
Abstract
Background:
Factors that influence quality of life (QoL) are used to determine the burden of disease, risk factors, and monitor management.
Objectives:
This study investigated the Australian inflammatory bowel disease (IBD) population and factors that affect QoL.
Design:
A national online survey was available to Australian IBD patients. Respondents were required to have a medical diagnosis of Crohn’s disease or ulcerative colitis, over 18 years of age, and receive healthcare in Australia.
Methods:
A mixture of validated questionnaires and additional questions were utilized to assess disease activity, QoL, and depression, anxiety and stress levels as well as demographic information. A variety of nonparametric statistical tests were used to explore relationships and compare groups.
Results:
A total of 825 participated in the survey across Australia with a 75% completion rate. The median Crohn’s and Ulcerative Colitis Questionnaire-8 (CUCQ-8) score was 37 with higher scores indicating worse QoL; those who have access to local support networks (Md = 36) had significantly lower CUCQ-8 scores compared to those who do not (Md = 44), U = 38,178, p = 0.014, r = 0.1. Similarly, those who feel adequately supported by local networks (Md = 35) had significantly lower CUCU-8 compared to those who do not (Md = 48), U = 30,772, p < 0.001, r = 0.21. Furthermore, perceived adequate support was associated with higher levels of QoL and lower levels of psychological stress. Heightened levels of psychological stress were associated with reduced QoL and increased disease activity.
Conclusion:
Support networks are essential to improve QoL. Local support networks may reduce psychological stress, improve disease activity, and enhance QoL. Management strategies are inadequate to minimize the decline in QoL when disease activity is heightened; therefore, the integration of adequate local support networks may be beneficial to assist management for Australians with IBD.
Introduction
Inflammatory bowel diseases (IBDs), specifically Crohn’s disease (CD) and ulcerative colitis (UC), are chronic gastrointestinal disorders characterized pathologically by intestinal inflammation.1,2 Throughout the 21st century, the prevalence of this disease is estimated to continue to rise worldwide. 3 In Australia, only a few epidemiological studies have predicted the prevalence of IBD.4–6 Recently, the prevalence of 653 per 100,000 Australians living with IBD was reported with this being almost double the previously reported data estimating Australia’s IBD prevalence.6,7 Despite the lack of continuous and historical data, Australia’s IBD prevalence is recognized to be among the highest worldwide. 8 Moreover, the higher prevalence translates to a higher burden of disease within individual countries. 3 Accordingly, additional information surrounding the IBD population is important to provide accurate data about the magnitude of the problem for each country.
Measures of quality of life (QoL) capture the well-being of the population 9 and are utilized to determine the burden of disease, associated risk factors, and assist in monitoring and management progression. QoL measures are particularly important for people with IBD as they live with a chronic, disabling disease that is likely to impact their physical, psychological, and social well-being. 10 Debilitating symptoms associated with IBD, such as abdominal pain, diarrhoea, cramps, rectal blood loss, and fatigue, 11 have a direct physical impairment on the individual; this can impede daily activities, hinder education and affect work production.12–14 Consequently, this contributes to psychological distress with interpersonal relationships, social participation and mental well-being affected. 13 Specifically, the psychological burden of IBD is distinguished through an increased number of patients with depression, one-in-four, and anxiety, one-in-three, like symptoms in remission. 15 Given the physiological and psycho-social outcomes of IBD, it is no surprise that manifestations of this gastrointestinal condition affect QoL.
The burden of disease is further highlighted with substantial financial and economic costs for the individual, society, and healthcare system. In 2012, an Australian-based report estimated over $380 million was attributed to IBD-related productivity losses; a further $2.7 billion was associated with the management of IBD. 14 Similar economic costs are observed in a Canadian study with an estimated $2.8 billion 16 ; higher indirect costs were estimated in the United States with $3.8 billion attributable to IBD. 17 With the number of IBD patients anticipated to increase, the direct and indirect costs will continue to grow for individuals, society, and healthcare systems, thus increasing the economic burden.
Identifiable factors that affect QoL among the IBD demographic may have the ability to direct and expand management interventions to reduce the decline of QoL. While limited, previous Australian-based studies have concluded that IBD significantly impairs QoL, 18 with malnutrition being associated with poorer QoL, 19 and disease activity correlating with reduced QoL.20–22 Additional research is required to investigate factors that influence QoL among the Australian IBD population.
