
Abstract
Background:
Early fluid resuscitation is one of the main therapeutic strategies for acute pancreatitis (AP). This study investigated the effects of early aggressive and nonaggressive hydration on AP.
Objectives:
The aim of this meta-analysis is to investigate the differences between aggressive and nonaggressive intravenous fluid resuscitation in AP.
Design:
This study was based on publicly available data, all of which have been extracted from previous ethically approved studies.
Data sources and methods:
Two authors systematically searched PubMed, Embase (via OVID), Web of Science, and Cochrane Library to find all published research before February 2023. In-hospital mortality were set as primary endpoints.
Results:
This meta-analysis included seven randomized controlled trials (RCTs) and eight cohort studies with 4072 individuals in nonaggressive (n = 2419) and aggressive (n = 1653) hydration groups. The results showed that patients in the nonaggressive group had a lower mortality rate than those in the aggressive hydration group [relative risks (RR), 0.66; p = 0.02]. Subgroup analysis results showed that patients in the nonaggressive hydration group had lower mortality rates in RCTs (RR, 0.39; p = 0.001), studies conducted in Eastern countries (RR, 0.63; p = 0.002), and studies with severe pancreatitis (RR, 0.65; p = 0.02). In addition, the nonaggressive hydration group had lower rates of infection (RR, 0.62; p < 0.001), organ failure (RR, 0.65; p = 0.02), and shock (RR, 0.21; p = 0.02), as well as a shorter hospital stay (weighted mean difference, −1.63; p = 0.001) than the aggressive hydration group.
Conclusions:
Early nonaggressive fluid resuscitation is associated with lower mortality, lower risk of organ failure and infection, and shorter hospital stays than aggressive fluid resuscitation.
Registration (prospero registration number):
CRD42023396388.
Introduction
Acute pancreatitis (AP) is an inflammatory condition of the pancreas, which can lead to a syndrome of local and systemic inflammatory responses, as well as organ failure.1,2 The incidence of AP and hospitalization have been increasing over the last 20 years. 3 The etiology of AP includes, but is not limited to, pancreatic duct obstruction secondary to gallstones, alcohol, endoscopic retrograde cholangiopancreatography (ERCP), and various drug-induced pathological cellular pathways and organelle dysfunction that that ultimately characterize AP.4,5 The clinical course of the disease varies and can be categorized as mild, moderately severe, or severe. Most patients are suffering from mild conditions with only interstitial changes in the pancreas.6,7 Around 20% of cases will present with moderate or severe episode of AP, accompanied by necrosis of the peripancreatic or pancreatic tissue or organ failure, or both, and a mortality rate of 20–40%.8,9
Intravenous fluid (IVF) resuscitation, oxygen, analgesia, and nutrition are the fundamental managements for AP. 10 Fluid administration can counteract tissue hypoperfusion and third-space volume loss without causing pancreatic and systemic hemodynamic deterioration in the inflammatory cascade.11,12 It is widely recommended by several guidelines and is highlighted as a pivotal therapeutic strategy. However, the evidence is limited and recent guidelines12,13 suggest that IVF should be guided with caution as fluid overload is known to exacerbate tissue edema and impact impaired oxygen delivery. 14
A number of randomized controlled trials (RCTs) have now explored strategies for IVF,15–18 the results of which are controversial and remain inconclusive. Some studies17,19–22 have demonstrated that aggressive fluid administration is associated with better outcomes in treatment of AP, while some of these studies16,18,23 have showed no significant difference between aggressive and nonaggressive outcomes. In addition, it has been argued that the risk of fluid overload must be taken into account when aggressive IVF is performed. 15 Therefore, the aim of this meta-analysis is to gather and summarize relevant data to investigate the differences between aggressive and nonaggressive IVF resuscitation in AP.
