
Abstract
The association of eosinophilic esophagitis and esophageal polyps has been reported in the literature but remains a rare finding in both adults and children. The patient in this case report presented with progressively worsening dysphagia secondary to eosinophilic esophagitis and an esophageal polyp. Dysphagia is always abnormal, and endoscopic evaluation is essential. Dysphagia is a well-known symptom in patients with eosinophilic esophagitis. While esophageal polyps as a whole are less common in the pediatric population, they should not be overlooked as a possible cause of dysphagia and esophageal obstruction.
Introduction
In this case report, an adolescent boy presented with dysphagia and was found to have eosinophilic esophagitis (EoE) and an esophageal polyp. The polyp in this case was inflammatory, had a stalk, and contained eosinophils. This lesion, including the inflammation in EoE, can cause physical obstruction and altered esophageal peristalsis, resulting in dysphagia. EoE typically presents with food impaction, dysphagia, abdominal pain, persistent reflux, and unusual eating behaviors like drinking excessive amounts of water to swallow food or over chewing. 1 It may also be associated with asthma, food allergies, seasonal allergies, or eczema. 1 Rates of EoE in the United States and worldwide are increasing. EoE is a chronic, relapsing condition that affects about 56.3 per 100,000 people per year. 2 The finding of polyps with EoE has been reported in the literature but is a rare finding.
There are many types of polyps in the gastrointestinal tract (GIT). Polyps can be categorized as inflammatory, hamartomatous, or adenomatous polyps. 3 Upper GIT polyps have been associated with dysphagia as well as dyspepsia, bleeding, anemia, abdominal pain, and gastric outlet obstruction. 4 The incidence of upper GIT polyps is low, particularly in the pediatric population. GIT polyps often occur with polyposis syndromes such as juvenile polyposis or familial adenomatous polyposis. In a study including 5766 children, only 45 (0.8%) were found to have a polyp, and typically they were hyperplastic-inflammatory polyps. 5 Hyperplastic polyps are abnormal growths of gastric-type foveolar epithelium, squamous epithelium, or both. 6 These polyps are often associated with gastroesophageal reflux (GERD) or hiatal hernias.5,7 However they have also been found with EoE, inflammatory bowel diseases, or neurofibromatosis type 1. 5 Comparatively, in a case series of seven individuals with esophageal polyps, two were noted to have EoE. 5 Hyperplastic polyps of the esophagus and the esophagogastric junction (EGJ), although benign, have been associated with mucosal damage.6,7 There are two other cases in the literature associating EoE and esophageal polyps with either eosinophils or hyperplastic fibrous changes.8,9 Histologically, hyperplastic polyps are filled with plasma cells, eosinophils, fibroblasts, and inflamed stroma. 7 Therefore, it can be concluded that any condition that causes repeat mucosal injury can produce these polyps, including EoE. Although a rare finding, the association of polyps and EoE has been published. However, the literature lacks treatment guidelines for polyps associated with EoE. No direct evidence has been observed regarding the resolution of polyps with antacid therapy in children. 5 There have been reports of improvement of hyperplastic polyps with proton pump inhibitor (PPI) treatment in adults. 7 Treating the inflammation or reducing the injury will likely resolve the polyp.
The literature and current management of both polyps and EoE were reviewed to assist clinicians in the management of these combined clinical findings.
Case report
The patient was a 16-year-old male with a past medical history of allergic rhinitis, reflux, and seasonal allergies who presented to a pediatric gastroenterology clinic with a 2-year history of dysphagia and recurrent choking episodes after all meals. Initially, this sensation only occurred with meat or chicken; however, it worsened while including other foods such as waffles. Due to the dysphagia, the patient was scheduled for an upper endoscopy without starting any acid blockers. The endoscopy revealed esophageal edema, furrowing of the mucosa, and an esophageal polyp in the distal esophagus near the gastroesophageal junction (Figure 1). Biopsies obtained showed significant esophagitis with greater than 60 eosinophils per high-power field (eos/hpf) in the distal esophagus and greater than 80 eos/hpf in the mid-upper esophagus (Figure 2). The surface of the polyp was separately biopsied, and the sample was also sent for viral culture. The viral culture was negative, and the histology was negative for atypical malignant cells. A total of 7 eos/hpf was noted in the esophageal polyp (Figure 3).