Measures of QoL are essential for people who suffer from chronic or debilitating diseases. The information provided by QoL questionnaires should direct management, and lead to modifications and improvements in healthcare. The combination of demographic characteristics and QoL among Australians with IBD warrants investigation to identify specific factors that affect well-being. Country-specific research is important to provide accurate data and information about the disease in that country. New and continual research surrounding the Australian IBD demographic and QoL remains essential to prioritize treatment provision. Therefore, the purpose of this study was to explore the Australian IBD demographic, identify factors that influence QoL and health status as well as the correlation with disease activity. We hypothesized that socio-economic factors and social support will be significantly associated with QoL. Additionally, an increase in disease activity will be correlated with a reduction of QoL and increased psychological stress.
Methods
Study design
The national survey was developed using a mixed-method approach with closed and open questions. The survey was designed to capture the Australian IBD population and took approximately 15 min to complete (see Supplemental Appendix 1). The electronic survey was hosted on the online forum SurveyMonkey (https://www.surveymonkey.com/) between 31 March and 7 December 2022. Survey responses were strictly anonymous. The reporting of this study adheres to the Checklist for Reporting Results of Internet E-Surveys statement (see Supplemental Appendix 2). 23 The survey comprised of five sections: demographic information, disease activity, QoL and health status, perspectives on management, and physical activity participation. This paper will report on demographic characteristics, QoL, health status, and disease activity.
Recruitment and participants
For participant recruitment, Australian IBD support groups were contacted to share the survey on their websites, social media online platforms and/or membership newsletter; Crohn’s and Colitis Australia (CCA), a not-for-profit organization, elected to do so. In addition, recruitment occurred through advertisements in print media such as posters, as well as electronic media platforms. Finally, word of mouth was used to promote the study.
Questionnaires
Following confirmation of diagnosis, participants completed a series of validated questionnaires regarding their disease activity, QoL, depression, anxiety and stress levels, as outlined below. Additional questions were utilized to understand their demographic, perspectives on management, and physical activity participation.
(1) Harvey–Bradshaw Index (HBI) is a five-item questionnaire measuring disease activity for CD. 24 A cumulative score is utilized to identify disease activity: <5 remission, 5–7 mild, 8–16 moderate and >16 severe. 25
(2) Simple Clinical Colitis Activity Index (SCCAI) is a six-item questionnaire measuring disease activity for UC 26 with a cumulative score to identify disease activity: <5 remission and ⩾5 relapse. 27
(3) QoL was assessed through Alrubaiy, Cheung 28 Crohn’s and Ulcerative Colitis Questionnaire-8 (CUCQ-8). Responses were scored 0–3 on a Likert scale and 0–14 for closed-ended questions. The score range is 0–90 with the higher score indicating a worse QoL.
(4) Lovibond and Lovibond 29 depression, anxiety and stress scales 21 (DASS-21) was used to analyse the three subscales: depression, anxiety and stress. Each subscale is measured through the combined scores of seven questions: items 3, 5, 10, 13, 16, 17 and 21 to analyse depression; items 2, 4, 7, 9, 15, 19 and 20 contribute to anxiety scores; and items 1, 6, 8, 11, 12, 14 and 18 for stress scores. Four-point Likert scales ranging from 0 to 3 were used for each of the 21 questions. DASS-21 scores are categorized into normal (depression: 0–4; anxiety: 0–3; stress: 0–7), mild (depression: 5–6; anxiety: 4–5; stress: 8–9), moderate (depression: 7–10; anxiety: 6–7; stress: 10–12), severe (depression: 11–13; anxiety: 8–9; stress: 13–16) and extremely severe (depression: 14+; anxiety: 10+ and stress: 17+).