Methods
This study was performed in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-analysis of Observational Studies in Epidemiology reporting guidelines. 24 This study was based on publicly available data, all of which have been extracted from previous ethically approved studies. The protocol of this study had been registered in the International Prospective Register of Systematic Reviews under the registration number of CRD42023396388.
Literature search strategy
Two investigators independently performed a systematic literature search in PubMed, Embase (via OVID), Web of Science, and Cochrane Library to find all publicly published research. The following search terms were used: (pancreatitis OR pancreatic OR pancreas OR acute pancreatitis) AND ((Ringer's OR Hartmann’s) OR (resuscitation OR fluid therapy OR fluid administration OR hydration OR hemodilution)). The search strategy for all databases is shown in Supplemental Table S1. The latest search was performed in February 2023. In addition, a manual search of references in the relevant literature was conducted to provide a comprehensive review of potentially relevant studies. 25
Inclusion and exclusion criteria
The studies were chosen on the basis of the following criteria: (a) the type of study falls under the category of RCTs or cohort studies. (b) The study reported on the outcomes of patients with AP who received aggressive hydration versus those who received non-aggressive hydration. Strictly speaking, aggressive hydration is defined as an infusion of isotonic crystal solution greater than 250 mL/h (or greater than 5 mL/kg/h). However, due to record limitations, patients receiving fluid volume (FV) greater than 4 L or more than 1/3 of the total 72 h FV within the first 24 h in observational studies were also considered to meet the guideline definition of aggressive IVF therapy.1,26
Exclusion criteria: (a) the research was published as conference abstracts, case reports, or narrative reviews; (b) the research reported only one group of outcomes or did not clearly distinguish between aggressive and nonaggressive IVF; (c) the study was not written in English; (d) the data from the study could not be extracted; (e) the research was duplicated.
Outcome measures
Given that influential subsequent clinical management decisions are based on mortality outcome, in-hospital mortality was chosen as the primary outcome of this meta-analysis. Secondary outcomes included: clinical improvement (within 36 h, was a composite outcome which required several all of the following to be fulfilled: decrease in hematocrit, Blood urea nitrogen (BUN), and creatinine from baseline, decrease in epigastric pain level, and tolerance of oral nutrition), 25 pancreatic necrosis, persistent systemic inflammatory response syndrome (SIRS), infection, organ failure, renal failure, respiratory failure, shock, and length of stay. All these outcomes were determined according to the definitions of each study, and had occurred within the first 24 h.
Data extraction and quality assessment
Two authors independently performed data extraction of all eligible studies, and the final results were reviewed and confirmed by a third adjudicative senior author. The following information was collected: (1) research characteristics (author, year of publication, and country); (2) the characteristics of patients (quantity of patients, age, etiology, and severity of the disease); (3) fluid therapy (fluid type, fluid rate, and FV); (4) the information of patients’ outcome (aggressive versus nonaggressive). The extraction of information was repeated if two authors were unable to achieve consensus.
Since the eligible studies included RCTs and observational studies, we used two tools to assess the potential risk of bias. The Cochrane Collaborative Risk of Bias Assessment Tool was used to assess potential risk of bias in RCTs. The risk was divided into three levels: high risk, low risk, and unclear risk. 27 The Newcastle-Ottawa Scale (NOS) was used to evaluate the methodological quality of the observational studies. Low-quality studies were defined as 0–3 scores, while 7–9 scores were defined as of high quality. 28
Statistical analysis
Statistical analysis was performed by using the Revman version 5.3 (The Cochrane Collaboration, Copenhagen, Denmark). For dichotomous variables, relative risks (RR) with 95% confidence intervals (CIs) were calculated. As for continuous variables, weighted mean difference (WMD) with 95% CIs were calculated. Heterogeneity across studies was measured by Q and I2 statistics. Studies with an I2 statistics of 0, 25, 50, and 75% corresponded to no, low, moderate, and high heterogeneity. Considering potential and unavoidable heterogeneity among included studies, a random effects model was adopted for all analyses in this study to improve the reliability of the results. Sensitivity analysis and subgroup analysis were performed to explore the sources of heterogeneity. Funnel plot was employed to assess publication bias. The outcome was considered to be statistically significant when p < 0.05. All statistical analyses were performed twice.
