
Abstract
Alpha-fetoprotein(AFP)-producing colorectal cancer is a rare form of colorectal cancer with a high degree of malignancy, advanced stage, strong invasiveness, poor response to treatment, rapid progression, and poor prognosis. Herein, we present the case of a middle-aged (in his 50s) male patient who underwent left neck lymph node biopsy due to “left neck lymph node enlargement for 5 months.” Biopsy results revealed metastatic adenocarcinoma, and computed tomography examination of the chest and abdomen suggested a malignant tumor of the sigmoid colon with multiple metastases. Subsequently, the patient underwent colonoscopy, and the pathological result was colonic adenocarcinoma. Regarding tumor markers, serum alpha-fetoprotein (AFP) was 214 ng/mL. The patient received first- and second-line treatments for colon cancer, but progression-free survival was short. AFP was consistently elevated; after 8 months, the patient had AFP levels of 11,371.8 ng/mL, and imaging confirmed disease progression. The patient subsequently died, with an overall survival of more than 9 months. Compared with other tumor markers, AFP better reflects tumor progression in AFP-producing colorectal cancer.
Introduction
Colorectal cancer is one of the most common malignant tumors worldwide. According to the latest global cancer burden data released in 2020 by the World Health Organization’s International Agency for Research on Cancer, 1 colorectal cancer ranks third in incidence and second in mortality among malignant tumors. In China, the incidence of colorectal cancer has jumped to the second most common malignancy and it is currently the fifth leading cause of cancer-related deaths.
Alpha-fetoprotein (AFP) is a serum glycoprotein synthesized by the liver and yolk sac in early fetal life.2,3 AFP synthesis is then suppressed soon after birth. When malignant lesions occur in the liver and gonadal embryonic tissue, related gene pathways are activated and cells that have lost the ability to synthesize AFP begin to recover this ability, resulting in a significant increase in serum AFP levels. Generally, detecting AFP concentration is of great significance for the diagnosis of malignant liver and germ cell tumors. Malignancies in certain tissues that originate from the foregut endoderm, such as the stomach and bile ducts, can also cause AFP elevation, 4 but elevated AFP is rare in colorectal cancer.5–13
Herein, we report the case of an AFP-producing colorectal cancer in which elevated AFP was accompanied by disease progression. Such patients have poor responses to standard treatment.
Case presentation
The patient was a male in his 50s with a medical history of hypertension and subacute cerebral infarction; history of hepatitis and cirrhosis were denied. He was a drinker for more than 30 years (250 mL of white wine every week) with no history of tobacco use. Initially, the lymph nodes of his left neck were found to be enlarged to approximately soybean size, hard, and without tenderness, which was ignored. Cervical lymph node biopsy was performed 5 months later, and the pathological results showed metastatic adenocarcinoma. Computed tomography of the patient’s chest and abdomen showed a thickened sigmoid wall with homogeneous enhancement; thus, a sigmoid malignant tumor was considered, and there were multiple metastases in the liver, multiple lymph node metastases throughout the body (neck, retroperitoneal, bilateral groin) (Figure 1a), and multiple bone metastases (L2, L3, S1). The patient had abnormal digestive tract tumor markers, including significantly increased serum AFP levels (214 ng/mL, reference value: 0–8.1 ng/mL) and slightly increased serum CEA (8.7 ng/mL, reference value: 0–5 ng/mL) and CA19-9 (39.4 ng/mL, reference value: 0–37 ng/mL) levels. Gastroscopy showed that the gastric mucosa was smooth from the cardia, the mucosa of the gastric fundus was hyperemic with edema, and there was no erosion or ulcers.
