
Abstract
Objective
Our aim was to assess the accuracy of angiopoietin-2 (Ang-2) as a prognostic marker for acute pancreatitis (AP) with organ failure (OF).
Methods
We undertook a systematic search of the PubMed, Cochrane Library, Embase, Chinese Journals Full-text, Wanfang, China Biology Medicine disc, and Weipu databases to identify eligible cohort studies on the predictive value of Ang-2 for AP with OF. The main outcome measures were sensitivity and specificity. The effects were pooled using a bivariate mixed-effects model.
Results
Six articles with seven case-control studies (n = 650) were included. Pooled sensitivity, specificity, and positive and negative likelihood ratios with 95% confidence intervals (CI) for AP with OF were 0.93 (95%CI: 0.75–0.99), 0.85 (95%CI: 0.75–0.92), 6.40 (95%CI: 3.36–12.19), and 0.08 (95%CI: 0.02–0.36), respectively. The area under the summary receiver operating characteristic curve was 0.95 (95%CI: 0.92–0.96), and the diagnostic odds ratio was 83.18 (95%CI: 11.50–623.17). Subgroup analysis showed that admission time of AP onset (< or ≥24 hours) was a source of overall heterogeneity. Sensitivity analysis supported this finding.
Conclusion
Ang-2 had high diagnostic accuracy for AP with OF; the best prediction of Ang-2 may be 24 to 72 hours after onset of AP.
Introduction
Acute pancreatitis (AP), an inflammatory disorder of the pancreas, is one of the most common reasons for hospitalization related to gastrointestinal disease in China and other countries.1,2 The annual incidence of AP ranges from 13 to 45 per 100,000 people, with an increasing trend.3–5 The total mortality rate of AP is 5% to 10%.4–6 The most serious systematic complication of AP is organ failure (OF), including mainly respiratory, circulatory, and renal failure, which are the main causes of death in severe acute pancreatitis (SAP).6,7 Studies have shown that early assessment of OF in AP and adequate treatment are of the utmost importance in reducing the morbidity and mortality associated with AP.8–10
Several scoring systems have been developed to detect severity of AP. These scoring systems include the Ranson criteria, Balthazar score, Acute Physiology and Chronic Health Evaluation II (APACHE II), and Bedside Index of Severity in AP (BISAP).11,12 Recent studies have identified numerous biomarkers that can be used to assess the severity of AP, including interleukin-6 and interleukin-8, D-dimer, and procalcitonin (PCT).11–13 Nevertheless, the low accuracy, tedious laboratory procedures, cost, and lag in detection associated with these biomarkers currently restrict their clinical use. 11 In addition, the sole use of computed tomography (CT) to evaluate the severity of AP is not recommended when a patient is admitted to the hospital, and the cost of radiological tests is high. 14 Therefore, a new biomarker is needed for better prediction of the severity of AP.
Angiopoietin-2 (Ang-2) belongs to a novel class of endothelial growth factors; it is a type of glycoprotein that acts selectively on endothelial cells and is packaged in secretory Weibel-Palade bodies. It is discharged from endothelial cells in response to hypoxia, inflammation, or mechanical injury.15,16 Ang-2 participates in priming the endothelium to respond to angiogenetic and inflammatory cytokines by binding to the same site of the Tie-2 receptor as Ang-1, which leads to instability of endothelial cells and vascular degeneration, causing a vascular leakage syndrome that results in hemoconcentration, hypotension, pulmonary edema, and renal insufficiency among patients with acute conditions, including AP.16–18 Recently, studies have identified Ang-2 as a promising biomarker to predict the complications that accompany AP, especially OF.17,18 However, owing to the lack of multi-center clinical studies with large sample sizes, Ang-2 is not widely used. To investigate the accuracy of Ang-2 in diagnosis of AP with OF, we reviewed related studies and determined the utility of Ang-2 in the diagnosis of AP with OF.
Methods
Ethics statement
Ethical review for this study was deemed unnecessary because the data were derived from existing databases.