Data analysis
Descriptive statistics were calculated for all demographic and clinical variables. Continuous data were described by median and interquartile ranges (IQR). Categorical variables were described by frequencies (%). Nonparametric statistical tests were used to explore relationships or compare groups as data did not meet the assumptions of the parametric techniques, specifically the distribution of the data set. Spearman’s rho correlation coefficient was used to explore relationships between two continuous variables and χ2 was used to explore the relationship between two categorical variables. To compare the relationship between one categorical independent variable and one continuous dependent variable, both the Mann–Whitney U test (two groups only) and the Kruskal–Wallis test (three or more groups) were used. The sample size was calculated on an online calculator provided by SurveyMonkey (https://www.surveymonkey.com/mp/sample-size-calculator/); this resulted in a total sample of 384 respondents required. A p value of <0.05 was considered statistically significant. Statistical analyses were performed using Statistical Package for the Social Sciences (IMB SPSS Statistics for Windows, Version 27.0, Armonk, NY, USA).
Results
Participant characteristics
There were 825 respondents to the survey with a 75% completion rate. Demographic characteristics for all respondents are presented in Table 1. The number of respondents diagnosed was evenly distributed between the two primary disease entities with 420 (50.9%) diagnosed with CD and 405 (49.1%) with UC. In general, the frequency distribution of the two groups was similar in demographic characteristics. The median age of respondents was 40 years (IQR = 32–49) with the majority being female (82.7%). The median age of diagnoses was 27 years (IQR = 20–35.50) with the median age of CD being slightly younger at 25 years (IQR = 19.75–33) compared to UC at 30 years (IQR = 22–37). Less than 1% of the respondents do not have access to support networks available in their local health district.
Demographic characteristics (number of responders).

IBD, inflammatory bowel disease.
Disease activity
Clinical characteristics are presented in Table 2. The HBI ranged from 0 to 26 with a median score of 5 (IQR = 2–8). A total of 47.8% of CD respondents (n = 379) were in remission, 23.5% had mild disease, 26.1% had moderate disease and 2.6% had severe disease. Alternatively, the median score of the SCCAI was 4 (IQR = 2–6) ranging from 0 to 17; 60.9% of UC respondents (n = 379) were classified to be in remission and 39.1% were in a relapse period.
Clinical characteristics (number of responders).

CUCQ-8, Crohn’s and Ulcerative Colitis Questionnaires-8; HBI, Harvey–Bradshaw index; IQR, interquartile range; SCCAI, Simple Clinical Colitis Activity Index.
Perceived stress
