
Abstract
Background:
Crohn’s disease (CD) is a chronic autoimmune inflammatory bowel disease. It is estimated that approximately 40% of individuals with CD are non-adherent to medical prescriptions. This lack of adherence to treatment plans has been linked to an increased risk of hospitalisation and surgical procedures, which can have a detrimental impact on the patient’s quality of life (QoL). Furthermore, the CD can impose significant stress on individuals, affecting their mental health and sense of mastery. The term ‘mastery’ is used to describe an individual’s awareness of their abilities and capacities that are essential for effectively managing life events and situations.
Objectives:
This study aimed to investigate the role of mastery in relation to medical adherence, distress, perceived social support, QoL, depressive and anxious symptoms and interoception in persons with a diagnosis of CD.
Design:
This is a cross-sectional study, involving 261 adults diagnosed with CD.
Methods:
Participants completed an online questionnaire comprising validated clinical and psychological scales, which lasted approximately 20 min. Participants were permitted to provide their most recently available medical report.
Results:
Patients with CD reported discrete levels of mastery. Two factorial ANOVA highlighted statistically significative differences in mastery in relation to clinical conditions (F(2, 253) = 11.22, p < 0.001) and a significative interaction effect between gender and symptomatology (F(2, 253) = 7.22, p < 0.001). Multiple linear regression illustrated a statistically significant association between mastery, clinical conditions, QoL, stress and interoception (adjusted R square = 0.558; F(14, 211) = 21.32, p < 0.001). Concerning the possible mediator role of mastery between psychological state and medical adherence, no statistically significant results emerged from the mediation model analysis.
Conclusion:
This study highlighted an effective impairment of mastery in CD patients, especially among men experiencing mild disease activity. A positive association between mastery and enteroception was outlined. The higher prevalence of distress, anxiety and depressive symptoms connected to mastery was substantiated. Future research should deepen the relationship between mastery with medical adherence.
Plain language summary
Crohn’s disease (CD) is an inflammatory bowel disease with severe implications on patients’ quality of life, social relationships and mental health. Mastery is a psychological construct concerning the personal awareness of possessing skills to properly manage life events; that can mitigate the impact of a persistent disease. The present study aimed to investigate the role and the association of mastery in relation to quality of life, medical adherence, distress, perceived social support, depressive and anxious symptoms and enteroception in persons with a diagnosis of CD. People with CD reported discrete levels of personal master. Two factorial ANOVA outlined variations in mastery according to the participants’ gender and clinical conditions. Multiple linear regression indicated a significative influence of distress and interoceptive features on mastery. The results should encourage clinicians to pay attention to the identification of the most effective approaches to enhance mastery and consistency with clinical prescriptions in individuals with CD; also considering their psychological state and mental health.
Introduction
Crohn’s disease (CD) is a chronic, autoimmune, inflammatory bowel disease (IBD), with a typical progressive destructive course that often results in complications, hospitalisation and surgical interventions. 1 Clinical symptoms may range from mild to severe and include abdominal pain, severe diarrhoea, melena, chronic malabsorption, lesions of the intestinal wall and extra-intestinal manifestations such as stomatitis, uveitis, perioral dermatitis, glossitis and/or cheilitis. 1
The CD is a widespread condition with an overall rising incidence, probably due to industrialisation and westernisation.2,3 The prevalence of CD in Europe is estimated to range from 0.3 to 12.7 per 100,000 person-years, with the highest prevalence observed in Germany (322 cases per 100,000 person-years).2,3 In Italy, the prevalence is estimated to be approximately, 100 cases per 100,000 inhabitants, with an incidence of new patients per year is approximately 10.5 per 100,000 inhabitants. 4 These estimates, when considered alongside the course of the illness, indicate that the treatment of CD places a significant economic burden on the healthcare system, which may be further exacerbated by difficulties in medication adherence among patients.5 –7 Approximately 40% of individuals with CD do not comply with medical prescriptions, particularly due to concerns about adverse effects from medications. 6 Untreated CD results in increased rates of complications and hospitalisations, and may lead to disability outcomes, affecting patients’ quality of life (QoL). 6