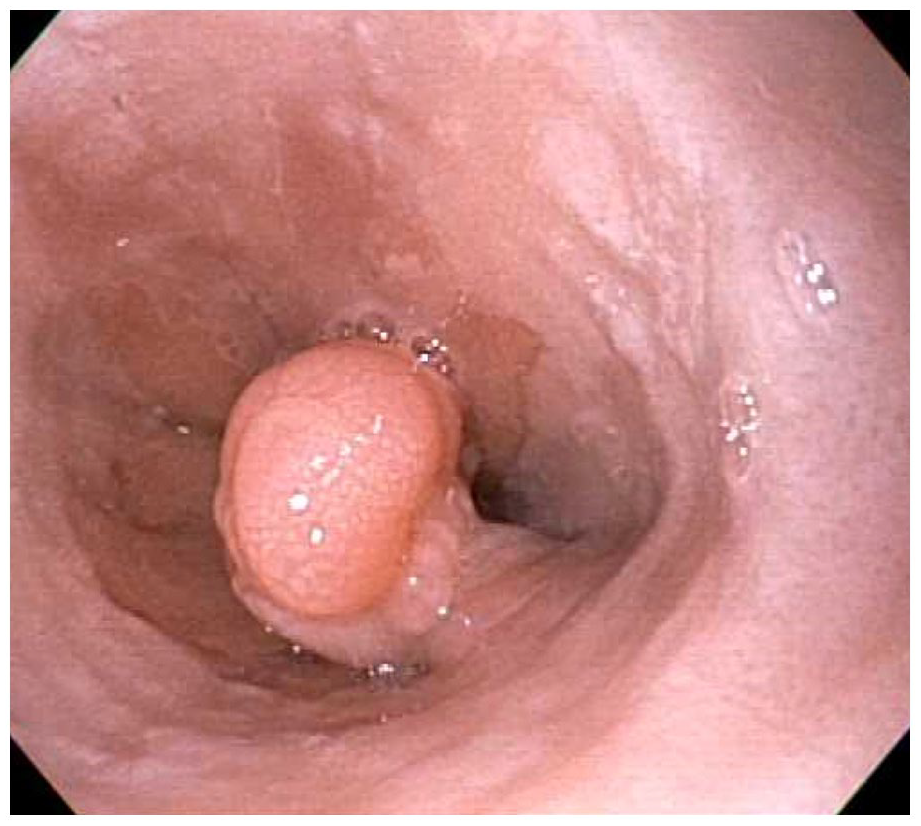
Polyp located in distal esophagus near gastroesophageal junction prior to starting treatment. Note typical mucosal findings of EoE surrounding the polyp which include furrowing and edema.

Histology of the esophagus before treatment. Blue arrows indicate eosinophils. Proximal esophagus (a) contained greater than 80 eosinophils per high-power field. Distal esophagus (b) contained greater than 60 eosinophils per high-power field ((a) and (b) resolution 200×).

Histology of the polyp before treatment. Blue arrows indicate eosinophils, with maximum 7 eosinophils per high-power field. Ulcerations, fungus, and viral inculsions were not seen. No glandular mucosa was present (resolution (a) 20×, (b) 200×).
The patient was started on omeprazole 40 mg once daily and topical budesonide (concentration of 0.5 mg/2 mL nebulizing respule) 1 mg or 4 mL mixed with 2 tsp table-sugar twice daily. He was referred to allergy/immunology for further evaluation. Diet elimination was not started as per patient preference.
The patient was seen 3 weeks after the initiation of treatment and reported feeling better. He denied nausea, vomiting, regurgitation, abdominal pain, chest pain, weight loss, dysphagia, choking episodes, or new adverse events. Approximately 5 months after starting the omeprazole and budesonide, a repeat upper endoscopy was performed. The histology showed 1 eos/hpf in both the distal and mid-upper esophagus (Figure 4), and persistent 7 eos/hpf in the esophageal polyp (Figure 5). However, the polyp has reduced in size since the last procedure (Figure 6).