Literature search
A systematic search was undertaken using the Cochrane Library, PubMed, Embase, Chinese Journals Full-text, Wanfang, China Biology Medicine disc, and Weipu databases for articles to assess the diagnostic value of Ang-2 for OF among patients with AP. The time span of the search was from the initiation of these databases to 2 April 2020. The search was conducted using the search terms “pancreatitis” OR “acute pancreatitis” OR “pancreatic inflammation” OR “pancreas inflammatory” AND “angiopoietin-2”. We also scanned reference lists from original articles and reviews to identify additional articles. The meta-analysis was performed and reported in accordance with the guidelines for reporting systematic reviews related to diagnostic accuracy and following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Study identification
Studies were included in this meta-analysis when they met the following criteria: (1) design—prospective and retrospective cohort studies; (2) population—adult patients (>18 years) with AP; (3) exposure—studies must provide Ang-2 value for both sensitivity and specificity of the diagnosis for AP with OF; (4) outcome—AP with OF (as defined by the authors of primary studies). Studies meeting the following criteria were excluded: guidelines, animal studies, comments, editorials, mechanistic studies, case reports, and review articles.
Data extraction
Data extraction was independently completed by two reviewers (Jingjing Lei and Yongcai Lv). In case of disagreement, a third co-author (Qi Liu) acted as ombudsman. The following data were taken from the primary study: the first author’s name, publication year, study country, study design, sample size, the number of patients developing OF, age, sex (proportion male), etiology, admission time of AP onset, Ang-2 sampling time of admission, Ang-2 assay, diagnostic definition of AP, diagnostic definition of OF, and rates of true positive, false positive, false negative, and true negative results. (Tables 1 and 2).
Characteristics of studies included in the meta-analysis.

Ang-2, angiopoietin-2; OF, organ failure; AP, acute pancreatitis; SD, standard deviation; MAP, mild acute pancreatitis; MSAP, moderately severe acute pancreatitis; SAP, severe acute pancreatitis; ELISA, enzyme-linked immunosorbent assay; —, not reported.
Diagnostic definitions and parameters for acute pancreatitis and organ failure used in the 7 studies.

OF, organ failure; AP, acute pancreatitis; SBP, systolic blood pressure; PO2, partial pressure of oxygen; Cr, creatinine; TP, true positive; FP, false positive; TN, true negative; FN, false negative; —, not reported.
Quality assessment
The methodological quality of the included studies was evaluated by Yanhua Yao and Yongcai Lv using the quality assessment of diagnostic accuracy studies questionnaire (QUADAS), and quality was determined according to the 14 items in Table 3. 19 If there were discrepancies between reviewers, a third investigator (Jingjing Lei) was consulted.
Quality assessment of included studies using the quality assessment of diagnostic accuracy studies questionnaire (QUADAS).
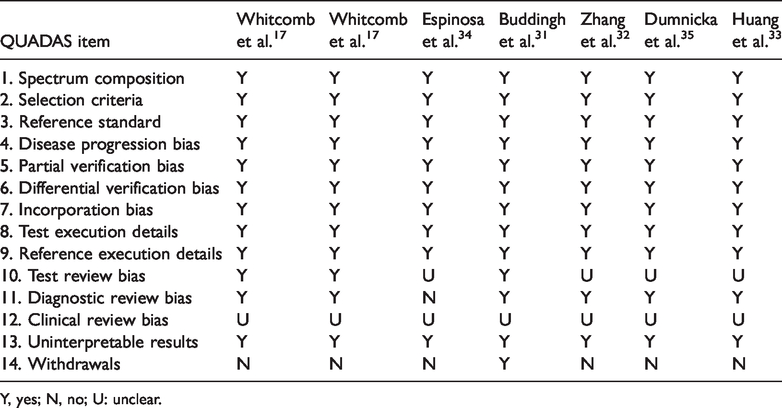
Y, yes; N, no; U: unclear.
Statistical analysis
We used Stata version 15.0 (Stata Corp., College Station, TX, USA) for this meta-analysis. The pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR) were calculated using the bivariate mixed-effects model. Detecting the source of threshold heterogeneity is a key step in diagnostic meta-analysis, and the discussion of heterogeneity includes threshold and non-threshold effects. To evaluate the threshold effect, the Spearman correlation coefficient (r) between logarithm of sensitivity and that of (1 − specificity) was calculated, and a threshold effect considered when r > 0.6 and p < 0.05. A summary receiver operating characteristic (sROC) curve was plotted, which was also used to check threshold effect and diagnostic accuracy. The threshold effect is considered to be absent when the sROC curve does not have a “shoulder-arm” distribution. Heterogeneity was evaluated by I2 value, and significant heterogeneity was considered when I2 >50%. Subgroup analysis was performed to assess the sources of heterogeneity, and sensitivity analysis was used to evaluate the stability of the results. The clinical applicability of Ang-2 was evaluated by Fagan nomogram, and publication bias was assessed using Deeks’ funnel plot.
