
Abstract
Background:
Eosinophilic esophagitis (EoE) is recognized as a chronic type 2 inflammatory disease characterized by the eosinophilic infiltration of the esophageal tissue, posing a significant disease burden and highlighting the necessity for novel management strategies to address unmet clinical needs.
Objectives:
To critically evaluate the existing literature on the epidemiology and management of EoE, identify evidence gaps, and assess the efficacy of current and emerging treatment modalities.
Design:
An extensive literature review was conducted, focusing on the epidemiological trends, diagnostic challenges, and therapeutic interventions for EoE. This was complemented by a survey among physicians and consultations with a scientific expert panel, including a patient’s association (ESEO Italia), to enrich the study findings.
Data sources and methods:
The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, scrutinizing epidemiological studies and management research to compile comprehensive insights into the disease’s landscape. The physician survey and expert panel discussions aimed to bridge identified evidence gaps.
Results:
The review included 59 epidemiological and 51 management studies, uncovering variable incidence and prevalence rates of EoE globally, with an estimated diagnosed prevalence of 41 per 100,000 in Italy. Diagnostic challenges were identified, including nonspecific symptoms and the lack of definitive biomarkers, which complicate the use of endoscopy. Treatment options such as elimination diets, proton-pump inhibitors, and swallowed corticosteroids were found to have varying success rates, while Dupilumab, an emerging therapy targeting interleukin (IL)-4 and IL-13, shows promise.
Conclusion:
Despite advancements in understanding and managing EoE, significant unmet clinical needs remain, particularly in biomarker identification, therapy personalization, and cost-effectiveness evaluation. A comprehensive, multidimensional approach to patient management is required, emphasizing the importance of early symptom recognition, accurate diagnosis, and tailored treatment strategies. Dupilumab offers potential as a novel treatment, underscoring the need for future research to explore the economic and social dimensions of EoE care pathways.
Plain language summary
Eosinophilic esophagitis (EoE) is a chronic inflammatory condition affecting the esophagus. We reviewed studies on how common EoE is and how it’s managed. In Italy, about 41 out of 100,000 people may have it. Diagnosis can be tricky due to vague symptoms, and current treatments vary in effectiveness. We found a need for better ways to diagnose and treat EoE, including exploring new therapies. A promising development is a biologic called Dupilumab. Future research should also consider the costs and social aspects of caring for people with EoE.
Introduction
Eosinophilic esophagitis (EoE) is a chronic type 2 inflammatory disease of the esophagus characterized by eosinophilic infiltration into its tissue.1–4 Studies on EoE endotypes suggest that the condition might progress over time. 39 Common symptoms in adult patients include dysphagia, food impaction, heartburn, and chest pain.3,5–7 The pathogenesis is multifactorial and arises from a complex interaction among genetic, intrinsic, environmental factors, as well as antigenic stimuli.4,5,7–9 Diagnosis relies on a comprehensive evaluation of clinical presentation, endoscopic findings, and biopsy results. 10 Managing EoE requires a multidisciplinary approach involving gastroenterologists, allergists, and pediatricians. Treatment options encompass elimination diets, proton-pump inhibitors (PPIs), swallowed topical corticosteroids (TCSs), and, if clinically relevant strictures persist despite initial therapies, esophageal dilation.11–16 While broad consensus exists on these initial therapies, some patients do not respond adequately to current treatments. Therefore, there is a need for effective therapies targeting the underlying inflammatory processes to induce and sustain disease remission. 13 One promising novel therapy for EoE is Dupilumab, a monoclonal antibody that modulates the activity of key cytokines involved in EoE development [interleukins 4 (IL-4) and 13 (IL-13)].17,18 Since 2017, there have been no updates to the management strategies for EoE in Italy. However, it is noteworthy that the latest British Society of Gastroenterology (BSG) Guidelines from 2022 have integrated the most recent advancements, including the adoption of Dupilumab.15,19,20
Hence, this review article aims to comprehensively discuss the disease burden, pathophysiology, diagnostic strategies, and presently available treatment options for EoE based on current literature. 8 Furthermore, our aim is to propose a novel approach for managing EoE.