The median score of perceived stress, measured through the DASS-21 stress scores, was 7 (IQR = 3–10), with both diseases, CD and UC, reflecting this score. A total of 57.6% of IBD respondents were experiencing normal levels of stress, while 14.4% had mild levels, 12.5% had moderate levels, 11% had severe levels and 4.5% were experiencing extremely severe levels.
Health status and QoL
Table 3 displays the extent to which respondents indicate IBD has negatively impacted their health status with the most reported IBD-related issue. Furthermore, respondents indicated two main factors surrounding IBD that have impacted their mental and/or emotional health; they were fatigue and sleep quality (n = 368) and disruption to usual life activities (n = 245). The burden of management (n = 161) and social and interpersonal functioning (sexuality, intimacy and body image satisfaction) (n = 179) followed.
Questions (number of responders).
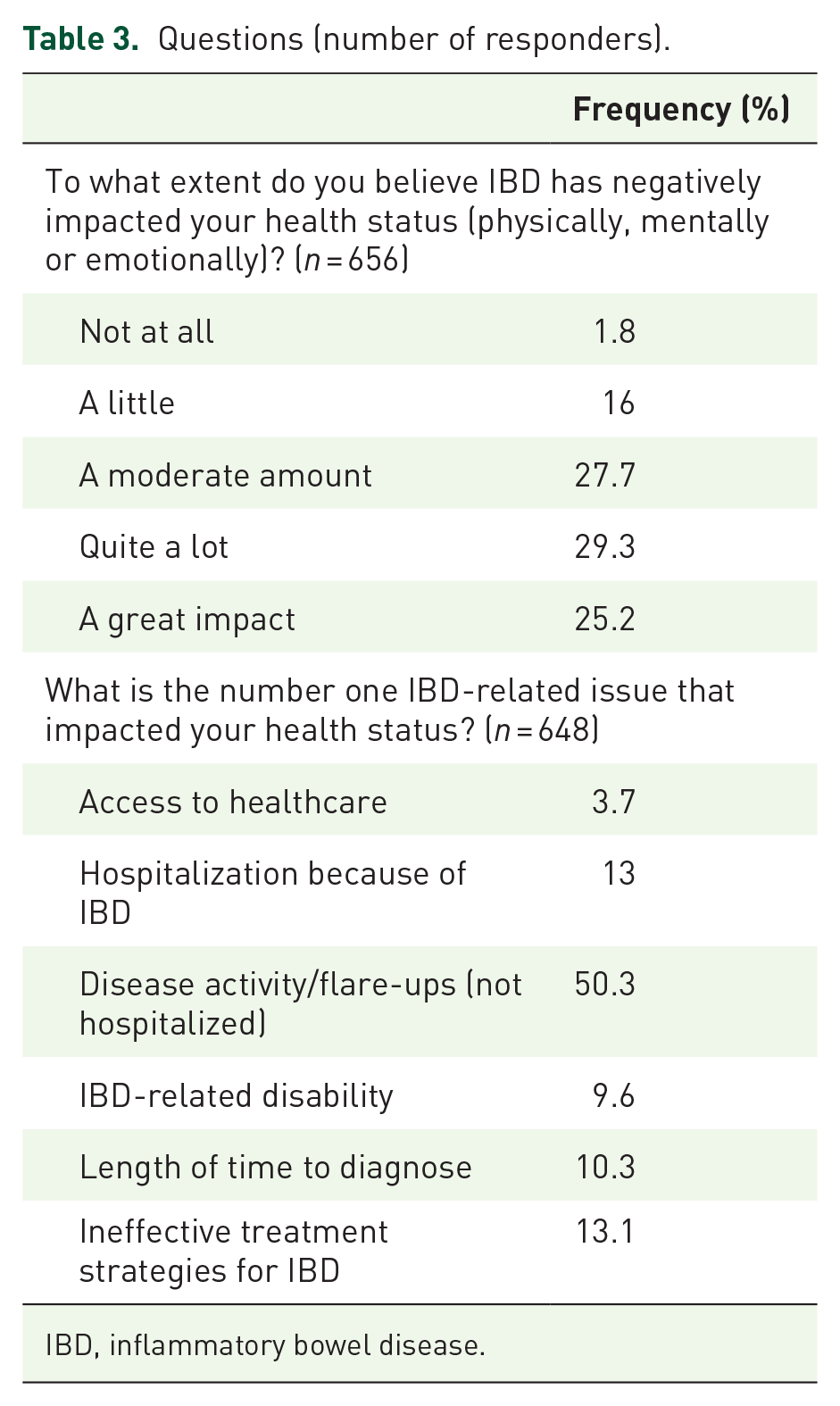
IBD, inflammatory bowel disease.
The median score of CUCQ-8 was 37 (IQR = 22–55.50) ranging from 0 to 90; higher scores indicate worse QoL. This clinical characteristic is presented in Table 2. There was no significant difference in CUCQ-8 scores between CD (Md = 37, n = 334) and UC (Md = 37, n = 331), U = 55,977, p = 0.777, r = 0.06. Therefore, the following analyses combined CD and UC CUCQ-8 scores.
The extent that one has perceived their health status was impacted by IBD revealed significantly higher CUCQ-8 scores indicating a worse QoL χ2 (4, n = 655) = 150.867, p < 0.001. A pairwise comparison with Bonferroni correction revealed majority of groups (Gp1, n = 12, not at all; Gp2, n = 105, a little; Gp3, n = 182, a moderate amount; Gp4, n = 192, quite a lot; Gp5, n = 164, a great impact) had significant difference between them (p < 0.001) except for Gp1 (not at all) and Gp2 (a little).
Relationship between QoL, health status and demographic characteristics
As presented in Figure 1, statistically significant differences in CUCQ-8 scores included: (a) those who have access to local support networks compared to those who do not; (b) those who feel like they are adequately supported by local networks and those who do not and (c) the perceived effectiveness of medication. Despite patients who were diagnosed within 2 years, scored higher CUCQ-8 scores (Md = 43) indicating a worse QoL, no significant difference was identified across CUCQ-8 scores and length of diagnosis. Similarly, there is no significant difference between CUCQ-8 scores and age of diagnosis, marital status, or education. The geographical location did not impact CUCQ-8 scores for kilometres (kms) travelled for treatment, hours travelled for treatment, residual state, or remoteness areas. In addition, there is no significant difference between QoL and the number of support groups.