Results
Characteristics and quality of included studies
A total of 196 articles were retrieved in this study (Figure 1). Eighteen articles were considered relevant and reviewed. Subsequently, 12 of the 18 studies were removed for the following reasons: 2 were review articles,20,21 1 was a letter, 22 6 had inconsistent observation indices,23–28 2 were based on the same populations,18,29 and the data of 1 could not be extracted. 30 In one of the remaining six articles, Whitcomb et al. 17 independently reported results of two parts of the study population, which we therefore considered as two studies in our analysis. Therefore, six original reports consisting of seven case-control studies were included in our meta-analysis.17,31–35 Of these, four studies were carried out in the United States and Europe and two studies were carried out in Asia. The included studies were published from 2010 to 2020.
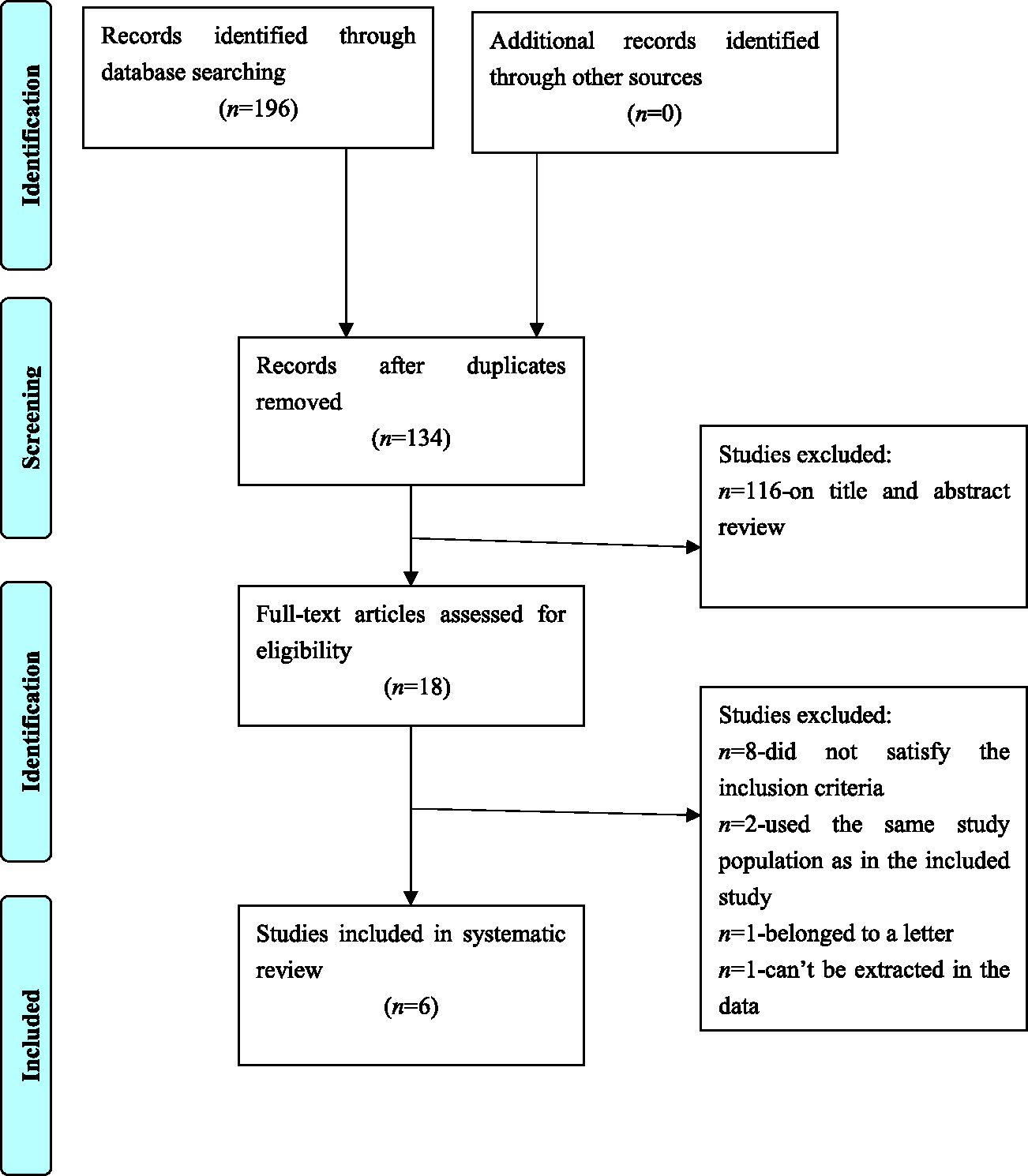
PRISMA flow diagram of the study selection process.