Mental health comorbidities represent a further significant factor contributing to elevated healthcare costs and a reduction in QoL among individuals with CD. They are more prone to experiencing depression and anxiety disorders than the general population 7 with an estimated prevalence of comorbid conditions ranging from 30% to 50%. 8 Additionally, recent investigations into the gut–brain axis (GBA) have elucidated a bidirectional interplay between pain, stress, emotional states and the functionality of the gastrointestinal tract, including inflammatory relapse, in patients with CD.1,9 The activation of the enteric nervous system by psychological distress leads to an increase in proinflammatory cytokines, resulting in an exacerbation of symptomatology. 9 Such alterations in the GBA, in association with chronic exposure to visceral pain, may also affect interoceptive awareness (IAw), 10 defined as the sense through which physical changes are properly subjectively perceived. 11 Interoception is closely linked to emotional processing and may impact the severity of CD clinical manifestations, exacerbating perceived distress and heightening sensitivity to negative emotional stimuli. 12 Individuals with the disease must maintain heightened and selective attention to their body signals, to recognise the initial symptoms of flare-ups. 10 This is of particular importance given that chronic clinical relapses and increased awareness of these unpleasant body sensations impose significant stress, thereby eroding the individual’s sense of mastery and perceived control.13–15
The concept of mastery can be defined as a psychological construct that pertains to an individual’s personal awareness of their capacity to effectively navigate and manage various life events. 16 This awareness is influenced, to some extent, by the presence, persistence and severity of stressors in one’s life. 16 Mastery can be conceptualised as a psychological resource, given that elevated levels of the construct have the potential to attenuate the impact of persistent disease and to minimise the impact of functional decline, chronic pain and uncertainty.13,17 Moreover, mastery serves as a mediator between distress and mental health, both in disease and health conditions. 18 It is a considerable influence, given the frequently invalidated psychological state of people with CD.7,8
Lastly, social support has a pivotal role in the management of CD, especially because patients often experience social stigma and isolation due to their clinical manifestations.7,19
Despite the protective and beneficial features of mastery in chronic illness, even in preventing disabling outcomes,13,17 scientific literature has not deepened the construct of mastery and its possible interactions with other psychological aspects in people with CD.
Objectives
The present study aimed to investigate the role and the association of mastery in relation to medical adherence, distress, perceived social support, QoL, depressive and anxious symptoms and enteroception in persons with a diagnosis of CD.
In line with existing literature, the research aimed to examine the impact of gender and clinical conditions on the level of mastery experienced by patients. Additionally, the study sought to investigate whether the symptomatology, distress, QoL and IAw influence the level of mastery.1,7–10,13,20 Furthermore, the research explored the possibility of mastery as a mediator between psychological state (in terms of stress, anxiety and depressive feelings) and medical adherence.18,20
Ultimately, concerning a subsample, the research aimed to inspect the congruence between patients’ clinical prescriptions and their personal statements about medical adherence.
Methods
Study design
The research was structured as a cross-sectional study and followed the STROBE guidelines (STrengthening the Reporting of OBservational studies in Epidemiology) 21 (Supplemental Material S1 file).
Ethical consideration
The study was approved on the 27th of January 2023 by the Ethical Committee for Research in Clinical Psychology (CERPS) of Università Cattolica del Sacro Cuore in Milan, Italy. Anonymity was guaranteed by the removal of every reference to people and places’ sensible data in medical reports and by assigning alphanumeric codes. To accurately ascertain medical adherence, the survey requested that participants attach their most recent clinical report. It should be noted that the decision to attach the report was entirely optional and had no impact on the completion of the survey questionnaire, which was placed as the final question for this reason. The link between the medical report and the subject’s response was made possible by the generation of an alphanumeric code at the outset of the compilation, which was subsequently reported by the participant upon attachment of the file.
Sampling
The recruitment of participants commenced in February 2023, lasted until October 2023, and was conducted in accordance with the criteria for a convenience sample through the dissemination of advertisements on social networks, including but not limited to Facebook and Instagram, targeting individuals within patient groups with CD. The Italian National Association for Inflammatory Bowel Diseases assisted the enrolment process by spreading the advertisement through its official channels.