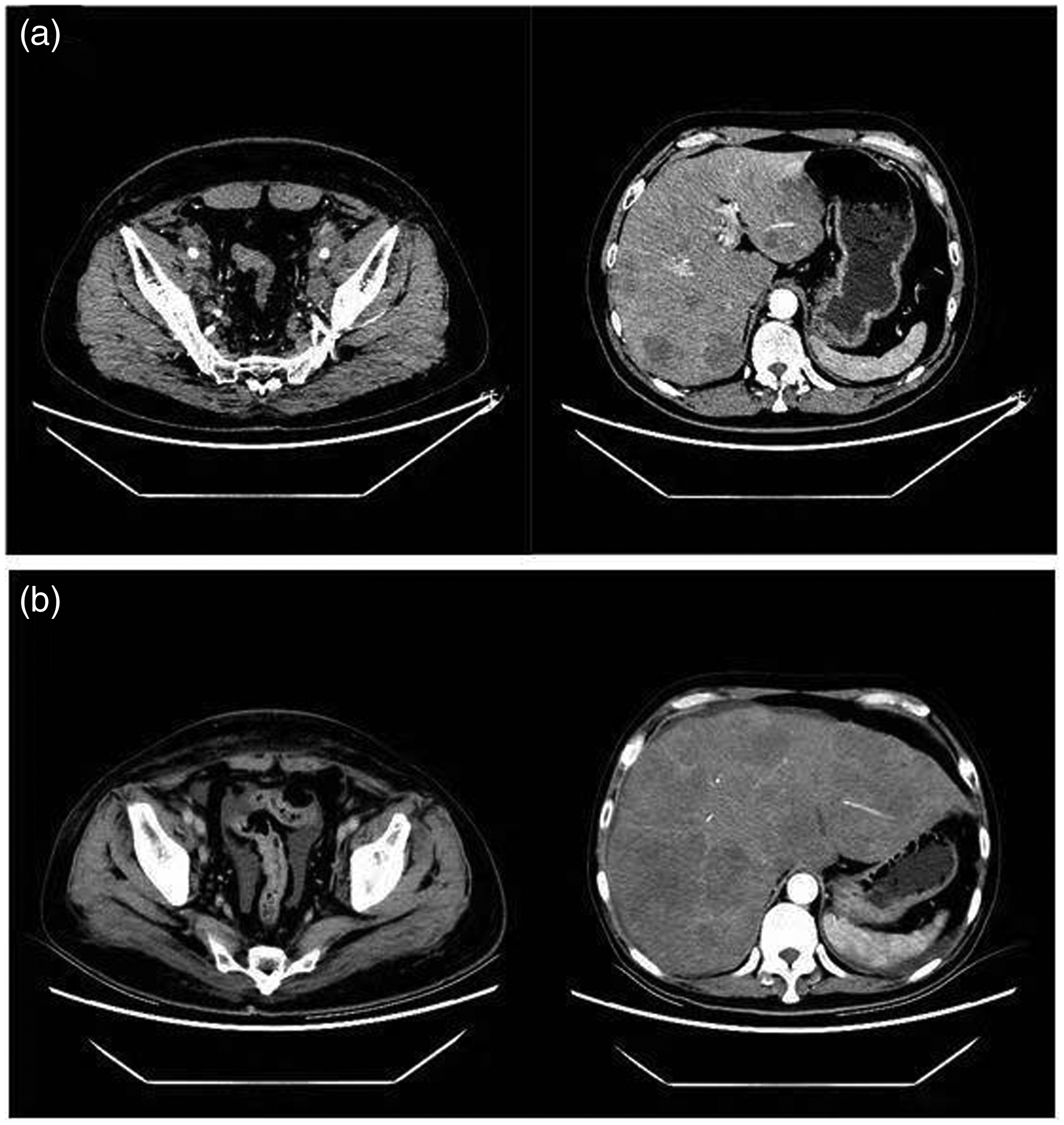
Imaging dates of the primary sigmoid colon lesion and liver metastases. (a) At the time of diagnosis and (b) Eight months after diagnosis.
Chronic non-atrophic gastritis was diagnosed on the basis of the mucosa of the gastric antrum being red and white and the pylorus orifice being smooth and well contracted. Subsequent colonoscopy found irregular lumps 17 to 20 cm from the anal margin, an uneven surface, hyperemia, edema, erosion, and bleeding from an easy touch (Figure 2). A pathological biopsy was taken, and the results showed adenocarcinoma with medium to low differentiation. Under the microscope, the tumor tissues were arranged in the shape of glandular tubules and sieve strips. The tumor cells were heteromorphic, with large and deeply stained nuclei, a dysplastic nuclear-to-cytoplasm ratio, and coarse and granular nuclear chromatin. Some tumor cells had rich and lightly stained cytoplasm, while others had translucent cytoplasm and no obvious nucleoli (Figure 3), which was confirmed by the pathologist as typical for adenocarcinoma after serum AFP levels were known. Gene detection showed no expression of PD-L1, MSS type, KRAS mutant type, and both NRAS and BRAF were wild type. Imaging of the patient’s liver displayed multiple patchy low-density shadows, an enhanced posterior margin, and part of the nodes presented the “bovine eye sign.” Radiologists at our hospital confirmed that the nodes of patient’s liver were metastatic tumors, not primary lesions. As the clinical stage of the patient was T2N2bM1b (IVB) according to the National Comprehensive Cancer Network guidelines and Chinese Society of Clinical Oncology guidelines, the patient agreed to receive anti-tumor therapy (bevacizumab 500 mg day 0 + oxaliplatin 0.2 g day 1 + capecitabine 1.5 g twice daily orally on days 1–14) for three cycles. After full communication, we reviewed the patient’s tumor markers: AFP 439.4 ng/mL, CEA 4.3 ng/mL, and CA19-9 16.5 ng/mL.

