
Abstract
Eosinophilic esophagitis (EoE) is a chronic inflammatory disorder of the esophagus characterized by symptoms of esophageal dysfunction and eosinophil-predominant inflammation. The incidence of EoE has increased substantially over the past two decades in Europe and North America. The natural course of EoE appears to be progressive with a high risk of stricture formation. The current European guideline recommend swallowed topical corticosteroids, proton-pump inhibitors or dietary intervention for initial and long-term treatment of EoE. Swallowed topical corticosteroids can be considered to be the best studied drug class in EoE, with more than 1000 patients enrolled in randomized clinical trials worldwide. In most of them, fluticasone or budesonide formulations have been used that were originally designed for asthma therapy, thus presumably suboptimal for EoE treatment. The new orodispersible budesonide tablet with effervescent properties is the first approved esophageal-targeted formulation specifically developed for the treatment of EoE, which has become available in many European countries. This article gives an overview of the evolution of topical corticosteroids in EoE and provides an update on recent data from large-scale multicenter trials exploring the efficacy and safety of the orodispersible budesonide tablet with effervescent properties in adult EoE patients.
Background
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated esophageal disease, characterized clinically by symptoms related to esophageal dysfunction and histologically by eosinophil-predominant inflammation.1,2 The symptoms of esophageal dysfunction consist of dysphagia, described in terms of discomfort during swallowing, and related symptoms such as food bolus obstruction. Other systemic and local causes of esophageal eosinophilia should be excluded if suspected. Eosinophilic inflammation of the esophagus as an exclusive organ manifestation was first described in the early 1990s.3,4 During the last two decades a considerable rise in this condition has been documented in many parts of Europe and North America. 5 Based on recent meta-analyses, the pooled prevalence of EoE is now estimated at 34.4 cases per 100,000, and was higher for adults than for children (42.2 versus 34 per 100,000). 6 The pooled incidence rates were 6.6/100,000 person-years in children and 7.7/100,000 in adults. EoE is more common in men than women (3:1) and can occur in any age group, with the peak incidence seen between the age of 30 and 40 years. 5 The first description of disease natural history came from Switzerland, in which patients were followed for a mean of 11 years. Continuing or recurring symptoms were seen in most patients, while the disease remained restricted to the esophagus in all cases. 7 More recently, a clear relationship between duration of untreated disease and fibrotic progression was seen.8,9 It is therefore widely accepted that EoE is a long-term, possibly life-long, condition that will require either repeated treatments or some form of maintenance therapy.2,5
The presentation of EoE varies in pediatric and adult patient populations. 10 In young children, symptoms are often variable and may include food refusal, failure to thrive, abdominal pain, heartburn, regurgitation, and vomiting. In adolescents and adults, recurrent dysphagia and bolus obstruction become the most prominent symptoms. In rare cases, spontaneous perforation during bolus obstruction has been described. Indeed, EoE is now regarded as the most common cause for bolus obstruction and spontaneous perforation of the esophagus.11,12 It appears obvious that, depending on the severity of EoE disease, the quality of life of EoE patients is restricted, not only because of the burden of symptoms, but also because of the adaptations they must make in their diet, their social habits, and the difficulties of coping without understanding the direct cause of their symptoms. 13