The sample size estimation was run employing G*Power statistical software.22,23 Considering feasibility, potential drop-out of 20%, the absence of literature on the field, and employing an α of 0.05, 1 − β (power) of 0.95, the total sample size needed was 175.
Inclusion and exclusion criteria
Subjects were eligible if they were diagnosed with CD and were over 18 years of age. Exclusion criteria were having a diagnosis of ulcerative colitis (the other most common IBD) and being underage.
Data collection
Instruments
The subjects who participated in the study completed an online questionnaire on the Qualtrics® platform (https://www.qualtrics.com), which lasted approximately 20 min and was presented to the participants only once. Prior to the administration of the questionnaire, each subject was required to provide online informed consent.
The first section of the survey involved questions related to participants’ demographic characteristics (i.e., gender, age, marital status, education, occupation, housing situation, presence and, in case, number of children, smoking and alcohol intake and physical exercise practised). Subsequently, the subject completed the following scales designed to detect each clinical and psychological aspect considered by the present research:
‘Harvey–Bradshaw Index’ (HBI): six items instrument administered for the assessment of the clinical condition and symptomatology of patients with CD 24 ;
‘Medication Adherence Report Scale-5I (MARS-5I)’: Italian validated version of the Medication Adherence Report Scale (MARS), 25 five-item scale employed for detecting medical adherence as reported by the subject 26 ;
‘Hospital Anxiety and Depression Scale’ (HADS): a 14-item questionnaire used for the screening of anxious and depressive feelings in people with chronic diseases 27 ;
‘Perceived Stress Scale’: classical 10-item instrument developed for the detection of distress arising from certain experiences 28 ;
‘Pearlin Mastery Scale’: a seven-item scale designed to measure the amount of internal or external control attributed to personal life choices 16 ;
‘World Health Organization Quality Of Life-Brief’ (WHOQOL-Brief): a short version of the original WHOQOL 29 composed of 26 items employed for the evaluation of the four aspects of QoL: ‘physical health’, ‘psychological health’, ‘social relationships’ and ‘environment’ 30 ;
‘Multidimensional Assessment of Interoceptive Awareness’ (MAIA): 32 items inventory used for the assessment of the eight components of enteroception: ‘noticing’, ‘not distracting’, ‘not worrying’, ‘attention regulation’, ‘emotional awareness’, ‘self-regulation’, ‘body listening’, ‘trusting’. 31
Medical reports
With regard to the matter of medical adherence, the final question of the online survey invited participants to attach (either directly on the platform or by sending it by e-mail to the researchers) the most recently available medical report. This was done to ascertain the degree of congruence between clinical evaluations and prescriptions and patients’ responses to the MARS-5I.
Data analysis
Data analyses were analysed using the software IBM SPSS Statistics (version 29, IBM Corporation©, Armonk, NY, USA) and its extension module PROCESS (version 4.3). 32 Statistical significance was set at α < 0.05. Missing data were not imputed and were excluded from data analyses.
The socio-demographic characteristics of the sample and clinical scales were analysed by identifying frequency, mean and standard deviation for each variable. For each scale or factor, reliability analysis was conducted by computing Cronbach’s alpha.
To fulfil the objectives of the present study, a factorial analysis of variance (ANOVA) between subjects was run to determine if mastery varied according to participants’ gender and clinical conditions. A linear multiple regression was conducted to verify if mastery was influenced by subjects’ current symptomatology, QoL, IAw and distress.
Regarding potential mediation and moderation models, a mediation process analysis and a moderation process analysis were performed.
Lastly, a comparison was made between the MARS-5I scores and the medical reports to ascertain the degree of congruence between the adherence levels reported and the clinical prescriptions.
Results
Characteristics of the study’s participants
A total of 418 records were collected via the online platform Qualtrics® (https://www.qualtrics.com). The responses were subjected to a process of data screening and assessment for instances of non-consensual participation. The final sample consisted of 261 participants. Figure 1 provides an accurate representation of the data-cleaning process.

Process of data cleaning.
Regarding participant demographics, among the 261 subjects enrolled in the study, 183 were women (70.1%), and 78 were men (29.9%). The average age was 38.43 years (SD = 14.48), and the average HBI was 4.95 (SD = 3.77; clinical remission). Table 1 illustrates the socio-demographic and clinical information of the sample.