Result
Study selection
A total of 5785 records were initially searched from the four public databases. After removing duplicate records and preliminary screening, 49 full-text articles were assessed for eligibility. Among them, 34 studies were excluded for following reasons, such as non-original article, not comparing between aggressive and nonaggressive, not containing the mortality or noteworthy outcomes, data that were not extractable, and duplicate reports. Following the inclusion and exclusion criteria, 15 studies were eventually included to underpin this meta-analysis,15–21,23,29–33 including 7 RCTs and 8 cohort studies. The PRISMA flow chart of this meta-analysis was shown in Figure 1.

Flow diagram of selection.
Study characteristics and quality assessment
The characteristics of all the studies included in this meta-analysis were shown in Tables 1 and 2. Fifteen studies meeting the inclusion criteria, with 4072 AP patients involved in nonaggressive (n = 2419) and aggressive (n = 1653) groups, were conducted between 2009 and 2022. Six studies were conducted in Eastern countries, seven in Western countries, and two were multicentered. The smallest sample size was 40 and the largest sample size was 1097. The main etiologies of AP in the included studies were biliary diseases and alcohol, others included hypertriglyceridemia, post-ERCP, and idiopathy. Biliary disease was the main cause of AP in 11 studies, and alcohol was the main etiology in 2 studies. Severe pancreatitis was mainly reported in six studies and mild pancreatitis was mainly reported in nine studies (the severity of pancreatitis in each study was assessed by the proportion of severe pancreatitis). The results of Cochrane Collaborative Risk of Bias Assessment Tool and NOS were presented in the Supplemental Figure S1, Figure S2, and Table S2. All studies were of moderate or high quality.
Characteristics of all the studies included in the meta-analysis.

The nonaggressive group in the study were divided into moderate and conservative hydration.
Agg, aggressive; ERCP, endoscopic retrograde cholangiopancreatography; NA, not applicable; Non-Agg, nonaggressive; POS, prospective observational study; RCT, randomized controlled trial; ROS, retrospective observational study.
Characteristics of all the studies included in the meta-analysis.

The nonaggressive group in the study were divided into moderate and conservative hydration.
Agg, aggressive; FV, fluid volume; LR, Lactate Ringer’s; Non-agg, nonaggressive; NA, not applicable; NS, normal saline.
Primary outcome and subgroup analysis
In this meta-analysis, 13 studies reported the in-hospital mortality of 2054 patients in the nonaggressive group and 1546 patients in the aggressive group. Pooled results showed that patients in the nonaggressive hydration group had a lower mortality rate than those in the aggressive hydration group (RR, 0.66; 95% CI, 0.47–0.92; p = 0.02; I2 = 29%) (Figure 2).

Forest plot of meta-analysis of in-hospital mortality.