Methods
A literature review on the epidemiology, current management practices, including diagnosis and treatment pathways for patients with EoE, was conducted (by authors FR and AC) with the objective of identifying gaps in the existing evidence within the field. Subsequently, a survey among physicians was carried out to partially address the identified gaps in the literature. All results were discussed and validated by a scientific expert panel of eight clinicians and the leader of Italian Association of Families Against Eosinophilic Esophagitis (ESEO Italia). This collaborative effort aimed to reach a consensus on the management of EoE.
The steps involved in this process were as follows (Figure 1).
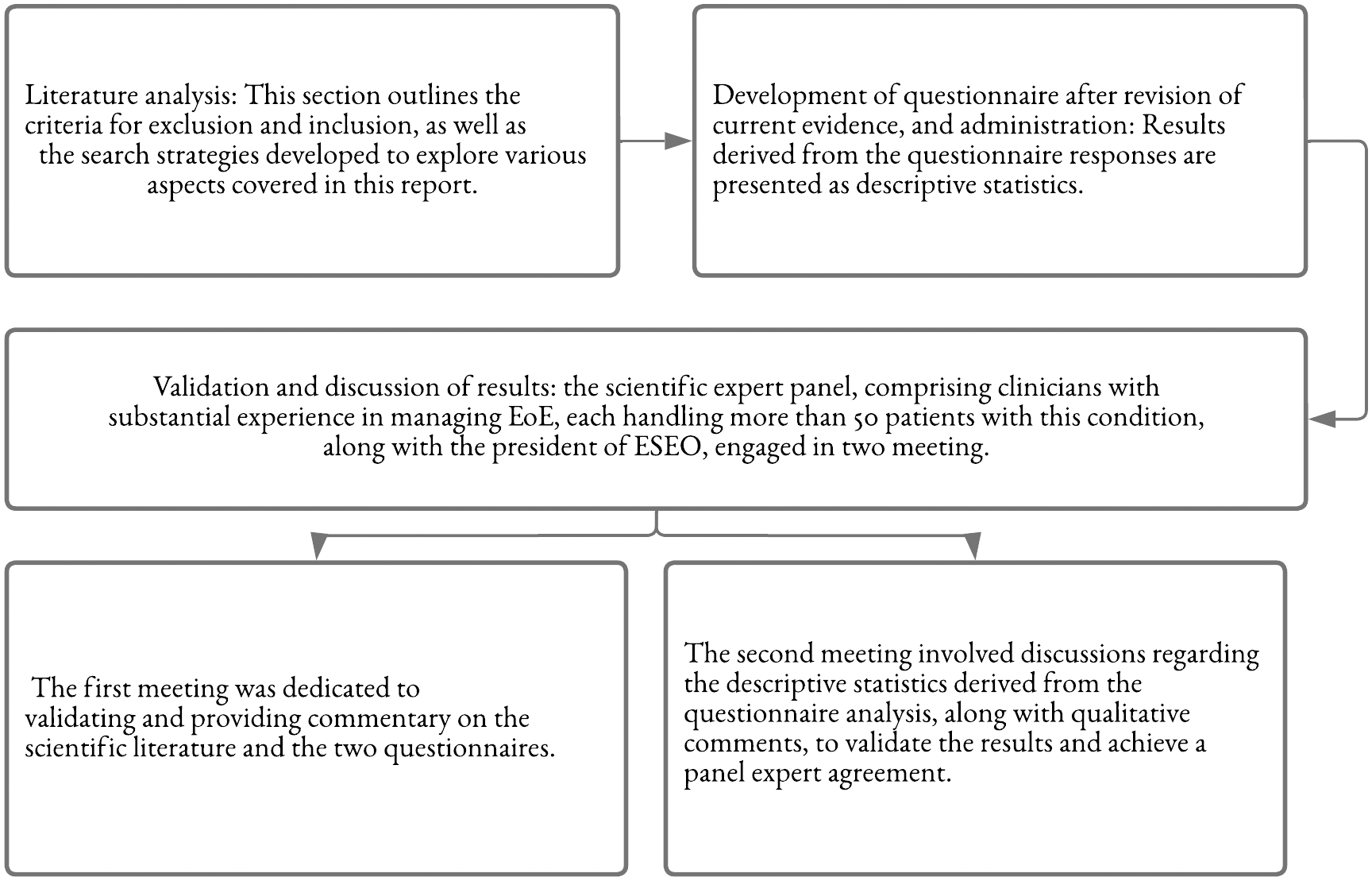
The study phases.