Colonoscopy report. Irregular lumps can be seen. The surface is uneven; hyperemia, edema, and erosion are present, and bleeding occurs at a light touch.
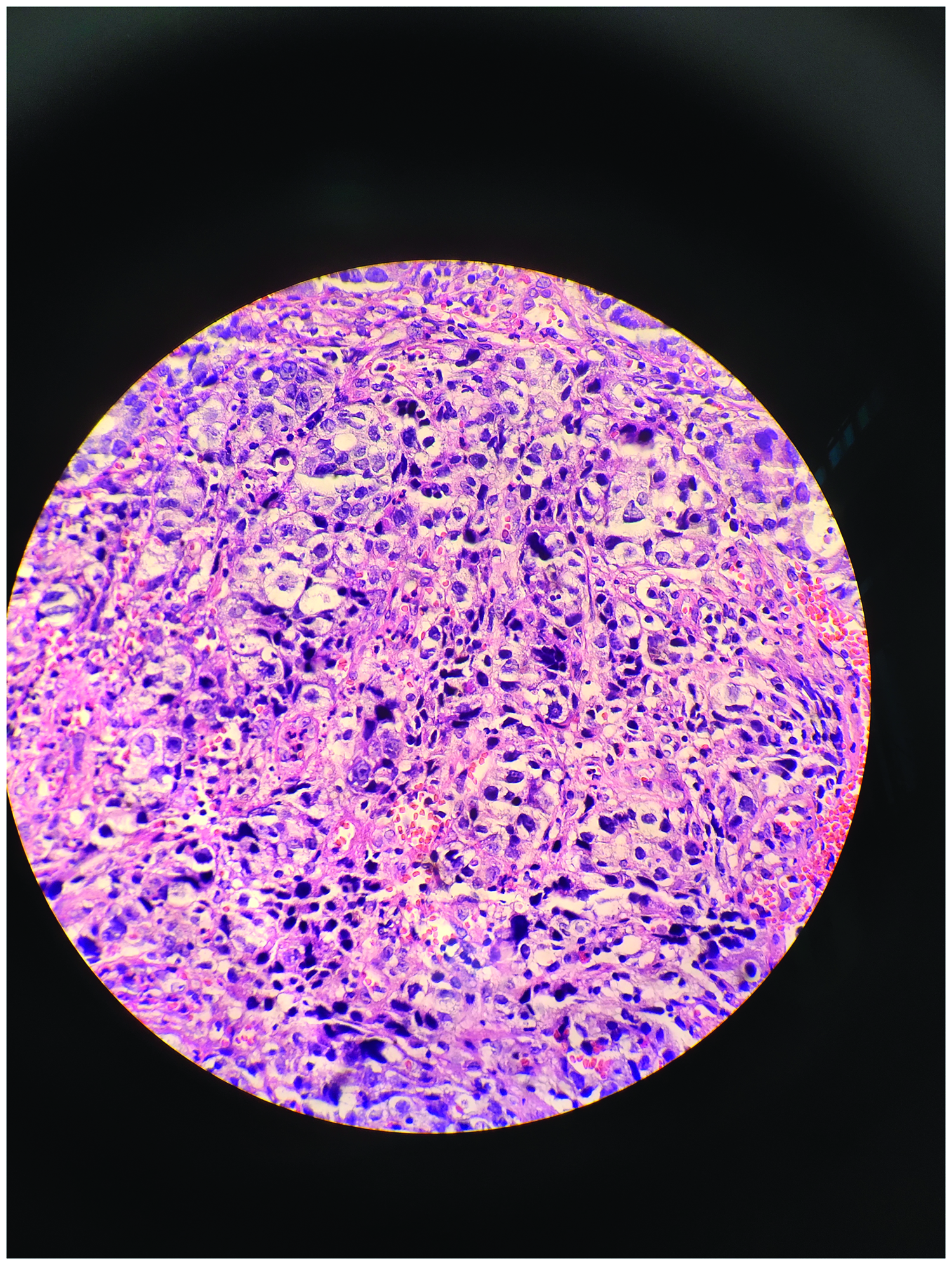
Biopsy findings. Common adenocarcinoma with low differentiation (hematoxylin and eosin staining, magnification 400×).