Demographic and clinical characteristics of the sample.
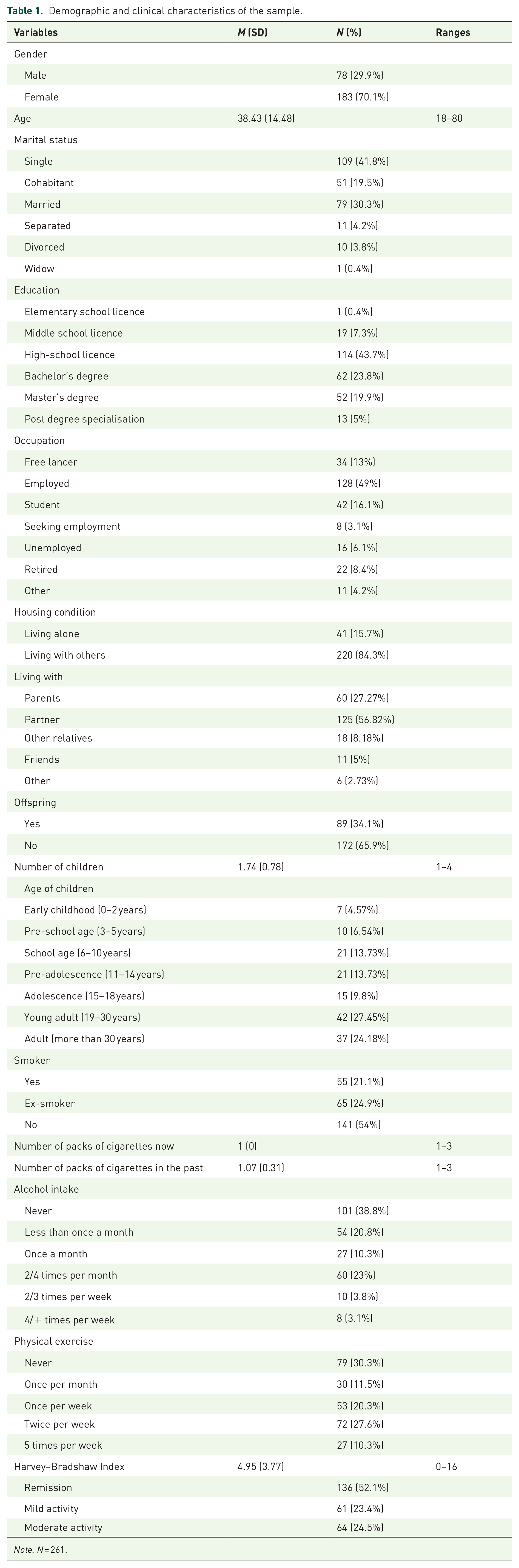
Note. N = 261.
Characteristics of the clinical scales
To ascertain the reliability characteristics of the various clinical scales employed in the study, the values of Cronbach’s alpha for each scale or dimension are reported in Table 2.
Values of Cronbach’s alpha.

A descriptive analysis of the data revealed that the mean level of mastery in the sample was 17.64 (SD = 3.63), indicating a distinct sense of personal mastery. The majority of the sample reported moderate distress (160 subjects, 61.5%); conversely, HADS indicated normal levels of depressive symptoms (M = 7.52, SD = 4.02), and mild levels of anxious manifestations (M = 9.07, SD = 3.95). The mean level of medical adherence was 20.11 (SD = 5.2), indicating a moderate degree of consistency in following clinicians’ prescriptions. Table 3 illustrates the descriptive statistics for all the clinical scales included in the research.
Descriptive statistics of clinical scales.

n = 261.