The diagnostic gold standard of EoE is upper endoscopy with sampling of mucosal biopsies, not only from the esophagus but also from the stomach and duodenum, to rule out other sites with eosinophilic infiltration. 14 According to recent United European Gastroenterology (UEG) guidelines, six biopsies should be obtained from different parts of the esophagus with special attention for visible lesions. 2 The diagnosis of EoE is secured, if an eosinophil-predominant inflammation in any esophageal biopsy is confirmed histologically [>15 eosinophils per high power field (hpf); >48 eosinophils per mm2 hpf] and other obvious causes for eosinophilic eosinophilia are ruled out. 2 In the past, a diagnostic trial with proton pump inhibitors (PPI) has been recommended aiming to rule out GERD or PPI-responsive esophageal eosinophilia. This recommendation has now been abandoned by the recent international AGREE consensus guideline, since extensive clinical and basic research has shown convincingly that PPI-responsive patients are a sub-phenotype of EoE and not a separate disease entity.15,16 Currently, there are no non-invasive biomarkers available that have added value in the primary diagnosis or monitoring of EoE.1,2
Evolution and current role of topical corticosteroids in EoE
Current UEG guidelines recommend swallowed topical corticosteroids (STC), high-dose PPI, or elimination diet for the initial treatment of EoE (Figure 1). 2 For the purpose of this review, only STC will be discussed further. Shortly after the description of the disease, corticosteroids with reduced bioavailability, swallowed instead of inhaled, proved to be equally effective as systemic steroids in inducing clinical and histological remission of EoE in a small series of four children between 12 and 13 years old. 17 The first proof-of-concept study to confirm the efficacy of STC in EoE was a randomized placebo-controlled trial (RCT) in 36 children demonstrating that topical fluticasone administered by an inhaler and swallowed, could achieve histological remission in 50% of patients. 18 In a subsequent randomized study in 80 pediatric EoE patients, topical fluticasone was confirmed to have similar efficacy as systemic prednisolone, whereas prednisolone had many more side effects. 19 The first RCTs on budesonide for induction of remission of EoE were published in 2010, both demonstrating that topical budesonide suspension was superior to placebo in induction of histological remission and symptom improvement in adult and pediatric EoE patients populations.20,21 Over the years, additional RCTs have been conducted, comparing STC with placebo or esomeprazole, or comparing STC in different forms of esophageal delivery for induction of histological remission (Tables 1 and 2). The first RCT evaluating long-term treatment with budesonide suspension for maintenance of remission was published in 2011. 22 In 28 adolescent and adult EoE patients it was demonstrated that low-dose budesonide (0.5 mg per day) was more effective than placebo in maintaining histologic and clinical remission, and was well tolerated. Currently, STC can be regarded as the best studied drug class in EoE, with a total of 16 RCTs including more than 1000 patients (Tables 1–3). The majority of trials have used budesonide or fluticasone preparations originally designed for the treatment of asthma. Other topical corticosteroids, such as beclomethasone or momethasone, have been studied only in small, mostly uncontrolled, trials.23–25