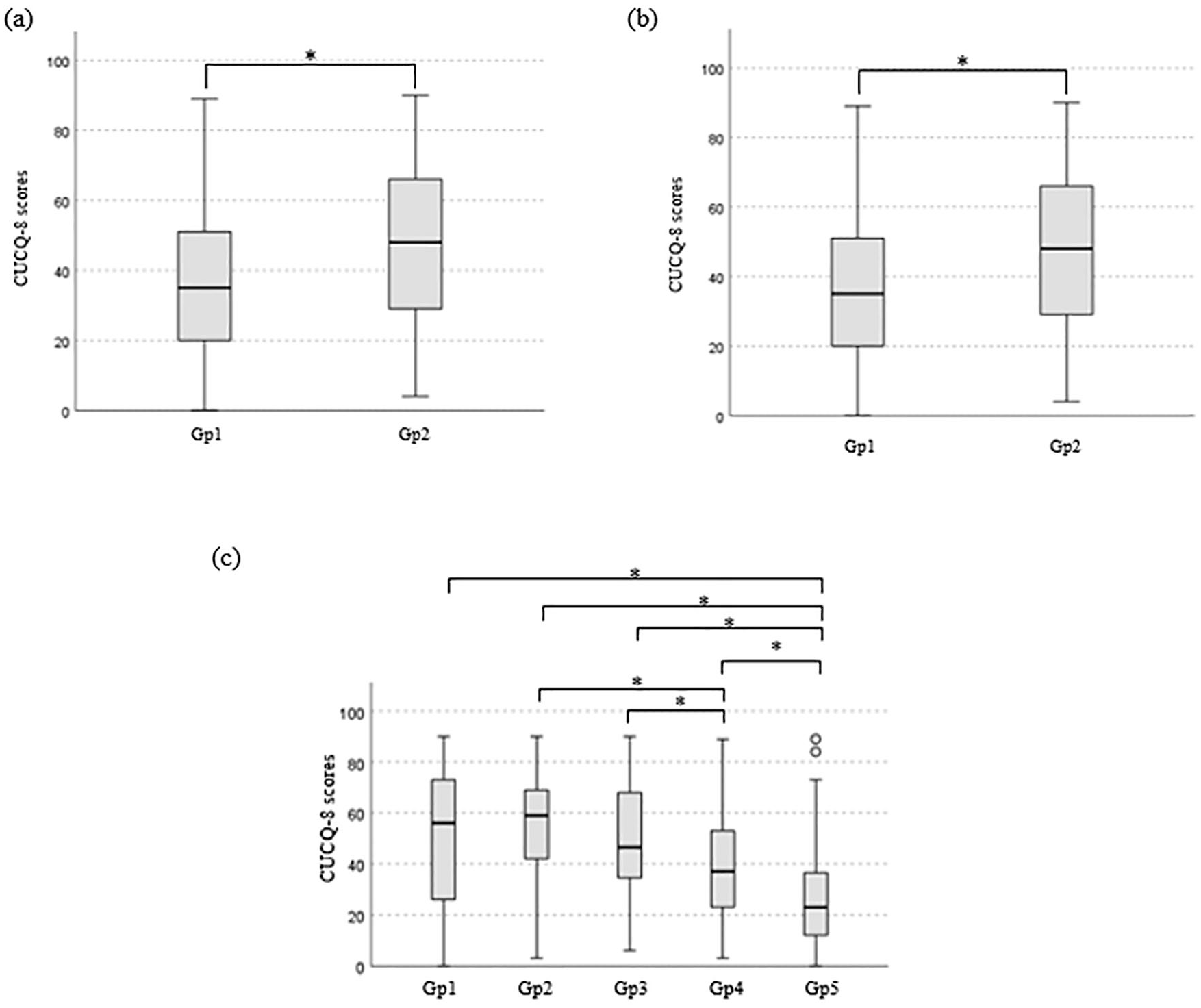
A statistically significant difference in CUCQ-8 scores for (a) those who have access to local support networks (Gp1, Md = 36, n = 504) compared to those who do not (Gp2, Md = 44, n = 133), U = 38,178, p = 0.014, r = 0.1; (b) those who feel like they are adequately supported by local networks (Gp1, Md = 35, n = 377) and those who do not (Gp2, Md = 48, n = 127), U = 30,772, p < 0.001, r = 0.21 and (c) perceived effectiveness of medication (Gp1, very ineffective, n = 25; Gp2, ineffective, n = 65; Gp3, n = 108, indifferent – neither effective nor ineffective; Gp4, effective, n = 308; Gp5, very effective, n = 123), χ2 = (4, n = 629) = 104.048, p < 0.001.