The relationship between mastery, gender and clinical conditions
A two-factorial ANOVA between subjects was conducted on a sample of 259 subjects to ascertain whether mastery, the dependent variable, varied according to gender (the independent variable, with two levels: male and female) and clinical conditions (the independent variable, with three levels: remission, mild activity and moderate activity). The results of the Levene test indicated no statistically significant difference (1.32, p = 0.26), allowing for the interpretation of the findings. ANOVA revealed no statistically significative differences in mastery in accordance with gender (F(1, 253) = 0.38, p = 0.54, η2 = 0.002); instead, there were statistically significative differences in mastery in relation to clinical conditions (F(2, 253) = 11.22, p < 0.001, η2 = 0.08). In this regard, post hoc analysis (Tukey’s HSD) highlighted statistically significant differences: subjects in remission presented higher levels of mastery compared to participants with mild activity (mean difference = 1.52, p = 0.01), and people with moderate activity (mean difference = 1.94, p < 0.001). Table 4 properly reports all descriptive statistics of mastery according to gender and clinical conditions.
Descriptive statistics of mastery according to independent variable.

Furthermore, an interaction effect between the two variables was observed (F(2, 253) = 7.22, p < 0.001, η2 = 0.05). The higher level of mastery was observed in male participants with CD in remission (M = 19.86, SD = 3.68); while the lower level was evident in men with mild activity (M = 15.19, SD = 2.74). Figure 2 shows the profile plot of the interaction effect between gender and clinical symptoms on mastery.

Profile plot of interaction effect between gender and clinical symptoms on mastery.
Influences on mastery
A multiple linear regression was calculated on a sample of 226 subjects to ascertain the impact of clinical conditions, distress, QoL (in its dimensions ‘physical health’, ‘psychological health’, ‘social relationships’ and ‘environment’) and IAw (in its factors ‘noticing’, ‘not distracting’, ‘not worrying’, ‘attention regulation’, ‘emotional awareness’, ‘self-regulation’, ‘body listening’, ‘trusting’) on mastery (dependent variable).
The independent variables considered for the analysis collectively explained the 55.8% of the variance in mastery. The F-test yielded a statistically significant result ((14, 211) = 21.32, p < 0.001), indicating that the model was statistically significant.
The regression coefficients were interpreted, and the results revealed that the factor ‘noticing’ was a significant predictor of mastery, with a beta coefficient of 0.13 (t-value of 2.37, p-value of 0.02). Furthermore, distress was identified as a statistically significant predictor of mastery, with a beta coefficient of −0.42 (t = −5.76, p < 0.001). Considering multicollinearity, VIF values ranged between 1 and 2 for all regression predictors, consequently, coefficients were considered acceptable.
Mediation models
To analyse the mediation process, Pearson’s correlations were performed between the variables that were considered in the model. These variables were mastery, distress, anxiety, depression and medical adherence. Table 5 presents the Pearson correlation coefficients and their associated significance levels. Subsequently, mediation process analyses were conducted. The mediator variable was mastery, while the independent variables were anxiety (in the first model), depression (in the second model), and distress (in the last model). The dependent variable was medical adherence. No statistically significant results were obtained from any of the models. The respective p-values for the first, second and third models were 0.13, 0.18 and 0.06.
Pearson’s linear correlations for mediation and moderation analysis.

n = 257, significance (sign.) was two-tailed, *indicated a statistically significative correlation for α = 0.05, ***indicated a statistically significative correlation for α = 0.001.
Congruence of medical adherence
Regarding the congruence between MARS-5I scores and medical reports attesting to clinicians’ prescriptions, 44 participants attached the relevant documentation.
An analysis of the type of medical report provided alongside the survey responses revealed that four subjects (9.1%) had submitted blood tests, 34 (the majority) had undergone gastroenterological assessment, 4 (9.1%) had presented the results of abdominal magnetic resonance imaging and 2 participants (4.5%) had submitted the results of intestinal biopsies. In the subsample, the mean score on the MARS-5I was 20.89 (SD = 4.87), indicating a moderate level of adherence to medical recommendations.
Analysing congruence between the two aspects, in three cases (6.8%) it was impossible to determine the consistency. In most cases (30 subjects, 68.2%), there was correspondence between the provided medical report and the MARS-5I score, 8 persons (18.2%) presented a partial congruence and only for three participants (6.8%) resulted in a lack of consistency.