Quality assessment
Assessment of methodological quality showed that items 1, 2, 3, 4, 5, 6, 7, 8, 9, and 13 had the response “yes” in all studies; items 10, 11, 12, and 14 had responses of “no” or “unclear.” The overall quality of the seven studies was good. The results are shown in Table 3.
Meta-analysis results
Testing for heterogeneity
The Spearman correlation coefficient (r) for heterogeneity was −0.464 (P = 0.294), and the sROC curve did not show a “shoulder-arm” distribution, indicating that the heterogeneity of this meta-analysis could not be explained by a threshold effect. The I2 and P-values of the pooled sensitivity and specificity were 72.67% (P < 0.01) and 91.65% (P < 0.01), respectively, indicating significant heterogeneity among the included studies (Figure 2). Therefore, meta-regression and subgroup analysis were needed to find the source of heterogeneity.

Diagnostic accuracy
The pooled sensitivity, specificity, PLR, and NLR of Ang-2 to predict AP with OF were 0.93 (95%CI: 0.75–0.99), 0.85 (95%CI: 0.75–0.92), 6.40 (95%CI: 3.36–12.19), and 0.08 (95%CI: 0.02–0.36), respectively. The area under the sROC curve (AUC) for OF was 0.95 (95%CI: 0.92–0.96), with a DOR of 83.18 (95%CI: 11.50–623.17); these results indicated high overall accuracy of Ang-2 for predicting AP with OF (Figures 2 and 3).

Summary receiver operating characteristic (sROC) curve of Ang-2 for diagnosis of AP with OF..
Subgroup analysis
Sources of overall heterogeneity included sample size (≥100 or <100), study design (prospective or retrospective), geographical location (Asia vs. Europe or United States), definition of OF (Atlanta classification or others), Ang-2 sampling time relative to admission (≥24 hours or <24 hours), and admission time of AP onset (≥24 hours or <24 hours), and the above factors were predefined in our meta-analysis. The subgroup analysis showed sensitivities of studies to Ang-2 sampling time of admission and definition of OF, and specificities of studies for sample size, but only admission time of AP onset was a source of overall heterogeneity (P < 0.05) (Figure 4, Table 4).