Systematic review
A PICO model specifying target population (P), intervention (I), comparators (C), and outcomes (O) was stated. The research strategy encompassed two distinct research queries: one focused on investigating the epidemiology of EoE and the other aimed to examine current management practices. Adhering to PRISMA guidelines, studies were sought from the PubMed and EBSCO-MEDLINE databases in May 2022. For the search related to current management and the economic burden of EoE, a time limit of 20 years was applied to the epidemiological search to discern prevalence and incidence trends. Initial screening of evidence was conducted based on keywords within records, delving into identified systematic literature reviews and meta-analysis to extract further Evidence was initially screened based on keywords reported in records and within title or abstract. In addition, a snowball sampling method was applied to the identified systematic literature reviews and meta-analyses to detect more information on topics investigated. Records were eligible unless they met one or more of following criteria: irrelevant to studied condition, nonrelevant study type, or insufficient information. All articles were classified in Microsoft Excel worksheet after being exported from EndNote software. In Figures 2 and 3, we are reporting the results of our review through the PRISMA flowcharts. Supplemental Table S1 shows the query strings and the included studies related to the literature review.

PRISMA model. Flowchart of the literature review process relating to the EoE epidemiology.

PRISMA model. Flowchart of the literature review process relating to the EoE current management.
Questionnaire
The questionnaire comprised 3 sections and a total of 34 questions (Supplemental Table S2). Section 1 comprised five questions and investigated epidemiology of EoE in adult and adolescent patients. Section 2 comprised nine questions and explored challenges in diagnosis. Section 3 comprised 20 questions and examined the current therapies for managing EoE. The survey used three question types: multiple-choice, open-ended, and Likert-scaled. The Likert-scaled questions were rated from 1 (not important) to 7 (extremely important). A score between 5 and 7 was considered when defining the agreement. Questionnaire was administered to the scientific expert panel, with the subsequent possibility for panel members to share the survey with additional key opinion leaders and clinicians experienced in EoE.
Results
The epidemiological research identified 648 studies, of which 522 were excluded after title/abstract assessment. Subsequent full-text review excluded 12 studies reporting epidemiological data on other conditions, 7 on EoE and other conditions, and 39 reporting nonspecific epidemiological data. Additionally, nine studies were excluded due to the unavailability of full text. Finally, 59 studies were included (Figure 2).
The current management research identified 619 studies, of which 493 were excluded after title/abstract assessment. Subsequent screening excluded 18 studies reporting a condition other than EoE, 21 presenting insufficient information, and 36 reporting a nonrelevant study type. Finally, 51 studies were included (Figure 3).
After reviewing and critically analyzing the current evidence, a survey has been developed and administered to 80 physicians from different specialty. A total of 52 respondents (65%) completed the questionnaire. The respondents comprised 37 gastroenterologists, 7 allergists, 4 internists, and 3 pediatricians; only 1 responding physician did not indicate his clinical specialization.
Summary findings
Epidemiology
The incidence and prevalence of EoE varied among studies, reflecting differences in population features such as geographical location, ethnicity, gender, and age. 8 These variations were corroborated by Arias et al., 21 who noted a higher prevalence and incidence rate in North America (30.7 and 5.4 per 100,000 inhabitants/year, respectively) than in Europe (16.1 and 1.7 per 100,000 inhabitants/year, respectively). The prevalence rate ratio by gender was also highlighted, with a rate of 53.8 per 100,000 inhabitants for males compared to 20.1 per 100,000 for females. Additionally, this study explored prevalence in different age groups, reporting rates of 28.9 per 100,000 for adults and 26.9 per 100,000 for pediatric patients. 21
More recently, Navarro et al. conducted a systematic review to assess the current incidence and prevalence of EoE due to its escalating occurrence. They reviewed 29 population-based studies, encompassing 2386 documents, to update outdated estimates of EoE incidence and prevalence. The pooled prevalence of EoE was found to be 34.4 cases per 100,000 inhabitants, with higher rates in adults (42.2) than in children (34). Incidence rates were 6.6/100,000 person-years in children and 7.7/100,000 in adults. The analysis revealed no significant differences between North American and European studies or between different data sources. Despite variations in the definitions used for EoE, a consistent rise in both incidence and prevalence rates over time was observed. These findings indicate a substantial increase in EoE rates compared to previous estimates, especially in developed countries, emphasizing the need for updated awareness and diagnostic strategies for this condition. 40
Other studies have reported a higher prevalence of EoE among Caucasians than in other ethnic groups.21–24 Considering the heterogeneity among results in various epidemiological studies and systematic reviews and the limited data regarding the Italian national context, clinicians were interviewed to gather epidemiological data in their respective countries. Summarizing questionnaire results based on clinicians’ feedback and the variability rates in different countries (e.g. 7/100,000 in Serbia and 500/100,000 in Ireland, averaging 38.7/100,000), along with the similarity between Italy and Spain (67/100,000), the panel agreed on a diagnosed prevalence of 41/100,000 inhabitants (standard deviation: ±23.89).