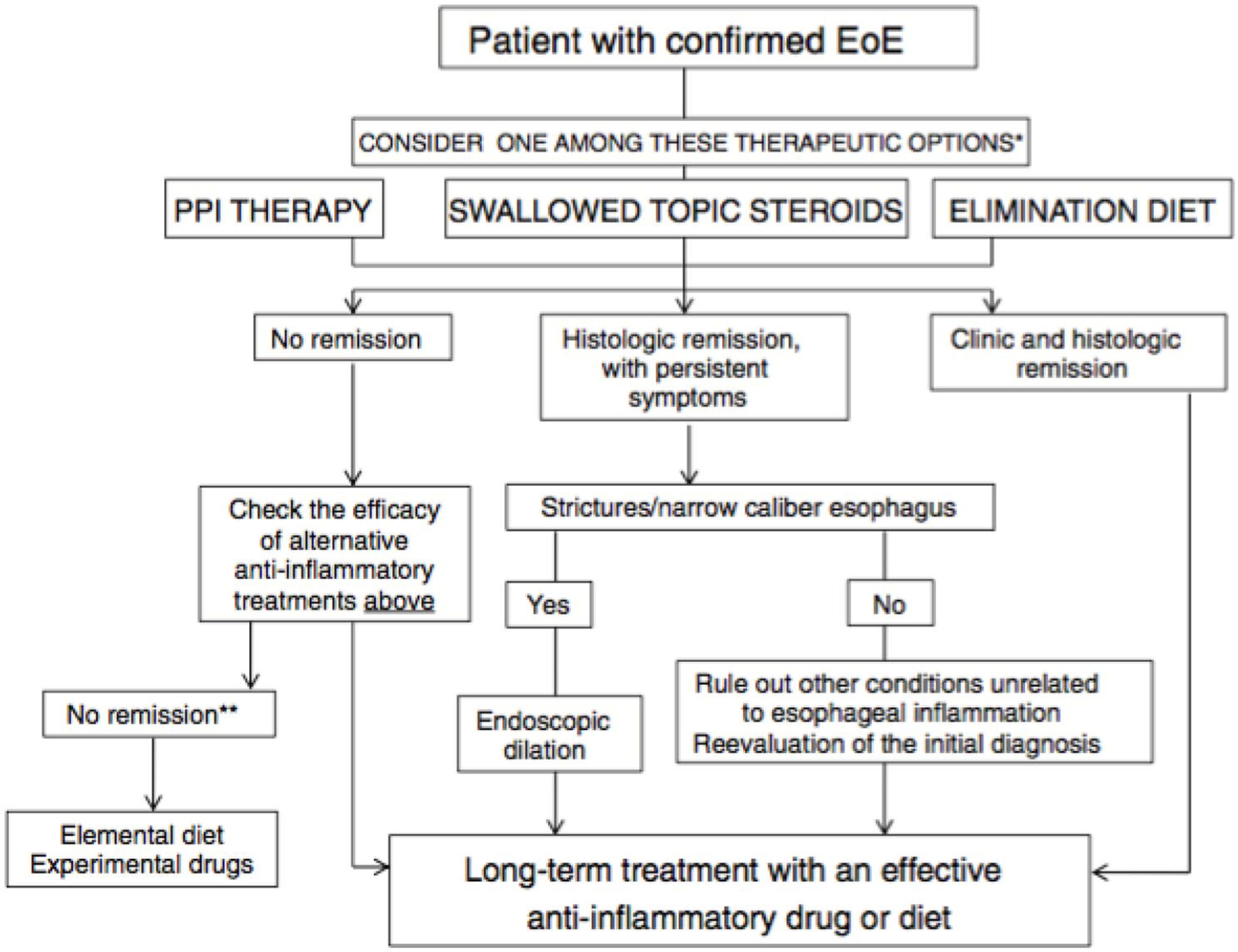
UEG recommendations for treatment of EoE. 2
RCTs on STC compared to placebo for induction of remission in EoE.

EoE, eosinophilic esophagitis; RCT, Randomized controlled trials; STC, swallowed topical corticosteroids.
RCTs on STC compared with X for induction of remission in EoE.

EoE, eosinophilic esophagitis; RCT, Randomized controlled trials; STC, swallowed topical corticosteroids.
RCTs on STC compared to placebo for maintenance of remission in EoE.

EoE, eosinophilic esophagitis; RCT, Randomized controlled trials; STC, swallowed topical corticosteroids.
So far, there have been only a few studies on STC formulations developed specifically for esophageal administration. The orodispersible budesonide tablet with effervescent properties is the first drug to be developed for esophageal targeting, and has meanwhile been approved for the induction treatment of adult EoE patients by the European Medicines Agency (EMA) in January 2018 and is now available in many European countries.
Pharmacokinetic and pharmacodynamic data of budesonide orodispersible tablet
The first pharmacokinetic and pharmacodynamic data of an orodispersible budesonide tablet for buccal administration (3–9 mg daily for 1 week) was generated in healthy subjects and patients with oral graft-versus-host-disease (GVHD). 37 It was shown that only 2% of the buccal dose of budesonide achieved systemic circulation in healthy individuals, whereas the fraction was 10% in patients with oral GVHD, likely because of alterations in drug uptake and CYP3A metabolization. In a subsequent phase I study, pharmacokinetics, CYP3A-dependent metabolites, and endogenous cortisol were studied in 12 adult patients with active EoE and in 12 healthy controls after single and multiple doses of orodispersible budesonide tablets. 38 Plasma budesonide concentration time curves in healthy subjects following single doses of budesonide orodispersible tablets containing either 1 mg, 2 mg, or 4 mg of budesonide are displayed in Figure 2. Systemic exposure to budesonide was lower after administration of orodispersible tablets than after administration of the classical gastroresistant 3 mg capsule formulation. Comparison of budesonide disposition between healthy subjects and patients with active EoE is illustrated in Figure 3. Following the highest single dose of orodispersible budesonide, a significantly higher extent of systemic budesonide exposure and also a significantly longer terminal elimination half-life of budesonide was observed in EoE patients than in healthy subjects. Mean relative bioavailability of budesonide after administration of the 4-mg orodispersible tablet as compared with the 3-mg capsule in patients was not significantly different from the value calculated in healthy subjects. It was further shown that repeated doses of budesonide-containing orodispersible tablets (4 mg/day) over 1 week did not result in systemic drug accumulation. The mean morning serum cortisol levels at baseline and after continuous treatment were similar between healthy subjects (13.27 and 11.70 μg/dl) and EoE patients (13.98 and 11.56 μg/dl). None of the morning serum cortisol values was <5 μg/dl after continuous treatment with the orodispersible budesonide tablet. In summary, suggesting a reassuring safety profile of this new drug delivery mode.

Mean plasma budesonide concentration-time curves in healthy subjects following single doses of orodispersible budesonide tablet.