New lesions in his liver were found in chest and abdomen computed tomography examinations. According to the RECIST criteria, the efficacy was assessed as progressive Disease (PD). With the consent of the patient, we change treatment to a second-line regimen that was applied to for four cycles (bevacizumab 500 mg day 0 + irinotecan 280 mg day 1 + diageo 60 mg twice daily day 14). After two cycles, data from imaging examination showed the efficacy to be evaluated as stable disease (SD). After four cycles of second-line treatment, chest and abdominal computed tomography examination found disease progression, with the primary manifestations being enlargement and increased numbers of metastatic tumors in the liver, continuously increasing trend of AFP (963 ng/mL) (Figure 4), and severe anemia (hemoglobin 66 g/L). Transfusion of leucocyte-free suspended erythrocytes was given, and the treatment regimen was considered to be changed to targeted therapy (Igofenib), but the patient refused. The patient received only over-the-counter drugs for personal use after discharge. Eight months after his diagnosis, the patient was admitted to the hospital due to “fatigue and abdominal distension for more than half a month.” Computed tomography examination of the chest and abdomen showed multiple new nodules in both lungs, which were considered metastases; multiple intrahepatic metastases, larger and more numerous than before (Figure 1b). Incredibly, his serum AFP levels were 11,371.8 ng/mL at that time. Because the patient was a poor candidate for any intervention, he was accepted to hospice until death, with an OS of more than 9 months. We have de-identified all patient details in the article such that the identity of the patient cannot be ascertained in any way. The reporting of this study conforms to CARE guidelines. 14

Trends of tumor markers.
Discussion
In this report, we describe a rare case of an AFP-producing colorectal cancer. Tumor markers can be any molecules synthesized or released by tumor cells themselves or produced or elevated by the body in response to tumor cells. CEA plays an important role in colorectal cancer screening, diagnosis, efficacy evaluation, and regular follow-up 15 and has been recommended by domestic and foreign colorectal cancer guidelines. However, in our case, the elevated levels of CEA and CA19-9 were not clinically significant at the time of diagnosis, and no corresponding changes were observed during subsequent treatment, although the tumor continued to progress. However, serum AFP levels were positively correlated with tumor progression.
Although abnormal elevation of serum AFP is common in primary hepatocellular carcinoma or yolk sac carcinoma, it has also been reported to occur in malignancies of the lungs, 16 ovaries, 17 kidneys, 18 and esophagus. 19 AFP-producing tumors occurring in the gastrointestinal tract are mainly located in the stomach. The study by Kong et al. showed gastric cancers accounted for 83.1% of such malignancies, 20 although this only represents 1.3% to 15% of all gastric cancers. 21 The reason for this situation may be that AFP-producing tumors are primarily derived from organs originating from the foregut endoderm. 22 However, this patient was diagnosed with non-atrophic gastritis by gastroscopy, and a malignant tumor of gastric origin was excluded. AFP-producing colorectal cancers are rare, accounting for less than 1% of colorectal cancers. 23 Possible reasons for this might be that colorectal tissues originate from the hindgut endoderm. Ren et al. divided AFP-producing colorectal cancer patients into three histologic types: common adenocarcinoma type, mucinous adenocarcinoma type, and hepatoid type, in which common adenocarcinoma was the most common, 24 which is consistent with the pathologic pattern of our patient. AFP expression in tumor tissues is not strictly associated with serum AFP or hepatoid differentiation. 20 However, there is no uniform standard for the diagnosis of this type of colorectal cancer. Currently, diagnosing this type of colorectal cancer tends to rely on serum AFP levels.