Diagnostic challenges and red flags
Diagnosing EoE can pose challenges. In adult patients, symptoms vary in severity, ranging from difficulty in swallowing, food impaction, heartburn, chest pain, and nausea. These symptoms are nonspecific to EoE and can resemble other gastrointestinal disorders such as gastroesophageal reflux disease and esophageal motility disorders. In pediatric patients, clinical presentations span from mild, nonspecific symptoms like abdominal pain, vomiting, and dyspepsia to more severe manifestations like failure to thrive, dysphagia, and even food impaction, depending on the age at diagnosis. Additionally, specific noninvasive biomarkers aiding in the diagnosis of EoE are lacking. Ishihara et al. conducted a study to evaluate eosinophil-related proteins as potential serum biomarkers for diagnosing and monitoring eosinophilic gastrointestinal diseases. They examined serum concentrations of 49 cytokines, chemokines, and other proteins in 29 patients with eosinophilic gastrointestinal diseases and 80 controls. While some proteins did not show significant elevation in serum levels, others like BCA-1/CXCL13 and HCC-1/CCL14α were elevated, and GCP-2/CXCL6 was suppressed in patients with EoE and gastroenteritis. Furthermore, CTACK/CCL27, SDF-1/CXCL12, MIP-3β/CCL19, and SCCA2 were found to be elevated specifically in EoE. Despite these findings, the study concluded that none of the 49 investigated serum proteins exhibited sufficient sensitivity to be reliable biomarkers for diagnosing or monitoring eosinophilic gastrointestinal diseases with the available assay systems. This conclusion was supported by a recent review on noninvasive biomarkers’ role in EoE. 38
Another diagnostic challenge in identifying EoE involves the inappropriate use of endoscopy. Although endoscopy might not be sensitive enough to detect EoE, it remains the most used diagnostic tool.10,26,27 For instance, Oude Nijhuis et al. assessed the diagnostic efficacy of routine esophageal biopsies in individuals experiencing refractory reflux symptoms. Among 301 enrolled patients, only 4.7% met clinicopathological diagnostic criteria for EoE. Notably, factors like dysphagia, food bolus impaction, an atopic background, and typical endoscopic features exhibited the strongest associations and diagnostic accuracy for EoE. However, in patients lacking symptoms of dysphagia or relevant endoscopic features, the diagnostic yield was minimal, at 0% and 1.9%, respectively. The study suggests that routine esophageal biopsy sampling in individuals with refractory reflux symptoms has low diagnostic yield and recommends selectively obtaining esophageal biopsies, focusing on patients with refractory reflux symptoms accompanied by dysphagia for a more targeted and clinically meaningful diagnostic approach. Interpretation of biopsy results may also pose challenges, as patient-reported symptoms may not consistently align with histological activity. Therefore, the standard diagnostic threshold is defined as ⩾15 eosinophils in at least one high-power field. Additional histological features integrated into the EoE histologic scoring system support diagnosis and aid in evaluating inflammatory activity during follow-up. Consequently, reaching the correct diagnosis can often be difficult, leading to diagnostic delays. Factors contributing to these delays include delayed referral to gastroenterologists, postponed esophagogastroduodenoscopy, and inadequate biopsy collection or histopathologic evaluation. 2
A recent study by Lenti et al. 28 revealed a median diagnostic delay of 3 years for EoE. One approach to hasten EoE diagnosis involves recognizing the concurrent presence of various warning signs, such as difficulty in swallowing, food impaction, reflux symptoms, noncardiac chest pain, a history of atopic/type 2 inflammatory diseases and food allergies, and, in young patients, failure to thrive. 3
A survey was conducted to explore physician perceptions of diagnostic challenges within the Italian context. Results indicated that physicians estimate an average of 41 (standard deviation: ±23.89) out of every 100 patients are correctly diagnosed with EoE (diagnosed prevalence). Additionally, clinicians were asked to identify, based on their experience, the most critical factors for a timely and accurate diagnosis. Red flags were categorized into three main groups: patient’s clinical history, exclusion of other possible confounding conditions for diagnosis, and performing endoscopy to confirm the diagnosis. The analysis of results (Figure 4) highlighted bolus impaction (mean score = 6.4) as the most significant factor for a correct and timely diagnosis. This finding was supported by 88.5% of respondents who regarded bolus impaction as crucial (score of 5–7). The survey also indicated that other critical factors for a correct diagnosis included accurate biopsy sampling (mean score = 6.1), presence of dysphagia (mean score = 5.7), and characteristic lesions observed during endoscopy (mean score = 5.3).