Mean plasma budesonide concentration-time curves in patients with active EoE and healthy subjects following single dose of budesonide orodispersible tablets 4 mg or budesonide capsule 3 mg.
Phase II clinical trial of budesonide orodispersible tablet
In a phase II clinical trial, the orodispersible budesonide tablet was further studied in 76 adult patients with active EoE in a randomized, placebo-controlled double-blind, double-dummy fashion. 29 The study population consisted of EoE patients with a typical demography (age and gender distribution, atopic comorbidities) and a mean symptom duration of 8.5 years. The median duration of confirmed EoE diagnosis was 2.2 years. Disease activity at baseline was considered moderate, with a peak eosinophil count of 263 per mm2 hpf, a total endoscopic intensity score of 6.0, and a dysphagia score of 4.6.
Budesonide was administered for 2 weeks, either as orodispersible tablet with a dose of 1 mg twice daily or 2 mg twice daily, or as viscous suspension with a dose of 2 mg twice daily, in a concentration of 0.4 mg/ml. The administration and mode of action of the orodispersible budesonide tablet is displayed in Figure 4. The tablet is placed on the tip of the tongue and pressed gently against the hard palate until it completely disintegrates by contact with saliva. The components dissolved in saliva are swallowed stepwise, which take several minutes (2 to 20 min). After drug administration, eating and drinking has to be avoided for 30 min.

Administration and mode of action of the budesonide orodispersible tablet.
The primary endpoint was histological remission at week 2, defined as mean of <16 eosinophils/mm2 hpf, which was achieved in nearly all patients after budesonide treatment (Figure 5). Highly significant decreases in the mean number of eosinophils (eosinophilic load) (Table 4), and the mean peak number of eosinophils were observed for all three budesonide groups in all segments of the esophagus. In