6 years) than Mayo patients, even if none had PSC. Based on the recommendations of the American Gastroenterological Association and European Crohn’s and Colitis Organization guidelines, colonoscopy for dysplasia surveillance should be conducted in all colonic IBD patients 8–10 years after disease diagnosis and promptly upon the diagnosis of PSC.22,23 However, based on our findings, if Asian patients do not undergo a surveillance colonoscopy until 8–10 years after CD diagnosis, around 30% of patients will have already been diagnosed with CRC. Therefore, one might consider surveillance earlier than the guidelines for Asian patients. Our study’s multivariate Cox regression analysis also confirmed that CRC, diagnosed by surveillance, was significantly associated with improved survival (aHR, 0.56; 95% CI, 0.32–0.98).
When focused on the disease extent of CD (L2 plus L3), Asan patients had a higher proportion of colonic involvement than Mayo patients at both the initial CD (94.1% vs 75.7%) and CRC diagnosis (97.1% vs 82.5%). Moreover, Asan patients had more penetrating behavior and perianal fistula. Asan patients received IMM at a higher rate and underwent biological therapy at a similar rate, but their biological treatment times were shorter. As a result, no Asan patients achieved CD remission at the time of CRC diagnosis. Our study also found that CD remission was associated with a favorable outcome (aHR, 0.26; 95% CI, 0.08–0.91). A retrospective multicenter study of 316 Japanese CD-associated cancer patients identified that penetrating behavior was significantly associated with poor survival (HR, 1.89; 95% CI, 1.16–3.09) and relapse-free survival (HR, 2.15; 95% CI, 1.28–3.63). 24 On the other hand, our study revealed no significant difference (crude HR of B3/B3p relative to B1/B1p, 0.66; 95% CI, 0.31–1.43). The difference in penetrating definition could explain this; the Japanese study included perianal fistula and ulcer in their definition of penetrating behavior.
Asan patients were started on biologics later in the course of the disease, resulting in a shorter duration of biological treatment before CRC diagnosis and ongoing inflammation. In addition, these patients had a higher prevalence of penetrating disease and perianal fistula. To improve patient outcomes, we recommend the earlier initiation of biologics to achieve remission. Our study found that achieving CD remission significantly lowers the risk of mortality (aHR, 0.26; 95% CI, 0.08–0.91), emphasizing the importance of early intervention in this patient population.
This study’s most common CRC location was the rectum, particularly in Asan patients, making perianal fistula and anal pain the most frequent presenting symptoms. These findings are consistent with those of a study conducted in Japan, which reported that the most common location for CD-CRC was the anorectum (81.6%). 21 The predominance of perianal fistula in Asan patients could also explain this, emphasizing the importance of surveillance for detecting anorectal cancers in this subset of patients. A systematic review and meta-analysis found that 50% of CRC patients had perianal CD, and 36% of these patients were Korean. 25 Our study found a lower prevalence of perianal fistulas (31.8%) due to the smaller representation of Asan patients within our overall patient population. In addition, the CRC location of patients in our study was similar to the result of a systematic review and meta-analysis. 15 In their study compared to ours, the occurrence of left-sided CRC in Western patients was 63.1% versus 57.0%, and in Asian patients, it was 84.1% versus 91.7%. 15 A systematic review and meta-analysis of CRC in the general population showed that left-sided CRC was significantly related to a lower risk of mortality (HR, 0.82; 95% CI, 0.79–0.84). 26 However, our result did not show any association between location and survival (crude HR relative to right-sided, 1.03; 95% CI, 0.65–1.62).
Patients with IBD-associated CRC have higher rates of poor differentiation and mucinous or signet ring cell carcinoma compared to those with non-IBD-CRC. 3 The study from Japan revealed that mucinous adenocarcinoma was the prevailing pathological finding in CD-CRC (38.7%–46.0%).21,27 Conversely, papillary and well-differentiated adenocarcinoma were the predominant pathological findings in UC-CRC and sporadic CRC, at rates of 65.2% and 48.2%, respectively. 27 Poorly differentiated adenocarcinoma and signet ring cell carcinoma were associated with the worst survival. Mucinous adenocarcinoma also tends to have a slightly worse prognosis than non-mucinous adenocarcinoma (HR, 1.05; 95% CI, 1.02–1.08). 28 In our study, Mayo patients had poorly or undifferentiated adenocarcinoma more often than Asan patients (42.9% vs 8.7%, p value, <0.01), who had more mucinous adenocarcinomas (47.2% vs 18.0%, p value, <0.01). The prevalence of signet ring cell carcinoma did not significantly differ between the two groups. The univariate and multivariate regression analysis revealed that mucinous and signet ring cell carcinomas in histopathology were not significantly associated with the risk of death (crude HR, 0.88; 95% CI, 0.56–1.38; and aHR, 1.90; 95% CI, 0.99–3.62, respectively). Other factors, such as lymphovascular invasion, perineural invasion, and tumor bud score, are related to survival. 29 Furthermore, the molecular biomarkers, which were MSI, Kirsten rat sarcoma virus (KRAS), v-RAF murine sarcoma viral oncogene homolog B (BRAF), and caudal-type homeobox 2 transcription factor (CDX2) also had a role in prognosis. 29 Because this information was missing, we could not assess these.
This study discovered that CD patients who were diagnosed with CRC in 2011–2022 had a better prognosis and 5-year survival rate (aHR relative to 1989–2000, 0.46; 95% CI, 0.25–0.87; 5-year survival rate, 70.1% vs 54.6%, respectively). This likely represents advances in CRC treatment strategies that decrease mortality. Unsurprisingly, our analysis found that poor outcome was associated with advanced age, unresectable CRC, and advanced CRC stage. Surgical resection is often the first line of treatment for CRC in CD patients. This may be followed by chemotherapy or radiation therapy, depending on the stage and location of the cancer and the patient’s overall health. The multivariate Cox analysis did not reveal an association between CRC surgery and the risk of death (aHR, 1.08; 95% CI, 0.50–2.34), even though Mayo patients underwent more overall CRC surgery than Asan patients (92.0% vs 80.6%). This suggests that CRC treatment should be a multidisciplinary approach.
Our study is the first to directly compare data from CD patients with CRC in the USA and Korea. This study was a retrospective chart review; however, the electronic database was well-organized. The majority of the important details were thus finished. Despite the cohort’s imbalance resulting from the small number of Asan patients, this discrepancy could introduce biases and compromise the statistical analysis’s reliability. However, certain key characteristics of Asan patients resemble those of larger cohorts, such as the Japanese cohort (n = 233), 21 which could potentially mitigate this limitation in drawing conclusions.
This study has some limitations. Notably, several factors, such as the extension of Crohn’s colitis and histologic severity score of inflammation, were absent in some medical records making it impossible to complete data collection. Additionally, tumors were not reviewed by the same pathologist, potentially impacting the consistency of reporting. Moreover, this is a result of tertiary referral centers. The findings might not apply to other populations, particularly in areas with limited resources for managing CD and CRC.
Conclusion
There were some clinical characteristics differences between the Mayo and Asan patients with CD and CRC; however, the risk of death was not significantly different. CD remission, CRC surveillance, and more recent diagnosis of CRC were associated with a reduced risk of death.