Red flag results from the physician survey.
Treatment
pathway and available therapies.
The current treatment pathway for EoE (Figure 5) aims to alleviate tissue inflammation and symptoms. First-line treatment typically involves dietary modifications and medications.7,8,12,14,15 Dietary changes, specifically eliminating certain trigger foods (e.g. dairy, wheat, soy, and eggs), may help in alleviating symptoms and reducing inflammation.9,12 Medications used to address EoE include PPIs, which exhibit anti-inflammatory effects and promote enhanced barrier function, as well as topical steroids (TCS).12,29 Additionally, esophageal dilation, performed using Savary dilators/bougie or hydrostatic balloons, has proven to be a relative safe and effective treatment for both adult and pediatric EoE patients with fibrostenotic features, particularly when combined with other therapeutic strategies targeting eosinophilic inflammation. However, the treatment pattern for each patient is individualized based on severity, age, overall health, and food allergies or intolerances. 8 Consequently, challenges regarding adherence, long-term efficacy, and adverse events persist.

EoE treatment plan (2017 EoE guidance from the UEG, EAACI, ESPGHAN, and EUREOS).
The induction phase seeks to diminish inflammation and ameliorate symptoms, with patients often experiencing improvement after several weeks or months of treatment. Common therapies during the induction phase include PPIs, swallowed corticosteroids, or elimination diets, typically leading to symptom improvement in 60–80% of patients.30–32 Subsequently, patients transition to the maintenance phase to avert symptom recurrence and sustain disease remission. Swallowed corticosteroids and elimination diets effectively sustain remission in approximately 50–70% of patients. 30 Even PPIs have demonstrated some success in maintaining long-term remission (60%).29,31,32 Various factors contribute to the variability in treatment response among patients, as outlined in existing literature. These factors may encompass the patient’s overall health status, severity and nature of the treated condition, presence of concurrent medical conditions, genetic factors, and adherence to prescribed treatment regimens.
Concerning PPIs, 43.62% of physicians reported unsatisfactory patient responses to monotherapy, with approximately 5% discontinuing treatment due to side effects, with an average treatment duration of 19 months.
Regarding TCS, physicians noted that 15.84% of treatments were discontinued due to lack of drug efficacy, approximately 11% of patients were unsuitable candidates, with an average treatment duration of 24.08 months.
It is important to emphasize that the data concerning PPIs and TCS are solely based on the perceptions of participating clinicians in the survey. Moreover, regarding the discontinuation rate, it remains unclear whether clinicians considered possible nonadherence to prescribed treatments.