addition, significant improvements of the endoscopic appearance based on a semiquantitative score and a visual analogue scale were observed. The active treatment was safe and well tolerated. Local and mostly asymptomatic candidiasis occurred in only 10% of budesonide-exposed patients. At the end of treatment, the majority of patients decided that, based on handling, taste, and comfort, they would prefer the orodispersible tablet for long-term treatment of their EoE, whereas only some patients voted for the viscous suspension (Figure 6).
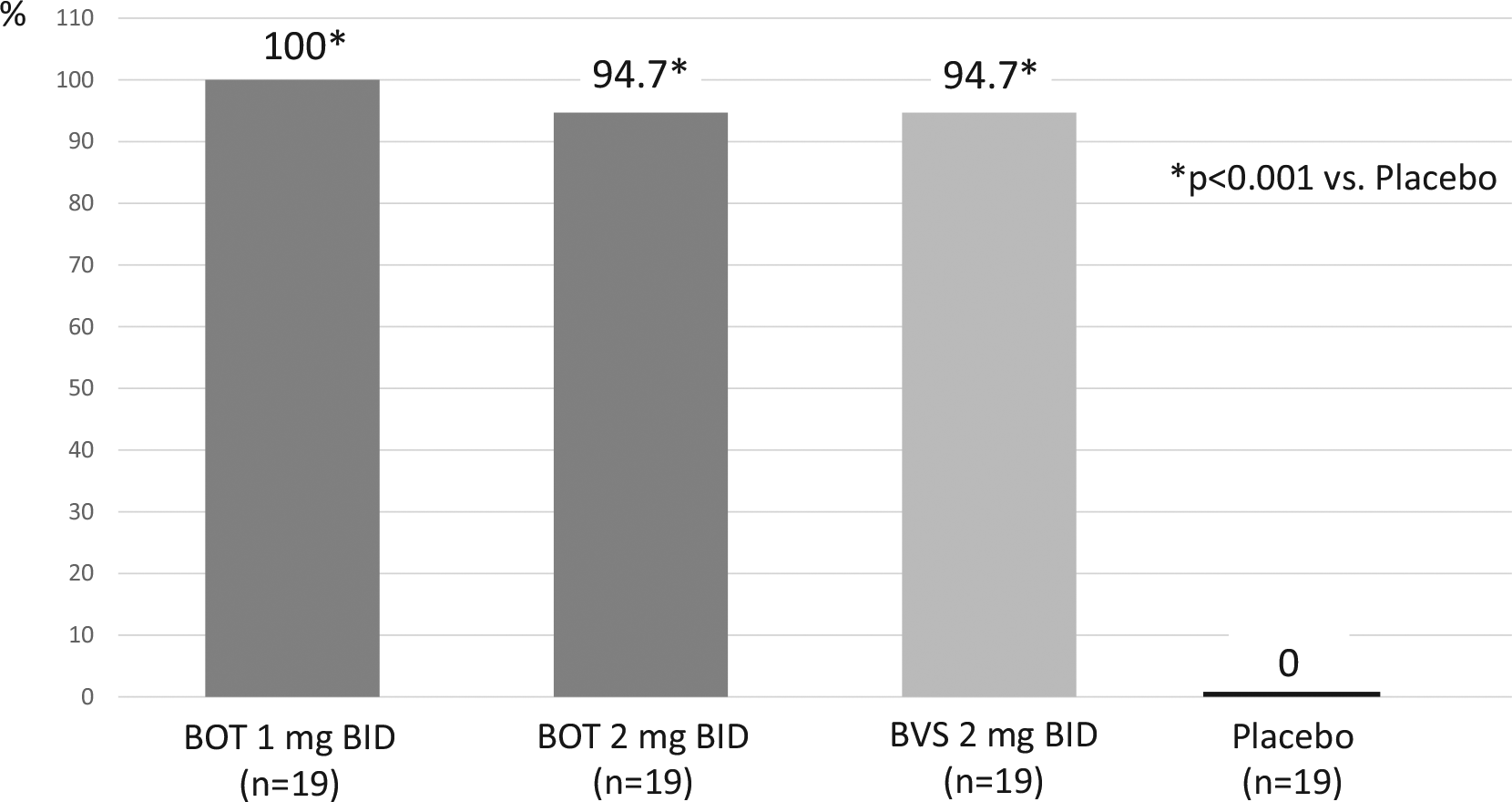
Histologial remission (%) after 2 weeks of BOT or BVS in active EoE (phase II). 29
EoT with budesonide adminstered as orosdispersible tablet (BOT1: 1 mg BID, BOT2: 2 mg BID) or viscous suspension 2 mg BID (BVS) on eosinophilic load by esophageal segment. 29

BID, twice daily; BOT, budesonide orodispersible tablet; BVS, budesonide viscous suspension; eos, eosinophils; EoT, effect of treatment; hpf, high power field.
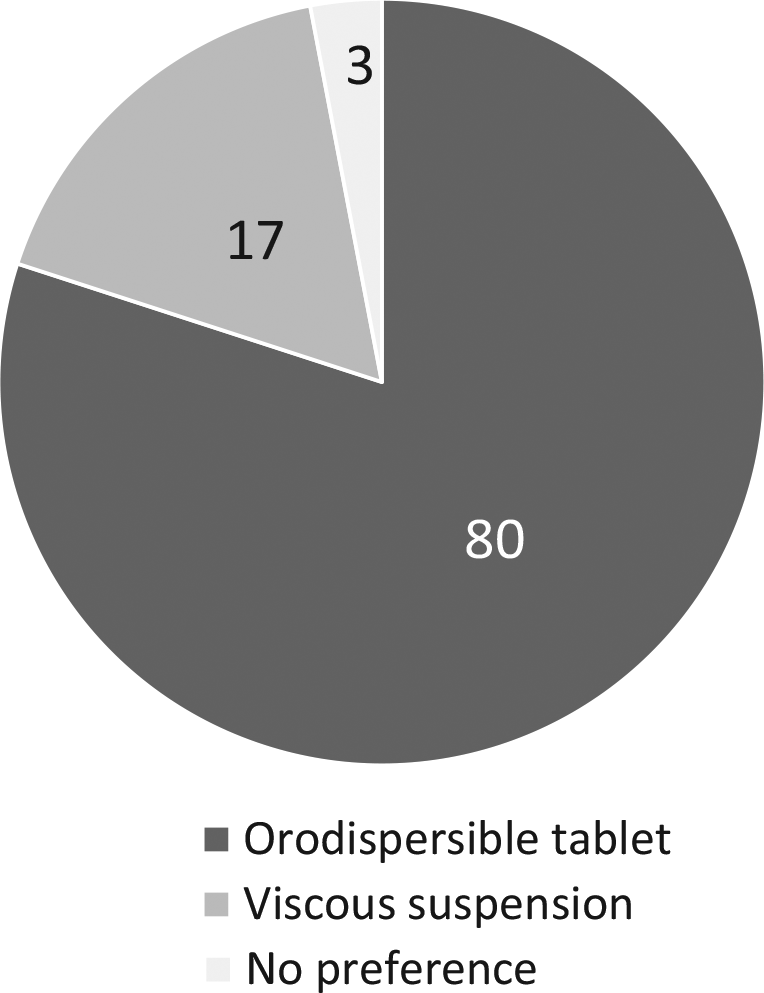
Patient’s preference (%) for long-term treatment of their EoE. 29
In a sub-study of this phase II trial, several EoE-associated blood and serum markers were studied in order to non-invasively monitor the response to treatment with topical budesonide. 39 A highly significant decrease of absolute blood eosinophil counts (AEC), serum levels of CCL-17, CCL-18, CCL-26, eosinophil-cationic-protein, and mast cell tryptase was observed after 2 weeks of treatment with budesonide, but not with placebo. Among these candidates, the absolute blood eosinophil counts significantly correlated with esophageal eosinophil density before and after budesonide treatment, and their post-treatment values were associated significantly with histological remission. Unfortunately, the use of AEC as non-invasive marker of EoE’s inflammatory activity is hampered by the lack of its specificity. Therefore, it cannot be used for monitoring of EoE.