As the studies included two different types (RCT and observational study), mortality was significantly lower in the nonaggressive hydration group compared to the aggressive hydration group in the RCTs (RR, 0.39; 95% CI, 0.22–0.69; p = 0.001; I2 = 0%), while there was no difference between the two groups in observational studies (RR, 0.79; 95% CI, 0.53–1.17; p = 0.23; I2 = 31%) (Figure 3). It is worth mentioning that in studies conducted in Eastern countries, mortality was lower in patients who received nonaggressive hydration than in those who received aggressive hydration (RR, 0.63; 95% CI, 0.46–0.84; p = 0.002; I2 = 12%), whereas in studies reported in Western countries there was no significant difference between the two groups (RR, 0.94; 95% CI, 0.38–2.30; p = 0.89; I2 = 52%) (Figure 4). Subgroups analyses were performed according to the main etiology. In studies where biliary disease was the main etiology, there was no difference in mortality between groups (RR, 0.77; 95% CI, 0.45–1.30; p = 0.33; I2 = 25%). Notably, in studies with alcohol being the main etiology, mortality was lower in the group receiving nonaggressive hydration than in the aggressive hydration group, but the difference was not statistically significant and included only two studies (RR, 0.50; 95% CI, 0.23–1.07; p = 0.08; I2 = 55%) (Figure 5). Similarly, there was no significant difference in mortality between the two groups in studies with older participants (mean age > 50 years) (RR, 0.73; 95% CI, 0.45–1.20; p = 0.22; I2 = 30%). However, mortality was lower in the nonaggressive hydration group in studies with younger participants (mean age < 50 years) involved, but the results did not reach a statistically significant difference (RR, 0.58; 95% CI, 0.33–1.03; p = 0.06; I2 = 43%) (Figure 6). In addition, mortality was reduced in patients with severe pancreatitis who received nonaggressive hydration compared with the aggressive hydration group (RR, 0.65; 95% CI, 0.44–0.94; p = 0.02; I2 = 31%), whereas in patients with mild pancreatitis there was no significant difference between aggressive and nonaggressive hydration groups (RR, 0.69; 95% CI, 0.31–1.51; p = 0.35; I2 = 42%) (Figure 7).

Forest plot of meta-analysis of in-hospital mortality in the subgroup (RCT and observational study).
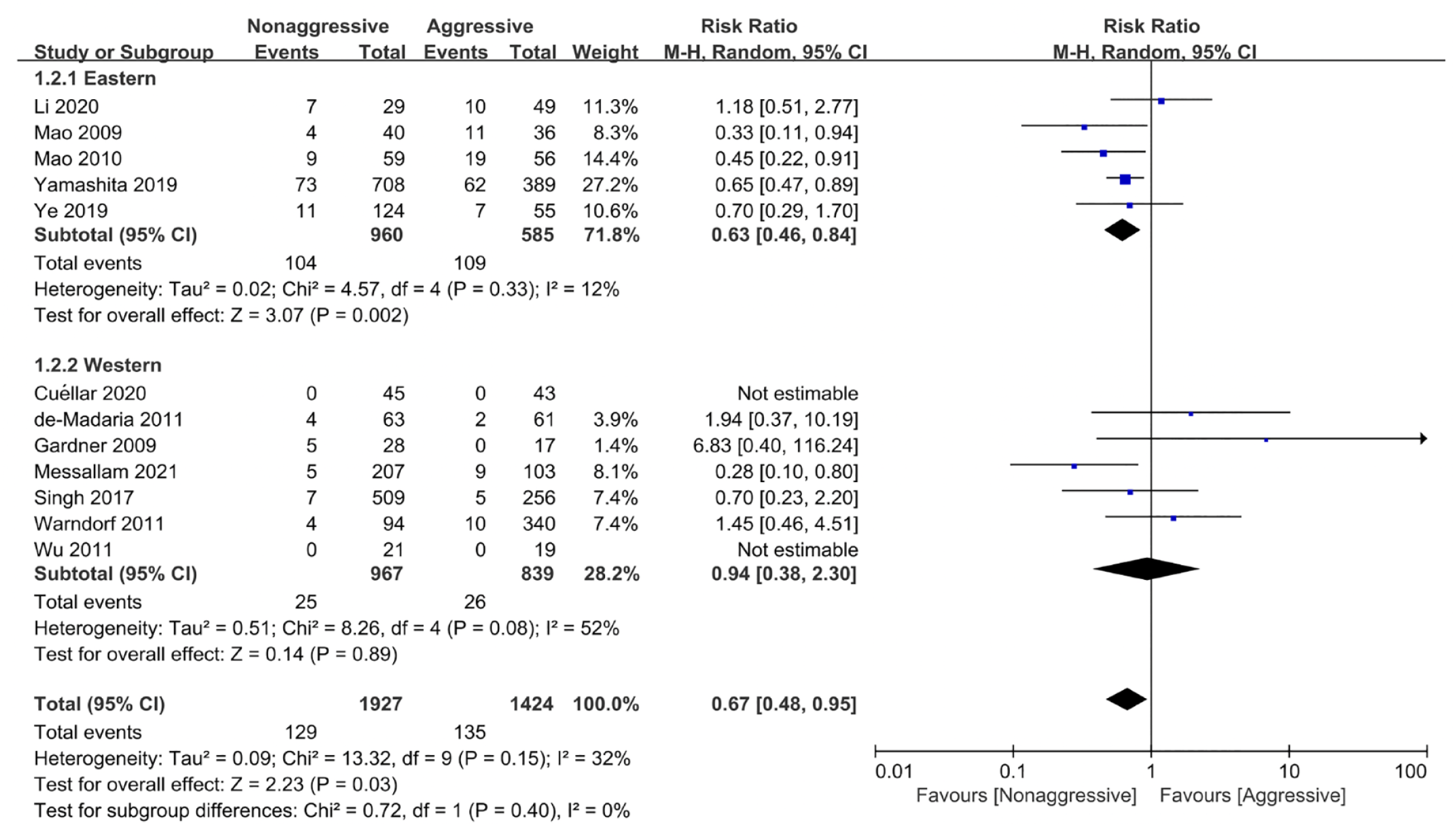
Forest plot of meta-analysis of in-hospital mortality in the subgroup (Eastern study and Western study).

Forest plot of meta-analysis of in-hospital mortality in the subgroup (studies with biliary disease as the main etiology and studies with alcohol as the main etiology).