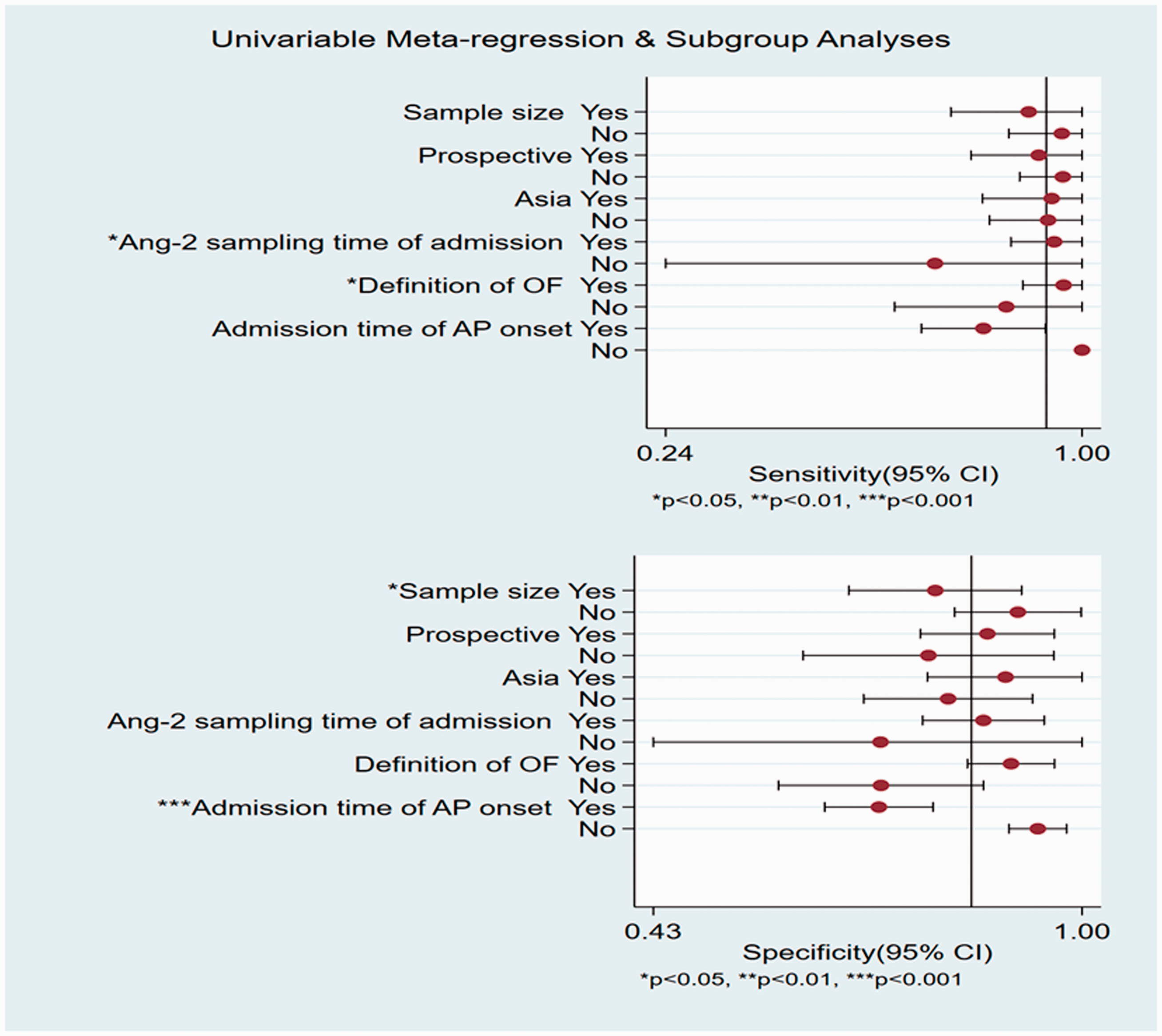
Subgroup analysis of potential heterogeneity within the included studies. Meta-regression analysis for Ang-2 with following variables: sample size ≥100 or not; prospective or not; Ang-2 assay with Asia or not; definition of OF (Atlanta classification or not); Ang-2 sampling time of admission ≥24 hours or not; admission time of AP onset? 24 hours or not; where yes =1, not = 0.
Subgroup analysis of potential heterogeneity within the included studies.

AP, acute pancreatitis; Ang-2, angiopoietin-2; OF, organ failure; P1, P-value for heterogeneity of sensitivity; P2, P-value for heterogeneity of specificity; P-value, P-value for overall heterogeneity in the subgroup.