Phase III program of the orodispersible budesonide tablet in EoE
Based upon the high efficacy and the patient preference observed in the phase II trial, the orodispersible budesonide tablet was enrolled in a multicenter European phase III program for adult patients with active EoE. This program included a placebo-controlled induction of remission trial (EOS-1), a 48-week placebo-controlled maintenance of remission trial with open-label induction (EOS-2), and an open-label extension phase of maintenance therapy for another 96 weeks (Figure 7). The program is finished and some parts of it have already been published as full paper or in abstract form at time when this review article was written.

Phase III program of BOT in adult patients with active EoE.
Induction treatment of EoE (EOS-1)
In the EOS-1 trial, 88 adult patients with active, PPI-refractory EoE (medical history of PPI used at least in standard dosages for at least 4 weeks) were randomly assigned to treatment with budesonide orodispersible tablet (BOT) 1 mg twice daily or placebo for 6 weeks. 31 Now onset of dietary restrictions within 4 weeks before screening was an exclusion criteria and new dietary changes were not permitted during the trial. Active disease was defined as having a severity of at least 4 points on a 0–10 numerical rating scale (NRS) for either dysphagia or odynophagia for at least 1 day in the week before randomization, a Patient’s Global Assessment Score (PatGA) of at least 4 points on a 0–10 NRS, and histological activity with peak eosinophils of at least 65 per mm2 hpf in at least 1 hpf (corresponding to at least 20 eos/hpf), as measured in a total of 6 hpfs derived from six biopsies, two each from the proximal, mid, and distal segments of the esophagus. The patient cohort included into this trial was typical for EoE with respect to age, gender and atopic comorbidities, and clinical appearance. Disease duration based on symptoms was more than 11 years, with a history of confirmed EoE diagnosis of 4.5 years (mean). Dysphagia was assessed by a numerical rating scale (NRS 0–10) and scored 5.9 at baseline. The clinical disease activity was also assessed by the validated EEsAI-PRO (patient reported outcome), 40 and was moderate at baseline with a score of 55.5. More than 80% of patients showed a moderate-to-severe endoscopic activity with about 75% of patients having a pan-esophagitis. The mean peak number of eosinophils was around 240 per mm2 high power field (hpf).
The primary combined endpoint “clinico-histological remission” (defined as dysphagia ⩽2 points + odynophagia ⩽2 points + peak eosinophils of <16 eos/mm2 hpf) was achieved in 57.6% of patients receiving orodispersible budesonide and none of the placebo recipients (Figure 8). Patients who were not in clinico-histological remission after 6 weeks of double-blind treatment, were further treated with open-label BOT 1 mg BID for another 6 weeks. After 12 weeks of active therapy, the proportion of patients with clinico-histological remission reached 85% (Figure 8). In a post hoc analysis, a higher dysphagia score and a higher patient global assessment of disease activity have been identified as significant predictors for a delayed treatment response. 41

Induction of remission rates (ITT) with BOT after 6 and 12 weeks (double blind EOS-1). 30
Several a priori ordered secondary endpoints were analyzed including histological remission and clinical remission at week 6, which was achieved in over 90% (in all three segments of the esophagus), and in 59% of BOT patients versus 0% and 14% in placebo recipients (Figure 8). Further secondary clinical endpoints included the EEsAI-PRO complete resolution of dysphagia; days per week with no, or minimal, dysphagia; and patient’s global assessment of disease activity, which all were significantly improved after 6 weeks with BOT compared with placebo. Endoscopic remission at week 6 was documented in 61% of BOT recipients and in none with placebo. Administration of BOT was safe and well tolerated over 6 and 12 weeks, with 5% of patients developing symptomatic, mild oral and/or esophageal candidiasis, which was treated easily with local antimycotic agents. The proportion of patients with local candidiasis was well in the range of other clinical trials of topical corticosteroids in adult and pediatric EoE.