Forest plot of meta-analysis of in-hospital mortality in the subgroup (studies in which participants were older and studies in which participants were younger).

Forest plot of meta-analysis of in-hospital mortality in the subgroup (studies with severe pancreatitis as the main and studies with mild pancreatitis as the main).
Secondary outcome
Secondary results were summarized in Table 3.
The meta-analysis of secondary outcomes compared to nonaggressive and aggressive hydration.

This data is the value of RR.
This data is the value of WMD.
CI, confidence interval; RR, risk ratio; SIRS, systemic inflammatory response syndrome; WMD, weight mean difference.
Three studies with a total of 192 patients reported clinical improvement, a composite outcome that required all following conditions to be met: a reduction in hemocytometry, BUN, and creatinine from baseline, a reduction in epigastric pain levels, and tolerance of oral nutrition. 17 These three studies were RCTs, and the results showed no statistical difference between aggressive and nonaggressive hydration groups (RR, 0.81; 95% CI, 0.50–1.33; p = 0.41; I2 = 71%).
Nine studies each reported outcomes of pancreatic necrosis (RR, 0.70; 95% CI, 0.43–1.16; p = 0.17; I2 = 90%) and persistent SIRS (RR, 0.98; 95% CI, 0.67–1.44; p = 0.92; I2 = 74%), with the pooled results showing no significant difference between the two groups. In addition, pooled data from four studies confirmed patients in the aggressive hydration group had a higher risk rate of infection than those in the nonaggressive hydration group (RR, 0.62; 95% CI, 0.49–0.80; p < 0.001; I2 = 0%).
A total of 9 studies with a total of 2357 patients reported on organ failure, and the pooled results showed that patients in the nonaggressive hydration group had a reduced risk of organ failure (RR, 0.65; 95% CI, 0.45–0.94; p = 0.02; I2 = 57%). However, seven studies each reported outcomes on renal failure (RR, 0.77; 95% CI, 0.50–1.18; p = 0.23; I2 = 46%) and respiratory failure (RR, 0.60; 95% CI, 0.30–1.17; p = 0.13; I2 = 97%), and the pooled results showed no significant difference between the two groups. Three studies reported outcomes on shock, and pooled results suggested that a higher probability of shock in aggressive hydration group compared to nonaggressive hydration group (RR, 0.21; 95% CI, 0.05–0.78; p = 0.02; I2 = 0%). Nine studies reporting the length of stay were analyzed and the pooled data showed a significant difference, with patients in the nonaggressive hydration group having shorter lengths of stay and faster recovery than those in the aggressive hydration group [WMD, −1.63; 95% CI, (−2.59)–(−0.66); p = 0.001; I2 = 92%].