There was a significant association between feeling adequately supported and perceived impact of IBD on one’s health status, χ2 (3, n = 504) = 23.274, p < 0.001, Cramer’s V = 0.215; while there was no significant association between access to local support networks and perceived impact on one’s health status χ2 (3, n = 638) = 6.190, p = 0.103, Cramer’s V = 0.099.
Relationship between QoL, disease activity, psychological stress and perceived support
The relationship between disease activity and QoL was investigated using Spearman’s rho correlation coefficient. Preliminary analyses were performed to ensure no violation of the assumptions. There was a strong, positive correlation between the two variables for both CD (rho = 0.724, n = 334, p < 0.001) and UC (rho = 0.740, n = 331, p < 0.001) with high levels of disease activity associated with worse levels of QoL. Disease activity helps to explain approximately 50% of the variance in respondents scores on the CUCQ-8 scale (CD r2 = 52.4%; UC r2 = 54.8%). The heightened level of disease activity recorded significant higher median CUCQ-8 scores indicating worse QoL; this is presented in Figure 2.

A statistically significant difference in CUCQ-8 scores across disease activity categories: (a) Harvey–Bradshaw Index scores (Gp1, n = 153: remission, Gp2, n = 81: mild disease; Gp3, n = 91: moderate disease; Gp4, n = 9: severe disease), χ2 (3, n = 334) = 144.697, p < 0.001; (b) Simple Clinical Colitis Activity Scores (Gp1, remission, Md = 29.50, n = 204; Gp2, relapse Md = 59, n = 127), U = 22,567, p < 0.001, r = 0.624 and (c) received stress levels (Gp1, n = 356, normal; Gp2, n = 89, mild; Gp3, n = 77, moderate; Gp4, n = 68, severe; Gp5, n = 27, extremely severe), χ2 (4, n = 617) = 63.698, p < 0.001.
There was a small, positive correlation between those with IBD and perceived stress (rho = 0.356, n = 665, p < 0.001) with high levels of perceived stress associated with worse QoL. Perceived stress helps to explain a small variance in respondents’ scores on the CUCQ-8 scale (r2 = 12.7%). Upon further analysis, those with CD had a slightly less correlation between the two variables (rho = 0.301, n = 313, p < 0.001, r2 = 9%) compared to those with UC (rho = 0.405, n = 304, p < 0.001, r2 = 16.4%). Those who were experiencing lower levels of stress had lower CUCQ-8 scores, indicating better QoL. The significant difference is presented in Figure 2. There was a statistically significant association between disease activity and psychological stress: CD, χ2 (8, n = 314) = 25.279, p = 0.001, Cramer’s V = 0.201; UC, χ2 (4, n = 304) = 34.679, p < 0.001, Cramer’s V = 0.338. A Chi-square test for independence revealed a statistically significant association between those who perceived support was adequate and psychological stress, χ2 (4, n = 480) = 10.381, p = 0.034, Cramer’s V = 0.34.
Discussion
The purpose of this study was to examine a sample of the Australian IBD demographic and investigate factors that affect QoL and health status. The novel finding of our study is social and local support networks significantly increase QoL. Adequate support was associated with higher levels of QoL and lower levels of psychological stress. Unlike the significant association observed through social support, the socio-economic factors measured in this study were not associated with QoL; therefore, these results were partially consistent with our hypothesis. An additional finding of this study, consistent with our second hypothesis, was levels of psychological stress were associated with reduced QoL and increased disease activity. The most important IBD-related issue that impacted health status was disease activity/flare-ups that did not require hospitalization. Country-specific data are essential for management evaluation, management progress, and future direction for healthcare providers. This study analysed patient’s perspectives to understand the impact IBD has on Australians and to advocate for their needs. This evidence will assist the quality of care available with continual research required to enhance Australian-based resources.