Discussion
The present study aimed to examine the construct of mastery and the influence of other psychological variables within a cohort of patients diagnosed with CD. The study was conducted in a cross-sectional design, in accordance with the recommendations outlined in the scientific literature. The objective was to examine the role of mastery in relation to other psychological variables, as well as the participants’ demographic and clinical characteristics, and its potential as a mediator in the relationship between medical adherence and psychological state. The clinical manifestations of CD have been demonstrated to significantly diminish patients’ sense of control and their overall QoL.6–8,13,20,33 Indeed, despite the majority of the sample being in remission (136 subjects, 52.1%), factorial ANOVA revealed a statistically significant effect of the illness status on mastery, as well as an interaction effect of clinical symptomatology and gender on the construct. By contrast, with regard to gender, the findings were inconsistent with those of previous studies which have indicated that women experience greater impairment in QoL, mental health and mastery. 20 The overall mean level of mastery for the entire sample was 17.64 (SD = 3.63), with male patients experiencing mild disease activity exhibiting the lowest scores (M = 15.19, SD = 2.74). While this study offers preliminary insights into mastery in individuals with CD using online self-report questionnaires – prone to potential subjective bias – these findings should be interpreted with caution. Nevertheless, the results support the notion that mastery may be diminished in chronic conditions, even during symptomatic remission or in cases of mild clinical manifestations. 33
Furthermore, multiple linear regression analysis revealed a significant relationship between mastery, clinical conditions, QoL, stress and interoception. Specifically, distress and ‘noticing’ (a dimension of interoceptive awareness) emerged as significant predictors of mastery: distress was negatively associated with mastery (higher stress levels were linked to reduced mastery), while ‘noticing’ was positively associated (greater interoceptive awareness corresponded to higher mastery). This evidence is interesting for different reasons. Firstly, many participants of the study reported experiencing moderate levels of distress in their lives (160 subjects, 61.5%), and the literature identified stressors as one of the determinants of personal mastery.16,18 Furthermore, chronic pain affects interoceptive awareness exacerbating perceived stress.10–15 Lastly, enhanced enteroception is related to acceptance of bodily sensations, and a general sense of self-control11–15,34; the assumption that may explain the positive association between mastery and IAw traits.
Stressors are considered one of the most impactful factors of QoL for individuals with CD. 33 Examining QoL dimensions, the sample obtained discrete scores for physical health (M = 12.79, SD = 3.06), psychological health (M = 12.09, SD = 2.99), environment (M = 12.73, SD = 2.62) and social relationships (M = 12.53, 3.78). These may be regarded as considerable results since social support is a determinant aspect for patients, aiding in the management of CD.7,19
In the present study, mental health was also operationalised both in terms of anxious and depressive manifestations. In general, participants reported normal scores of depressive symptoms (M = 7.52, SD = 4.02), and mild levels of anxious symptomatology (M = 9.07, SD = 3.95), with 86 subjects (33%) that referred to moderate levels of anxiety. The results were consistent with the higher prevalence of mental health comorbidities in people with CD.7,8
Focusing on the possible role of mastery as a mediator in the relationship between medical adherence and psychological state (in terms of stress, anxious and depressive feelings), it is relevant to state the non-statistically significance of each mediation model considered, non-significance that reoccurred even for moderation process analyses. The evidence may plausibly be attributed to the moderate levels of consistency to clinical prescription in the sample (M = 20.11, SD = 5.2); coherently with literature findings reporting great taxes of non-adherence in individuals with CD. 6 Moreover, the average age was low (M = 38.43, SD = 14.48), and the sample was mostly in symptomatologic remission (HBI score M = 4.95, SD = 3.77). Indeed, clinical studies report how young patients tend to be less adherent to medical prescriptions, perhaps for a minor experience of clinical complications and hospitalisations.6,35 Similar levels of medical adherence were reported in the subsample of subjects that provided medical reports (M = 20.89, SD = 4.87), despite in most cases (30 subjects, 68.2%) there was correspondence between the clinical examination and the MARS-5I score; evidence consistent with the above mentioned scientific literature.6,35 Regrettably, the present research did not consider the impact of the specific categories of medical treatment on adherence to therapy and mastery in patients with CD. This relevant issue should be deepened, given the several adverse effects aroused by medications, especially biological therapies. 36
However, collectively, the sample was composed of 261 adults with CD, higher than the one required by the power analysis, and the association ‘AMICI Italia’ helped in the recruitment process: thus, allowing to enrol in the study patients from all regions of Italy and to limit self-selection bias.