Publication bias and sensitivity analysis
The funnel chart for the studies reporting mortality was roughly symmetrical and evenly distributed vertically, with 95% CI including all included trials, showing that there was no obvious publication bias among the trials (Supplemental Figure S3). Sensitivity analyses were used to assess whether individual studies affected overall results. After deleting each study individually, the analysis was relatively stable.
Discussion
Two distinct stages of AP have been identified: the early (⩽2 week) stage, characterized by systemic SIRS and/or multi-organ failure (MOF), constituting the first peak of death; and the late (>2 week) stage, characterized by local complications and, in the case of multiple complications due to co-infection of the pancreas and peripancreatic necrotic tissue co-infection; this phase constitutes the second peak of death. 34 Recognition of the critical importance of organ failure in determining disease severity is essential. Therefore, fluid therapy to prevent hypovolemia and organ hypoperfusion is the long-term cornerstone of initial AP treatment. 10 The combination of microangiopathic effects and of inflamed pancreatic edema is now believed to play a central role in the pathogenesis of AP, resulting in reduced blood flow, cellular death, necrosis, and sustained increased release of pancreatic enzymes, which activates a number of cascade responses. 35 Inflammation also increases capillary permeability, leading to increased fluid loss in the third space, exacerbating pancreatic hypoperfusion, further aggravating SIRS and leading to MOF. 36 Early aggressive IVF resuscitation can therefore provide microcirculation support, restore blood perfusion, and reduce the occurrence of serious complications such as pancreatic necrosis. 37 Clinical guidelines for fluid therapy proposed by many experts agree that intravenous volume resuscitation should be initiated as soon as the diagnosis of AP is made. 1 Ringer’s lactate, normal saline, and other crystal solutions can be the first choice for liquid therapy. 38 At present, the indicators of successful hydration have not been unified, and can be referred to the resuscitation targets of early target-oriented therapy, including urine volume >0.5 mL/kg/h, mean arterial pressure >65 mmHg, central venous pressure 8–12 cmH2O, central venous oxygen saturation ⩾70%. 34 In addition, the use of hematocrit, BUN, and creatinine is widely recommended as alternative markers.39–41
Despite early aggressive IVF resuscitation playing an important role in the treatment of AP,17,20,21 some recent studies have suggested that aggressive hydration may be associated with increased morbidity and mortality.18,23 A recent RCT conducted at 18 centers worldwide reported that early aggressive fluid resuscitation resulted in a higher incidence of fluid overload (requiring the meeting of at least two of the following three criteria: symptoms, physical signs, and imaging evidence of hypervolemia; in addition, the acute respiratory distress syndrome had to be ruled out) compared with moderate resuscitation, but no improvement in clinical outcomes (incidence of moderately severe or severe pancreatitis). 15 Two previous meta-analyses explored the effect of early aggressive hydration. One meta-analysis reported that early aggressive IVF therapy did not improve mortality and may potentially increase the risk of acute kidney injury (AKI) and pulmonary edema. 42 Another meta-analysis showed that, compared to conservative hydration, aggressive hydration increased in-hospital mortality and the incidence of pancreatic necrosis and renal failure. 43 The lack of evidences for the efficacy of aggressive fluid resuscitation has practical implications because it challenges the strong predilection of many clinicians for early high-volume hydration. These findings require us to revisit the effects of early aggressive hydration in patients with AP.