In a further post hoc analysis, most stringent criteria for deep remission of EoE as proposed by Greuter et al. 42 have been studied. 43 These included deep clinical remission (complete absence of dysphagia and odynophagia), deep histological remission (0 eos per mm2 hpf), deep endoscopic remission (no endoscopic signs of EoE), and deep disease remission (combination of deep clinical, deep histological and deep endoscopic remission). This post hoc analysis revealed that even the criteria of deep remission can be achieved in a substantial proportion of patient already after 6 weeks of treatment with the BOT (Figure 9).

Most stringent criteria of deep remission criteria in EoE after 6 weeks treatment with BOT. 42
Open-label induction and double-blind maintenance treatment of EoE (EOS-2)
In the EOS-2 trial, 181 adult patients with active EoE were enrolled to open-label BOT 1 mg BID for 6 weeks. 44 The patient population was very similar to the EOS-1 population with respect to demographic and disease activity characteristics. Clinico-histological remission was achieved in 126 patients (69.6%) (Figure 10). Histological remission was documented in 90.1% and clinical remission in 75.1%, confirming the high efficacy of BOT for induction of remission in active EoE observed in the EOS-1 trial.

Induction of remission (ITT) with open-label BOT after 6 weeks (EOS-2). 43
A total of 204 adult EoE patients with confirmed clinico-histological remission after treatment with BOT were randomized to maintenance treatment with either BOT 1 mg BID or BOT 0.5 mg BID or placebo for 48 weeks. 36 The primary endpoint of this trial was the proportion of patients free of treatment failure after 48 weeks or double-blinded treatment, defined as absence of clinical of histological relapse, absence of food bolus impaction requiring endoscopic intervention or need for dilation. This endpoint was achieved in 75.0% and 73.5% of patients with BOT therapy and in only 4.4% of patients with placebo (each p < 0.0001). This was closely mirrored by the proportion of patients in remission as assessed by the EEsAI-PRO. There was no statistical or clinical meaningful difference between the two BOT groups, suggesting that clinico-histological remission can be maintained effectively by low-dose of BOT. Long-term treatment with BOT was well-tolerated and safe. Suspected symptomatic candidiasis was reported in 11–16% of patients, which, in all cases, was treated easily with local antimycotic therapy and did not lead to discontinuation of BOT therapy. In addition, no clinically relevant changes in morning serum cortisol levels or in levels of bone metabolism markers were observed.
Additional analyses of endoscopic findings revealed that deep endoscopic remission, as defined by Greuter et al. 42 was maintained effectively in significantly more patients with BOT therapy (79.2% and 71.1%) compared with placebo (8.5%). 45 Finally, long-term therapy with BOT was superior over placebo to maintain and further improve quality of life as assessed by the validated EoE-QoL-A questionnaire. 46
Discussion and future perspectives
EoE is a relativly new disorder, which was not described in text books at the time current practicing gastroenterology consultants were at medical school or in clinical training. Therefore, many parts of the medical community are currently not familiar with taking care of patients with EoE. A recent survey of United States (US) gastroenterologists has shown how variable the gastroenterologists clinical approach is to EoE, with variation in the numbers of biopsies, the standard of numerical counting of epithelial eosinophils, and the timing of interventions and their follow up. 47 Future work needs to identify ways to correct the diagnostic knowledge base amongst the wider community of gastroenterologists and primary care professionals. Education by specialist societies is a key strategy to address this.