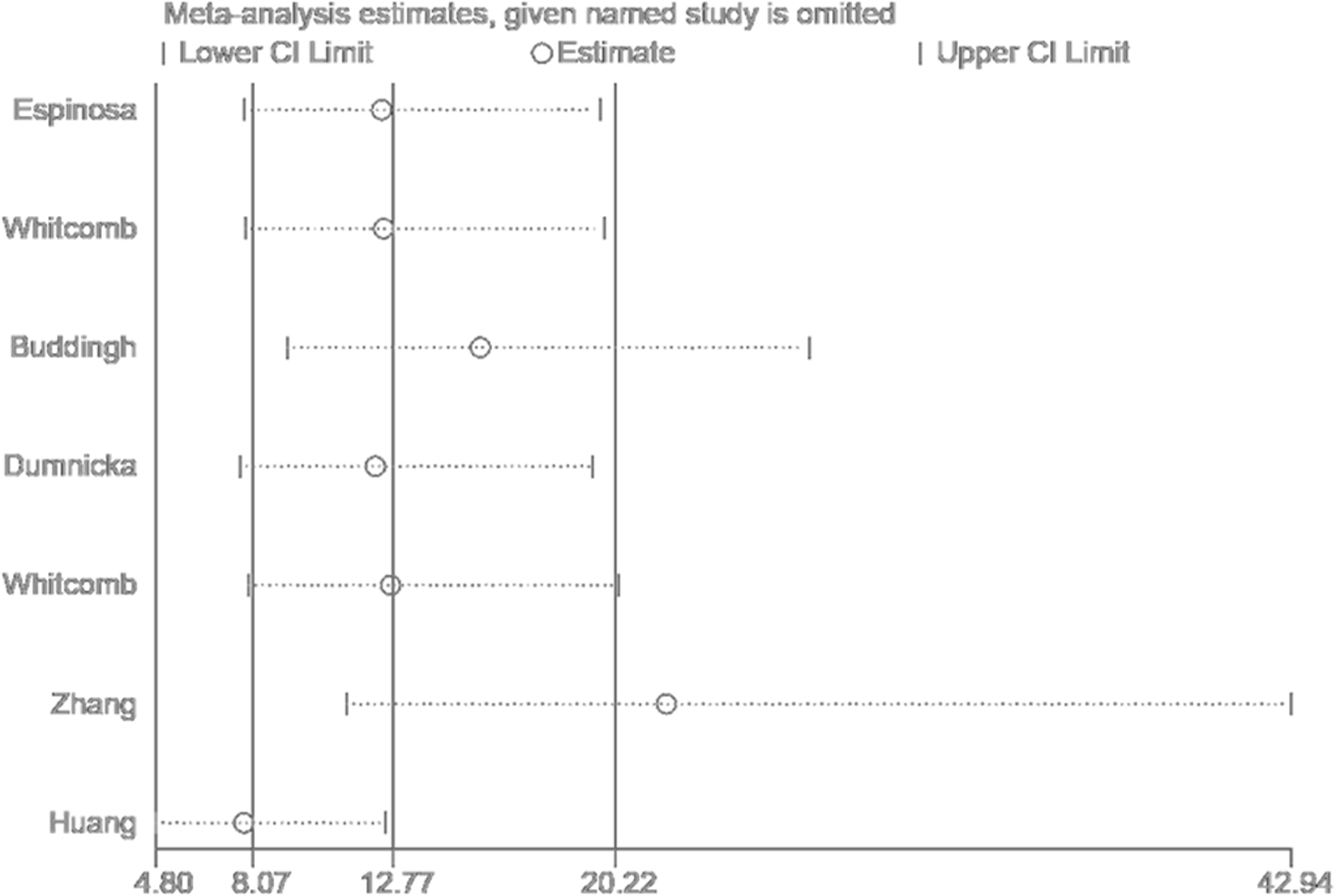
Sensitivity analysis
Sensitivity analysis was conducted to ensure that the overall results were not affected by individual studies and to assess whether the pooled effect was stable. Our analysis indicated that the best prediction of Ang-2 occurred between 24 and 72 hours after the onset of AP, which further confirmed the results of the subgroup analysis (Figure 5).
Evaluation of Ang-2 applicability
According to the results of the Fagan nomogram, with a pretest probability of 20% and Ang-2 being positive, the probability of a patient with AP being diagnosed with OF increased to 62%. If Ang-2 was negative, the probability of a patient being diagnosed with OF decreased to 2%, indicating that the early Ang-2 assay had good applicability (Figure 6).

Fagan’s nomogram of the Ang-2 test for diagnosis of AP with OF.
Publication bias assessment
Deeks’ funnel plot was used to evaluate publication bias. We found no evidence of publication bias in the included studies (Figure 7).