Our study found no overall benefit from early aggressive hydration compared to nonaggressive hydration and was associated with an increased risk of death during hospitalization. Overly aggressive fluid therapy may be associated with the harms in AP. A recent study suggested that fluid overload and positive cumulative fluid balance in critically ill patients might be associated with mortality. In particular, it is associated with mortality in patients with AKI, sepsis, respiratory failure, and post-operatively. 44 In summary, compared to nonaggressive hydration, the increased mortality in aggressive hydration group may be potentially related to the mechanism described above.
In order to explore the influence of different factors on the results, further subgroup analyses were conducted. In RCTs, nonaggressive hydration reduced mortality in AP patients compared to aggressive hydration, a trend not observed in cohort studies. The total available sample size of RCTs was small, so the difference may have been affected by random error. We speculate that clinicians may be more willing to use more aggressive rehydration regimens in patients with AP who are more severely ill and at higher risk of death. This may also have interfered with the overall mortality outcome in the aggressive hydration group. This speculation is contrary to our results, but the exact reasons for this remain unclear. Our results show that aggressive hydration may be associated with increased mortality in Eastern studies, whereas this difference does not appear to exist in Western studies. Some included studies did not report the exact fluid rate, only used the total volume of fluid to distinguish between aggressive and nonaggressive hydration groups. In fact, Eastern people, who being physically smaller than Westerners, may be more susceptible to aggressive hydration, leading to a positive cumulative fluid balance and thus increased mortality. 45 Cholelithiasis remains a leading cause of AP in developing countries, while in some developed countries it is more the case of excessive alcohol consumption and hypertriglyceridemia. 3 Hypertriglyceridemia and alcoholic AP are more common in young men, while biliary AP is more common in older patients. 34 Our results revealed that an aggressive fluid therapy appears to be associated with increased mortality in alcoholic, younger AP patients, but the results are not statistically different and the number of studies was relatively small. There was no difference between aggressive and nonaggressive hydration groups in the elderly patients and patients with biliary disease.
A subgroup analysis of mortality in mild AP and severe AP was performed according to the severity of the disease. Our results suggested that treatment in the aggressive hydration group is less favorable than in the nonaggressive hydration group in patients with severe pancreatitis. According to Atlanta revision (2013), severe pancreatitis is defined by the presence of persistent (fails to resolve within 48 h) organ failure. 5 Our results show that aggressive hydration is associated with an increased risk of both organ failure and infection, which is the primary cause of death in patients with severe pancreatitis. Pancreatitis is associated with increased intraabdominal pressure, which may be aggravated by excessive IVFs, thus exacerbating the symptoms of bloating in patients with severe pancreatitis. 44 This adverse effect of aggressive hydration may explain the trend toward higher symptom intensity. 15 In contrast, in mild pancreatitis, patients are better off, have no organ failure at the initial stage, and tolerate fluid overload from aggressive hydration. Therefore, there was no significant difference in mortality in patients with mild pancreatitis compared to nonaggressive hydration.
According to the analysis of the data collected so far, the therapeutic effect and prognosis of AP patients with nonaggressive liquid therapy is generally better than that of aggressive liquid therapy, so we must be extremely careful when choosing early aggressive hydration. It is important to recognize that early aggressive hydration needs to be used with greater caution in certain patient groups, such as the elderly or those with a history of cardiac or renal disease, to avoid complications such as fluid overload, pulmonary edema, and peritoneal compartment syndrome. 46 In this setting, measurement of central venous pressure through a centrally placed catheter is most often used to determine volume status. 37 Therefore, the rate and volume of fluid resuscitation should follow the principles of ‘individuality and precision’.