Limitations
Our study had several limitations, mostly due to the type of sample. The employment of a convenience sample restricted the possibilities of data extension. Participants were mainly female subjects in remission; consequently, the study did not have a representative sample. Given that the research involved an online questionnaire, self-selection bias may have occurred. It is plausible that this may have contributed to the determination of the result concerning participants’ gender and clinical condition in relation to mastery, which was in contrast with the existing literature.
Additionally, as previously mentioned, this study did not explore the impact of different categories of medical treatments for CD (e.g. steroids, biologics, antibiotics) on patients’ sense of mastery and adherence to treatment. It is important to acknowledge that this study represents a pioneering attempt to examine the construct of mastery in patients with CD. It provides a preliminary foundation that can be expanded upon in future investigations employing diverse methodologies. Furthermore, the research was designed to circumvent self-selection bias by disseminating the study to individuals with CD across the entire Italian territory with the assistance of the AMICI Italia association.
Further research and clinical implications
Future research should focus on further examinations of mastery in patients with active symptomatology of CD, employing larger and more heterogeneous samples and different methods.
Mastery indeed needs to be analysed in-depth, along with its relationship with medical adherence. This is particularly crucial given the risk of hospitalisations and complications, and the consequences on the healthcare system, of untreated CD5,6; considering, mastery’s association with improvements in both mental and physical health, and its nature of psychological resources that can mitigate the impact of symptoms worsening.13,17,18 Another aspect that literature should emphasise in the future is the influence of the various categories of medications on mastery and adherence to therapy, given the widespread collateral effect. 36
Therefore, further studies are needed to identify the most effective approaches to enhance mastery and consistency with clinical prescriptions in individuals with CD. By identifying patients with low levels of mastery, healthcare providers can intervene early with appropriate support and interventions to mitigate the negative impact of stress and improve disease management outcomes.
Conclusion
The results of this study support the hypothesis that patients with CD experience an effective impairment of mastery, in alignment with the assumptions made in the existing literature on the subject. Besides, male patients experiencing mild disease activity exhibited the lowest mastery score, in contrast to findings from previous studies, referring women who experience greater impairment in QoL, mental health and mastery. However, the results support the idea that mastery may be reduced in chronic conditions, even during symptomatic remission or in cases of mild clinical manifestations. Furthermore, the higher prevalence of distress, anxiety and depressive symptoms was substantiated, in alignment with the existing literature on patients’ QoL and enteroception. In addition, the relationship between these psychological manifestations and mastery was corroborated, in accordance with literature evidence concerning the psychological state of individuals with CD, and the influence of stressors on mastery. Notably, this study highlighted a positive association between mastery and enteroception in patients with CD, a construct deeply implicated in chronic pain conditions.
Conversely, regarding the potential mediator role of mastery, the study’s hypothesis was not supported, as the mediation process analysis yielded insignificant results. While these findings may be attributed to the participants’ demographic and clinical characteristics (predominantly in remission and young) and are consistent with existing literature, future research should delve deeper into this topic.
These findings must be regarded as preliminary and further extended to a larger sample and investigation with the employment of other methods is required. Nevertheless, the present study aimed to provide evidence that an invalidated sense of mastery is present in individuals diagnosed with CD. The collaboration with the AMICI Italia association enabled the recruitment of participants with CD from all regions of Italy, thereby reducing the potential for self-selection bias in the sample.
Supplemental Material
sj-doc-1-tag-10.1177_17562848251314796 – Supplemental material for The role of mastery in Crohn’s disease: a cross-sectional study
Supplemental material, sj-doc-1-tag-10.1177_17562848251314796 for The role of mastery in Crohn’s disease: a cross-sectional study by Marina Francesca Gattoni, Enrica Previtali, Salvatore Leone, Alessia Amore and Eleonora Volpato in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors thank the Italian National Association for Inflammatory Bowel Diseases ‘AMICI Italia’ for the support provided, and all the patients who contributed to participate in the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.