Among responding clinicians, 23.1% agree that first-line treatment with PPIs is equivalent in efficacy to TCS, while the remainder disagree. Additionally, the expert panel agreed that due to adverse events (e.g. candidiasis up to 18%), TCS are not typically prescribed continuously but rather in intermittent courses, which might not be suitable for the continuous treatment of a chronic disease. 33
Apart from current therapies, novel biological treatments are in development, 16 such as Dupilumab, a monoclonal antibody blocking IL-4 and IL-13 signaling, key and central drivers in EoE and other type 2 inflammation diseases, has shown promising results in reducing statistically symptoms, histological and endoscopical features of EoE.15–17 Its approval as the first and sole biological therapy by the US Food and Drug Administration (FDA) and the European Medicine Agency has marked its efficacy. 16 However, various other biologic drugs are currently undergoing development. 16
The panel of experts suggests (Figure 4) that Dupilumab could be a significant option for adults and adolescents (transitional age) inadequately controlled by, intolerant to, or ineligible for at least one conventional therapy. Additionally, in EoE patients with one or more type-2 inflammatory diseases, considering treatment in the first line with Dupilumab is recommended as well as in the adolescents (transitional age) patients who are at risk of TCS use.
Of note, in the context of EoE, the terms ‘inadequately controlled’, ‘intolerant to’, and ‘not candidates for’ conventional therapy require clear operational definitions to guide clinical decision-making.
‘Inadequately controlled’ refers to patients whose symptoms and disease activity persist or worsen despite an appropriate course of conventional therapy (i.e. PPIs, TCS, and dietary interventions). It implies that the chosen treatment regimen, pharmacological or dietary, has not effectively managed or alleviated EoE symptoms and eosinophilic inflammation.
Patients categorized as ‘intolerant to’ conventional therapy experience adverse reactions or side effects significantly impacting their quality of life (QoL) or hindering adherence to prescribed treatment. These reactions might manifest as allergic responses, gastrointestinal discomfort, or other adverse effects compromising continued adherence to the recommended therapy.
Regarding ‘not candidates for’ conventional therapy, this category includes individuals for whom standard treatment options are deemed unsuitable or present unacceptable risks. It may encompass patients with contraindications to specific medications or those for whom dietary restrictions are impractical or unsustainable (Figure 6).

2023 Italian treatment pathway for adult and adolescent (transitional-age) EoE (type 2 inflammation disease). Panel expert guidance.
The unmet clinical needs
Despite recent advancements in diagnosing and treating EoE, there remain several unmet clinical needs requiring further research and development. The literature review revealed a lack of specific biomarkers for diagnosing EoE, 25 specific therapies tailored to the unique features of EoE, efficacy and safety data concerning available treatments, QoL data for EoE patients, and cost-effectiveness analyses comparing new biologic drugs with traditional therapies for managing EoE. 16
To gauge the perception of unmet clinical needs in Italy, the questionnaire assessed the impact of current therapies on patients’ QoL (the subjective impression experts have about the level of QoL in EoE patients) and clinical outcomes, as well as their effectiveness. The assessment considered the importance of clinical, histological, and endoscopic remission dimensions in evaluating treatment effectiveness.
According to the survey results, histological remission received the highest mean score of 6.4, with 94% of physicians regarding it as the ‘most important’ factor. Clinical remission followed closely with a mean score of 6.3, endorsed by 92% of respondents. However, endoscopic remission was perceived as the less important factor among those investigated, earning an average score of 5.4 (Figure 7), with agreement from 76% of participants.

Importance of various remission factors for evaluation of treatment effectiveness.
Discussion
While the first case of EoE was reported in 1970, the disease, as recognized today, was described in only three cases in the early 1990s. Although EoE has been considered a rare condition, it remains a significant cause of morbidity in the upper gastrointestinal tract, resulting in increased healthcare costs. 6 The exact causes of EoE are not completely understood but are believed to be linked to genetic, environmental, and immune factors. Despite being relatively new, the incidence of EoE is on the rise globally, with reports of 1–34 new cases per 100,000 people per year. 34
Diagnosing EoE can be challenging due to its nonspecific symptoms and the absence of specific biomarkers. Diagnostic tools currently available are not sensitive enough to detect it. A major issue for EoE is diagnostic delay, with an average time from the first symptom to the final diagnosis being 10 years.16,35 Factors such as patient-dependent issues and misdiagnosis contribute to this delay, leading to increased EoE severity. In cases where patients report minimal symptoms, clinicians should explore dietary and adaptive behavioral or modifications, such as eating slowly, thorough chewing before swallowing, drinking fluids to aid swallowing, and avoiding solid foods. These adjustments help patients adapt to the reduced esophageal distensibility. 36 However, enhancing our understanding of EoE’s natural progression and refining clinical management will reduce diagnostic delays and optimize patient care pathways. Incorporating red flags into patient evaluations can enhance EoE diagnosis and management. 37 Essential red flags involve taking the patient’s initial history and ruling out other potential confounding conditions. Raising awareness among primary care physicians, often the first point of contact for patients with EoE symptoms, is the primary step. Subsequently, an optimal patient journey necessitates a multidisciplinary approach involving gastroenterologists, allergists, pathologists, and dietitians. Upon diagnosis, patients should be referred to specialists capable of performing endoscopies and biopsies to confirm the diagnosis and evaluate disease severity. Therefore, assessing EoE severity requires a multidisciplinary approach, considering clinical symptoms, endoscopic findings, histological evaluations, patient-reported outcomes, and emerging biomarkers. Integrating these factors offers a comprehensive understanding of individual patients’ EoE severity, aiding treatment decisions and monitoring disease progression.