The American College of Gastroenterology guidelines recommend aggressive fluid resuscitation defined as 250–500 mL/h for all patients unless cardiovascular or renal comorbidities exist. According to the published studies, 37 most studies took an aggressive rehydration rate of 3 mL/kg/h and a nonaggressive rehydration rate of 1.5 mL/kg/h, so after combining the results of this study, we recommend 1.5 mL/kg/h, and the specific rehydration rate needs to be determined according to the individual patient. For the interval between onset of pancreatitis and initiation of fluid therapy, guidelines also state that early aggressive intravenous hydration is most beneficial during the first 12–24 h, beyond which there may be little benefit. 37 Many of the included studies reported that the included patients were patients with pancreatitis onset of less than 24 h,14,15,22,23,29,31 so the results of this study are generally applicable to AP patients with a delay of no more than 24 h.
Admittedly, there are still some limitations to this study: (a) Several observational studies were included in the study, which led to a decrease in the credibility of the sample. (b) This meta-analysis was unable to address the issue of reverse causality bias. Clinically, the FV of infusion varies according to the severity of the pancreatitis. Patients with severe pancreatitis have a higher chance of receiving more fluid, which contributes to the skewed outcomes. (c) There was no uniformity in the types of fluids included in the studies, and no further analysis of the functional differences between each component. (d) There is no uniform criteria for defining nonaggressive and aggressive hydration. Some literatures use the fluid volume within the first 24 h as a cut-off, while some literatures are based on fluid rate. Therefore, there are differences among literatures, which may reduce the validity of this systematic review.
Nevertheless, there are many strengths to our study. A total of 15 studies, including 4072 patients, were included in our meta-analysis, making it the largest meta-analysis on this issue in history. Meanwhile, multiple factors such as study type, region, etiology, age, and severity of disease were also analyzed. There was low to moderate heterogeneity between studies and no publication bias was shown. This study is the first to find that nonaggressive fluid resuscitation is particularly beneficial in oriental patients and in patients with severe pancreatitis, which provides some guidance for clinical practice.
In conclusion, this meta-analysis suggests that early nonaggressive fluid resuscitation is associated with lower in-hospital mortality, lower risk of organ failure and infection, and shorter length of stay than aggressive fluid resuscitation. Nonaggressive hydration therapy is particularly advantageous in oriental patients and in patients with severe pancreatitis. In alcoholic pancreatitis and younger patients, there may be advantages to nonaggressive fluid resuscitation, but the current evidence is insufficient to fully support this contention. Therefore, the choice of early aggressive fluid resuscitation must be made very cautiously, and more importantly, with appropriate information regarding the individual patient. However, due to existing limitations, more well-designed and large-sample size trials are needed to confirm our findings.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231192144 – Supplemental material for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848231192144 for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis by Jian Guo, Jiaze Hong, Yujing He, Qingyuan Li, Tongmin Huang, Dandi Lou and Jie Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848231192144 – Supplemental material for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis
Supplemental material, sj-docx-2-tag-10.1177_17562848231192144 for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis by Jian Guo, Jiaze Hong, Yujing He, Qingyuan Li, Tongmin Huang, Dandi Lou and Jie Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-3-tag-10.1177_17562848231192144 – Supplemental material for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis
Supplemental material, sj-tif-3-tag-10.1177_17562848231192144 for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis by Jian Guo, Jiaze Hong, Yujing He, Qingyuan Li, Tongmin Huang, Dandi Lou and Jie Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-4-tag-10.1177_17562848231192144 – Supplemental material for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis
Supplemental material, sj-tif-4-tag-10.1177_17562848231192144 for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis by Jian Guo, Jiaze Hong, Yujing He, Qingyuan Li, Tongmin Huang, Dandi Lou and Jie Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tiff-5-tag-10.1177_17562848231192144 – Supplemental material for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis
Supplemental material, sj-tiff-5-tag-10.1177_17562848231192144 for Comparison of early aggressive versus nonaggressive fluid resuscitation in acute pancreatitis: a meta-analysis by Jian Guo, Jiaze Hong, Yujing He, Qingyuan Li, Tongmin Huang, Dandi Lou and Jie Zhang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.