Histology of the esophagus after treatment. Blue arrows indicate eosinophils. Proximal esophagus (a) contained 1 eosinophils per high-power field. Distal esophagus (b) contained 1 per high-power field ((a) and (b) resolution 200×).

Histology of the polyp post treatment with proton pump inhibitor and swallowed steroids. Blue arrows indicated eosinophils, with maximum 7 eosinophils per high-power field. Ulcerations, fungus, and viral inclusions were not seen. No glandular mucosa was present (resolution (a) 20×, (b) 200×).

Polyp located in distal esophagus near gastroesophageal junction, has flattened and reduced in size after treatment with proton pump inhibitor and swallowed steroids.
Discussion
EoE involves a TH-2 cell response that activates allergic cytokines of IL-4, IL-5, and IL-13. 10 The diagnosis must be confirmed histologically. Often, there are pre-existing symptoms and a history suggestive of allergic diseases. Unfortunately, blood or skin allergy testing does not provide accurate information about the allergic triggers. 11 Diagnosis is confirmed with the finding of greater than 15 eos/hpf on endoscopy and esophageal biopsies. 11 If the patient meets histologic criteria while off of PPI, they are placed on PPI treatment for 8 weeks. Following this trial, patients are advised to have an additional endoscopy with biopsies. If at this point, there are still greater than 15 eos/hpf, they are considered to have EoE. 11 If there is resolution of the eosinophils after proton pump inhibitors the diagnosis can either be acid reflux or PPI-responsive-EoE. 11
Due to the chronic inflammatory nature of EoE, patients often develop subepithelial fibrosis and esophageal wall thickening. 12 This inflammation is suggested to lead to other common findings such as edema, white exudates, furrows, lacerations, and strictures seen during endoscopy. 13 More recently, new technologies such as the functional luminal imaging probe (EndoFLIP™, Minnesota, MN) have evolved aside from endoscopy to diagnose EoE by assessing the esophageal diameter and elasticity. 14 It does so by measuring the distensibility plateau, which represents the most constricted area along the esophagus by exhibiting its resistance to additional expansion with an increase in balloon pressure. 14 Stationary manometry is less sensitive; it may either be normal or display static, narrowed caliber. 12 Of 49 patients with eosinophilic esophagitis studied, only 41% had abnormal esophageal manometry. 12 This includes uncoordinated contractions (30%) with or without LES relaxation, hypercontraction (7%), and ineffective peristalsis (4%). 12 This dysmotility may be attributed to acetylcholine activation via histamine release from mast cells in the esophageal wall. 15 Currently, the gold standard is histologic evaluation with upper endoscopy. There are some centers looking at the utility of trans-nasal endoscopy in children as a cost-effective test that does not need anesthesia. 16 The string test is another less invasive test that has been shown to have a good correlation with esophageal histological changes in EoE. 17 A string is attached to a capsule that is swallowed, and the string is held outside the mouth. 17 After 1 hr, the string is pulled and the capsule with the inflammatory mediators like eotaxin-2 and 3 are analyzed. 17
To date, we have not found an article specifically outlining the treatment of esophageal polyps associated with EoE. In this case, the swallowed steroids did appear to help reduce the size of the polyp, although the number of eosinophils was not reduced. Overall management of EoE includes swallowed steroids, biologics, food elimination, and elemental diets.