Until now, there was no single strategy of therapy that held a clear advantage in the primary therapy of EoE, and, therefore, the choice of initial therapy was often left up to patient choice, without medical guidance. Again, recent surveys of gastroenterologists in the US and Germany suggest that treatment decisions are also often very discordant with published guidelines.47,48 Among all options for medical treatment of EoE, STC are the most efficient, have a good safety profile, and should therefore be considered as first-line medication for induction- and maintenance treatment. Among all STCs, BOT appears to be superior compared with the off-label formulations used. Under the conditions that BOT is approved by the regulatory authorities and reimbursed by local health insurances, we recommend that BOT be used as first-line STC in adult EoE patients. If these conditions are not yet fullfilled, off-label use of topical corticosteroids designed for airway application are a possible alternative.
An alternative drug therapy for EoE is PPI, which, however, appears to be less effective compared with topical corticosteroids. Two RCTs compared esomeprazole and fluticasone and suggested similar efficacy; however, both studies appear to have several methodological weaknesses.32,34 A metaanalysis on PPI in EoE included 33 studies, with 22 of them being retrospective, and none placebo controlled. 49 Based on 619 patients, the rate of histological remission was 50.5% and the clinical response rate was about 60%. However, the authors of the metaanalysis concluded that these findings should be interpreted with caution because of poor quality of evidence, heterogeneity, and publication bias. A recently published analysis of 589 patients from a European EoE registry found a clinical+histological remission rate with first-line PPI therapy (50.2%) compared with first-line therapy with topical corticosteroids (67.7%) in real-world practice. 50
Finally, there is still the option of a dietary approach rather than drug therapy, as the only therapy that targets the cause of EoE, if a patient shows a desire once they have understood what it entails. It may be that using a step-up approach of two common foodstuffs excluded first, and if that is successful (in the expected 40%) then a certain number of patients may adopt an exclusion diet of milk and dairy products and/or wheat and gluten, which is cheap, accessible, and practical in terms of clinical follow up. More complex diets that exclude four or even six food groups, followed by the sequential reintroduction of each food excluded under endoscopic monitoring in case of clinico-histological response, potentially identify food triggers of EoE in each particular patient. However, this approach is associated with high costs in terms of research, and, if several culprit foods are identified, they will prove very impractical in terms of leading a normal dietary lifestyle. 51
It is not yet clear if all patients with EoE need maintenance therapy or if the long-term use of orodispersible budesonide can be reserved for patients with severe disease or for those only after their first relapse. Such decisions have important implications in cost containment in struggling healthcare economies. Having a clear measure of disease severity, and thresholds for initiating induction and maintenance therapy with orodispersible budesonide are important aspects of clinical care in EoE that need to be addressed.
Because symptoms and inflammation do not run in parallel, and clinical response does not guarantee histological remission, it is currently standard that patients should undergo a follow up endoscopy with biopsy after initiation of a new therapy or after a significant change in the treatment strategy. Treating physicians, as well as patients, must be aware of the goals they already have achieved or have not achieved with their already performed measures. The question of how often further endoscopic controls are needed is not yet clear. Because endoscopies are invasive and expensive, the indication for a follow up examination is currently often reappearance of symptoms. In the future some less-invasive tools – for example, the esophageal string test or the esophageal cytosponge – might help to solve this problem.52,53 However, more work must be done in order to determine the role of these tools in the long-term monitoring of EoE.
Until now there has been a major focus on trying to identify a third line of therapy to be used for those patients who frequently failed PPI therapy and unlicensed non-specific topical steroid therapy. These have included numerous biologic agents, often with great expense and very demanding schedules of dose administration. Now, with effective first-line therapy, backed up by effective maintenance therapy, new goals should be defined for research into other agents.
Footnotes
Funding
S. Miehlke und S. Attwood received financial support for the research, authorship, and/or publication of this article by Dr. Falk Pharma.
Conflict of interest statement
SM has received speaker and/or consulting fees from Dr. Falk Pharma, Falk Foundation, Celgene, and Esocap. AJL has received research funding from Dr. Falk Pharma. AS is a consultant for Calypso, EsoCap, Dr Falk Pharma GmbH, GSK, Receptos-Celgene, Regeneron-Sanofi, Shire, and Tillotts, and has received speaker fees and research funding from Dr Falk Pharma GmbH. AJB has received research funding from Nutricia, Norgine, and Bayer, and received speaker and/or consulting fees from Laborie, EsoCap, Diversatek, Medtronic, Dr Falk Pharma GmbH, Calypso, Thelial, Regeneron, Celgene, Bayer, Norgine, AstraZeneca, Almirall, and Allergan. SA has received speaker and consulting fees from Dr Falk Pharma GmbH.