In their study of 104 gastric cancer cases, Liu X et al. found that serum AFP levels were closely related to tumor liver metastasis. 25 Serum AFP levels can also be used as a prognostic indicator for AFP-producing gastric cancer. 26 Ren et al. 24 found that a diagnosis of this type of colon cancer was usually accompanied by multiple lymph node and distant metastases, with the liver being the most common site of visceral metastasis. The study by Kong et al. 20 showed that for cases with AFP ≥200 ng/mL at diagnosis, there is a high probability of stage IV disease, liver metastasis, large masses, and a high proportion of hepatoid adenocarcinoma. Moreover, liver metastasis is an independent prognostic factor for this type of colorectal cancer. In our case, AFP was 214.3 ng/mL at the time of diagnosis, with systemic and hepatic metastases, poor response to multi-line standard treatment, strong tumor invasion, and continuous progression. Other tumor markers could no longer express tumor load, and only serum AFP levels continued to rise, consistent with the disease progression.
Owing to the low incidence of AFP-elevated colorectal cancer, cases in the literature are generally from retrospective analyses, and there have been few studies on the pathogenesis of such cases. Therefore, there is currently no targeted treatment, but a standard treatment is referred to. Li et al. 10 also found that AFP-elevated colorectal cancer was resistant to a variety of chemotherapeutic agents, including VEGFR inhibitors. Local hepatic chemoembolization may be an effective treatment for liver metastases. Because this patient was diagnosed with stage IV disease with multiple liver metastases, lymph node metastasis, bone metastasis, and the gene test results suggested that the patient had MSS/KRAS mutations, NRAS/BRAF wild type, we chose the first-line chemotherapy regimen of bevacizumab + oxaliplatin +capecitabine. Unfortunately, the patient’s condition progressed after three cycles. Irinotecan was chosen as the main chemotherapy drugs for the second-line regimen. After two cycles of cross-line treatment with bevacizumab, the patient’s condition was stable, but progressed again after four cycles of treatment. We recommended the patient to switch to a third-line regimen, but the patient refused and died after only 2 months of treatment interruption, which suggests a poor prognosis. It is possible that there are still ambiguous signaling pathways that are activated in such patients, on which traditional therapies have poor effects. More research is needed and expected in this area.
Conclusion
Herein, we presented the case of an AFP-producing colorectal cancer, which is a rare tumor type. The patient presented with serum AFP levels >214.3 ng/mL, liver metastasis, multiple lymph node metastases, and bone metastasis. The tumor showed poor responses to standard chemotherapy and anti-angiogenic therapy, as continuous tumor progression was observed. The final OS was just 9 months. Therefore, special treatment strategies might be needed for this unique tumor type.
Abbreviations
Alpha-fetoprotein; Carcinoembryonic antigen; Carbohydrate antigen 19-9; Progression-free survival; Overall survival; Progressive disease; Stable disease.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221117218 - Supplemental material for Alpha-fetoprotein-producing advanced colorectal cancer: a rare case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221117218 for Alpha-fetoprotein-producing advanced colorectal cancer: a rare case report and literature review by Huan Ding, Shan Xu, Kang Wang, Xin Wang, Guanxing Sun, Xiang Li, Yancui Ran and Jinjun Sun in Journal of International Medical Research
Footnotes
Acknowledgements
We sincerely thank the department of pathology and radiology at our hospital for providing information. We are also very grateful to Dr. Meiqing Qiu in our hospital for her help in revising the article.
Author contributions
Huan Ding and Shan Xu wrote the manuscript and acquired patient information. Kang Wang, Xin Wang, and Guanxing Sun performed the literature review and follow-up. Xiang Li and Yancui Ran were responsible for the acquisition and analysis of imaging data. Jinjun Sun revised the manuscript. All authors have read and approved the final manuscript.
Availability of data and materials
All information about the patient came from the Department of Oncology, Zaozhuang Municipal Hospital. The data used and analyzed during the current study are included in this article.
Consent for publication
Oral consent for the publication of this case report was obtained from the patient's guardian.
Declaration of conflicting interest
All authors declare that they have no competing interests. All authors have confirmed no support from any organization for the submitted work, no financial relationships with any organization that might have an interest in the submitted work in the previous 3 years, and no other relationships or activities that could appear to have influenced the submitted work.
Ethics approval and consent to participate
Not applicable. This article describes a case report, a non-clinical trial, and the treatment regimen of the patient was carried out in accordance with the CSCO guidelines, without need for approval of the ethical review committee.
Funding
This case report was not supported by relevant funds.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.