Tailoring treatment to each patient’s specific needs based on factors like age, symptom severity, and comorbidities is crucial. This consideration should encompass current therapeutic approaches and novel biologic therapies displaying promising efficacy and patient safety. Regular follow-ups and monitoring are equally essential to assess treatment effectiveness, identify potential complications, or make necessary therapy adjustments. This study had two main limitations. First, there is a significant lack of evidence in the literature concerning the epidemiology and management of EoE in Italy. To address this gap, a survey was administered, although expert opinion cannot fully compensate for the absence of context-specific epidemiological studies. Second, despite being administered to EoE disorder experts, the survey was influenced by the inherent subjectivity of their responses, representing a second limitation of this study. Moreover, in addressing the limitations of our study, it is important to note that the survey was administered to a highly heterogeneous group of physicians. This diversity, while enriching the breadth of perspectives collected, also introduces a limitation as the survey did not investigate in depth the specific training physicians received on EoE, their experience in managing EoE patients, and the duration of their engagement in this field. Acknowledging this, our findings may not fully reflect the nuanced understanding and approaches that vary with different levels of expertise and experience in EoE management. Additionally, the number of respondents in the current study is relatively low, which may further limit the generalizability of our findings. Future studies could benefit from a more detailed exploration of these aspects and consider including a larger pool of respondents to better understand their impact on the management of EoE and to enhance the robustness and applicability of the results.
Conclusion
EoE is a chronic progressive type 2 inflammatory disease with a complex pathophysiology that can cause significant morbidity if not diagnosed and managed appropriately and promptly. The patient journey with EoE can pose challenges, and identifying red flags can assist in identifying patients who require further investigation and management.
The current standard of care for EoE involves dietary therapy, PPIs, and TCSs. However, many patients still experience symptoms, face adherence challenges, and encounter adverse events. Consequently, there remains high unmet medical need, necessitating the development of new additional therapies.
The recently approved biologic, Anti IL-4 and IL-13, a monoclonal antibody that blocks the signaling of IL-4 and IL-13, pivotal cytokines involved in EoE development and type 2 inflammation, has demonstrated positive short- and long-term results in clinical trials, offering a new treatment option for EoE patients.
In conclusion, establishing a new patient care pathway, beginning with the timely and accurate diagnosis of EoE, followed by the tailored definition of therapy based on individual patient needs, forms the foundation for future analysis. Further studies will be essential to assess the economic and social perspectives of this pathway for patients with EoE.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241249570 – Supplemental material for Eosinophilic esophagitis in adults and adolescents: epidemiology, diagnostic challenges, and management strategies for a type 2 inflammatory disease
Supplemental material, sj-docx-1-tag-10.1177_17562848241249570 for Eosinophilic esophagitis in adults and adolescents: epidemiology, diagnostic challenges, and management strategies for a type 2 inflammatory disease by Edoardo Vincenzo Savarino, Giovanni Barbara, Maria Beatrice Bilò, Nicola De Bortoli, Antonio Di Sabatino, Salvatore Oliva, Roberto Penagini, Francesca Racca, Annalisa Tortora, Filippo Rumi and Americo Cicchetti in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to thank ESEO Italia – ‘Associazione di famiglie contro l’esofagite eosinofila’, and the President: Dr. Roberta Giodice, for their contribution with no corresponding fees.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.