Timely access to healthcare professionals is essential to initiate interventions when the disease becomes acutely active. 30 As anticipated, our findings revealed the ability to access local IBD support networks such as general practitioners (GPs), specialists, or other medical staff, significantly increased QoL among Australians with IBD. Often, improvements associated with IBD are geographically dependent with untimely access to care identified as a critical challenge for the IBD community. 16 However, these results showed geographical location including distance travelled for treatment, residential state, or remoteness, did not influence QoL in Australia. In contrast with the known health inequalities of rural living and access to healthcare services, 31 this unexpected outcome does not indicate equal care throughout Australia for those living with IBD. Rather, the results suggest that access to management through local networks could be a key component to improve QoL and reduce the burden of disease.
In addition, the findings highlight that not all individuals with access to support from local networks actually felt adequately supported. In previous reports indicate that Australian medical care surrounding Crohn’s and colitis is inadequate and inconsistent,14,32 the present results are not surprising. Despite the individual variability of perceived support, the majority (74.8%) of participants felt adequately supported by local networks. This percentage of satisfaction with local care is similar to that previously associated with Australian IBD healthcare (74.8%). 33 With no observed improvement, and continual disparity established, interventions to minimize inconsistent levels of care are essential to ensure that quality disease management is provided to all Australians with IBD and further improve well-being.
Adequate support is essential to maintain mental health and improve QoL among the IBD demographic. It is theorized the belief that support is available buffers the effects of stress on health outcomes. 34 Known as the stress-buffering theory, 35 the interaction between perceived support, psychological stress, and QoL is observed in this study. The findings revealed that the perceived feeling of adequate support significantly improved QoL among Australians with IBD. Similar results are observed in previous work with perceived spousal support being associated with improved QoL 36 and lower perceived social support linked to diminished QoL. 37 Unlike the specific type of support measured in the previous studies,36,37 in this study, the term ‘support’ refers to that provided by hospitals and professional medical staff, as well as social support from family and friends. Although not analysed individually, and acknowledged as a limitation, this outcome could be attributed to the different aspects of support, their relationship with stress, and their impact on QoL.
Along with the evident relationship between perceived support and QoL, our results highlight the association between perceived support and perceived stress. A systematic review revealed similar outcomes with evidence to support the inverse relationship between social support and psychological distress. 38 In addition, Larsson et al. 39 identified emotional and instrumental support as the preferred types of social support for those with IBD, especially at the time of diagnosis or increased disease activity. Through emotional and instrumental support, the burden of disease could decrease and consequently, a reduction in psychological stress may occur. Furthermore, self-isolation has been suggested to have a crucial role in the prognosis of IBD. 40 Although the psychological pathways require additional research to link social isolation and disease progression, the importance of social support is apparent.
Social support may serve as a modifiable factor to improve psychological components of disease management38,41; specific modifiable factors include access to IBD nurse support, physician advice, 42 and the integration of psychological care into routine management. 43 Interestingly, the present findings indicate that the number of support networks does not influence QoL; rather, one quality support network is sufficient to improve QoL. This result may be attributed to the aforementioned relationship between social support and perceived stress. Continuous care through a variety of components may be influential in lowering the effects of stress. Therefore, specific support systems, including types of social support, and their relationship to psychological stress, must be identified among Australians with IBD to enhance well-being and disease management.
Another variable known to influence QoL among the IBD population is psychological stress44,45; our findings remain consistent with the literature as high levels of perceived stress were associated with worse QoL. To comprehend this relationship, the influence stress has on intestinal inflammation and disease exacerbation, and, consequently, QoL must be interpreted. Emerson et al. 46 highlighted the importance of monitoring subjective well-being in IBD clientele to identify psychological distress to predict disease progression, as psychological stress is associated with an exacerbation of IBD symptoms. 47 Results in this study demonstrate that increased levels of stress are associated with heightened levels of disease activity. Evidence has revealed psychological stress can induce a series of inflammatory responses that influence gut inflammation; more specifically, the stress-induced activation of mechanisms, such as hypothalamus–pituitary–adrenal axis and the autonomic nervous system, cause immunological and neuroendocrine changes that result in pro-inflammatory cytokines, activation of macrophages, and alter intestinal permeability and gut microbiota.48–51 Reductions in psychological stress are suggested to be an essential aspect of IBD to reduce disease exacerbation. 52 Therefore, monitoring well-being and psychological stress may be beneficial to manage and understand disease progression.