PPIs are often started and show improvement in a subset of patients, termed “PPI responsive EoE.” 18 PPIs inhibit TH-2 cytokine-stimulated eotaxin-3 secretion in esophageal epithelial cells, therefore reducing eosinophils in the esophagus. 18 The current adult American Gastroenterological Association (AGA) guidelines for EoE highly recommend a long-term proton pump inhibitor, which is usually prescribed along with a swallowed topical glucocorticosteroid such as budesonide or fluticasone. 11 In a study looking at the efficacy of budesonide and fluticasone, both steroids were highly effective for the treatment of EoE. 19 However, there was no statistically significant difference in the efficacy of the two steroids when compared. 19 Recently, drug manufactures have been developing steroid tablets formulated for EoE. The topical steroids swallows that are used for EoE currently are off-label uses of typical pulmonary medicines for asthma. Currently, there isn’t a set timeline for treatment and or weaning of these medications by the AGA. There are on-going studies looking at the safety of these medicines long term in children. In clinical practice, both proton pump inhibitors and swallowed topical glucocorticosteroids are continued for years if the patient responds adequately. There have been several articles describing adrenal insufficiency after prolonged oral glucocorticoid intake for EoE.20–25 These effects are more pronounced when the patient is on additional steroids for conditions like atopic dermatitis, asthma, or allergic rhinitis. 25 Adrenal insufficiency has been seen with both oral budesonide and fluticasone propionate. 23 Long-term side effects of PPI include increased rates of infections, vitamin deficiencies (calcium, magnesium, B12, and iron), bone fractures, anemia, dementia, and kidney disease. 26 It is important for the clinician to be aware and monitor for these side effects, especially since patients with EoE will remain on these medicines for months or years.
Food elimination diets are geared toward achieving healing and based on patient preference, slowly reintroducing foods individually. While elemental diets have been reported to have a remission rate of 90.8%, they are also found to be the most dramatic in terms of lifestyle management. 27 Long-term compliance, therefore, can be an issue with elimination diets. Elemental diets consist of an amino-acid-based formula only diet; like food elimination, once healing is observed, there is the opportunity to systematically reintroduce foods, followed by endoscopy.
More recently, biologic agents, such as dupilumab, have been found to be effective in targeting the treatment-refractory population of patients with EoE. 10 Dupilumab has shown excellent results in adults in a study published January 2020.10,28 Dupilumab was recently approved in the United States for the treatment of EoE in 2022 for children ages 12 and older. This biologic may become the preferred therapy in patients with EoE with polyps because good results have been seen in similar conditions like chronic rhinosinusitis with nasal polyps. 29 Other monoclonal antibodies including interleukin-5 (IL-5), interleukin-13 (IL-13), integrins, and siglec-8, have shown promise in trials but are not FDA approved yet for the treatment of EoE in children. 10 It will be interesting to see which of these medications will be the most effective for the treatment of patients with EoE and esophageal inflammatory eosinophilic polyps.
Currently, there is a paucity of literature regarding surgical resection of hyperplastic esophageal polyps in children. The resection can be technically difficult and there may be a high risk of perforation. Typically, medical therapy is exhausted in children before such procedures are considered. In adults, there are many articles outlining the endoscopic and surgical removal of fibrovascular polyps.30–33 There is also a case report of a successful endoscopic mucosal resection of hyperplastic polyps secondary to Barrett’s esophagus with the finding of low-grade dysplasia. 31 The patient for this case report did not have signs of Barrett’s esophagus or low-grade dysplasia. This is why medical therapy was recommended over endoscopic resection. The role of endoscopic/laparoscopic anti-reflux therapy is not indicated in EoE.
Conclusion
Esophageal polyps associated with EoE have been rarely reported in adults and children. In this case, treatment with swallowed steroids and PPI helped reduce the size of the esophageal polyp in an adolescent boy with EoE. Swallowed steroids may help treat esophageal polyps associated with EoE. Potentially, biologic therapy may be a more effective treatment for polyps found in patients with EoE. Further studies are needed to identify the most effective treatment for this condition.
Footnotes
Acknowledgements
Jeffrey Zacks, MD, is the pathologist who assisted with Figures 3–![]() in this article. The authors acknowledge his contribution to this article.
in this article. The authors acknowledge his contribution to this article.
Author contributions
S.K. provided supervision, expertise on the topic, idea creation, and was the corresponding author. B.S. and S.K. did article writing and editing. S.K. obtained endoscopic images. P.B., D.R.N., M.W. and J.N.K. did clinical data acquisition and article editing. All authors read and approved the final article.
Availability of data and material
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent for publication
Ethics approval was waived due to the nature of the article as a case report. Our institution does not require ethical approval for reporting individual cases or case series. Written informed consent was obtained by the parents for the patient who is under 16 years old in order to publish this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.