The negative effect that disease activity has on QoL has been previously investigated in IBD. 53 Our results support this notion as active disease, regardless of the severity, significantly impacted QoL. These results are consistent with previous research conducted in Australia that concludes disease activity correlates with reduced QoL.19–22 The unpredictable nature and severe symptoms that accompanies increased disease severity can substantially reduce QoL. 54 The present results, combined with prior literature, highlight the difficulties with disease management. Complementary or alternative management strategies warrant investigation to reduce the decline in QoL when disease activity increases. Lastly, this study revealed flare-ups that did not require hospitalization were the number one IBD-related issue that impaired respondents’ health status. Therefore, the need for disease management to extend beyond hospital care is apparent.
Limitations
This study has several limitations. First, the cross-sectional survey approach only collects a single moment in time; however, by identifying factors that influence QoL, other research methodologies should be used to observe and understand the physiological mechanisms support and stress have on disease activity and QoL. Second, data collection was conducted throughout the COVID-19 pandemic. During the pandemic, higher levels of psychological stress 55 and enforced social isolation 56 were lived experiences of IBD patients that escalated disease activity and declined subjective health; these aspects emphasize the importance of stress management and support systems to control IBD progression and reduce the decline of QoL. Third, despite our efforts to reduce selection bias, recruitment was largely attributed to CCA. For this reason, people who are part of the online community or spend more time on social media or the internet may have been more aware of the study. In regard to sharing through CCA, this allowed us to have a solid sample size. Fourth, 82.4% of respondents identified as female which may not accurately reflect the Australian’s IBD demographic; however, the gender distribution among the Australian IBD prevalence is unknown. In addition, online surveys usually obtain a much lower response rate in males participants compared to female participations. 57 Fifth, the disease-specific QoL scale, CUCQ-8, used in this study was an efficient tool to administer into the large questionnaire; however, a generic QoL questionnaires, such as Short-Form 36, 58 would have been beneficial to compare QoL across other population groups. Sixth, this survey did not use a validated scale for perceived social support. Therefore, additional research into social support should use a reliable scale to strengthen results such as the Multidimensional Scale of Perceived Social Support. 59 Last, specific support systems should be identified and evaluated in relation to QoL and disease activity to further assist Australians with IBD.
Conclusion
In conclusion, this study investigated factors that influence QoL among Australians with IBD. Local and social support systems were identified to significantly affect QoL. In addition, high levels of psychological stress were correlated with heightened levels of disease activity and worse QoL. The positive influence adequate perceived support has on QoL may be attributed to the stress-buffering theory which refers to the perceived availability of social support may reduce the effects stress has on QoL. Furthermore, the relationship stress has on QoL may be determined by the influence stress has on intestinal inflammation and exacerbation of IBD symptoms. Current management strategies for IBD are inadequate to minimize the decline in QoL when disease activity is heightened. The intertwined relationship of perceived support, psychological stress, disease activity, and QoL is apparent; therefore, social support systems ingrained into local networks may be beneficial for Australians with IBD to reduce psychological stress, and help control disease activity, thereby improving QoL.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848241264362 – Supplemental material for Living with inflammatory bowel disease in Australia: quality of life and the impact of support networks
Supplemental material, sj-pdf-1-tag-10.1177_17562848241264362 for Living with inflammatory bowel disease in Australia: quality of life and the impact of support networks by Kelly A. Baker, Frank E. Marino and Tegan E. Hartmann in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-2-tag-10.1177_17562848241264362 – Supplemental material for Living with inflammatory bowel disease in Australia: quality of life and the impact of support networks
Supplemental material, sj-pdf-2-tag-10.1177_17562848241264362 for Living with inflammatory bowel disease in Australia: quality of life and the impact of support networks by Kelly A. Baker, Frank E. Marino and Tegan E. Hartmann in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors would like to thank the respondents for participating in this survey and Crohn’s and Colitis Australia for making the survey widely available. The authors would like to acknowledge the Charles Sturt University Spatial Data Analysis Network that covers the cost of SurveyMonkey.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.