Deeks’ funnel plot for the assessment of potential publication bias of the included studies
Discussion
In recent years, many studies have assessed the diagnostic utility of Ang-2 in the severity of AP.17,31,32 As a biomarker, it is better than traditional predictors that are currently used in the clinical setting, such as C-reactive protein (CRP), PCT, APACHE II score, or the Ranson criteria17,31–35 (Table 5). Levels of CRP, PCT, and neutrophil gelatinase-associated lipocalin and APACHE II score have been positively correlated with Ang-2 in patients with AP.18,32 Watanabe et al. 26 revealed that serum Ang-2 was negatively correlated (ρ = −0.68, P = 0.03) with τ-values (the average time from abdominal aorta to pancreatic tissue; its value is negatively correlated with hyperdynamic state of systemic circulation) of perfusion CT parameter. Taken together, these findings indicate that a serum Ang-2 level at admission could be a useful predictor for the severity of AP. The current meta-analysis is the first to assess the diagnostic accuracy of Ang-2 for AP with OF. Six articles (7 case-control studies) met the inclusion criteria and included 650 patients. The methodological quality of the included studies was systematically reviewed using the QUADAS tool and showed that the basic characteristics of the patients were relatively consistent, which could meet the requirements of QUADAS scale for literature evaluation. Detailed information of the QUADAS criteria indicated that future clinical studies should pay attention to several aspects, including test review bias, diagnostic review bias, clinical review bias, and withdrawals.
Angiopoietin-2 compared with other more commonly used predictors in acute pancreatitis with organ failure.
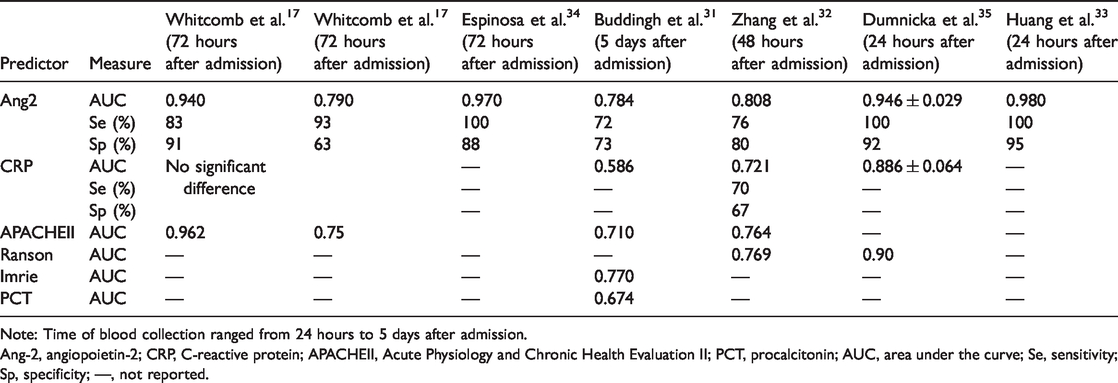
Note: Time of blood collection ranged from 24 hours to 5 days after admission.
Ang-2, angiopoietin-2; CRP, C-reactive protein; APACHEII, Acute Physiology and Chronic Health Evaluation II; PCT, procalcitonin; AUC, area under the curve; Se, sensitivity; Sp, specificity; —, not reported.
Sensitivity and specificity values provide false negative and false positive rates, helping clinicians to screen for or diagnose diseases. 36 Data from the studies included in our meta-analysis demonstrated that the serum Ang-2 assay had a relatively high sensitivity (0.93) and specificity (0.85), resulting in a false negative rate of 7% and false positive rate of 15%. Therefore, Ang-2 can only be used as a screening tool; it cannot be used, as yet, in the diagnosis of AP with OF.
The AUC of the sROC indicate the overall diagnostic value of a biomarker, and DOR indicates testing performance.37,38 Therefore, the potential diagnostic accuracy of Ang-2 for AP with OF can be calculated by AUC and DOR. In this meta-analysis, DOR and AUC were 83.18 and 0.95, respectively, showing a high overall accuracy for predicting AP with OF.
According to the results of this meta-analysis, the PLR of 6.40 implied that a patient with OF in AP was 6.4 times more likely to have a positive test than a negative test, and the Fagan nomogram with a pretest probability of 20% showed that the probability of being diagnosed of AP with OF, following a positive Ang-2 test, increased to 62%. The NLR of 0.08 indicated that the probability of AP with OF in patients with a negative Ang-2 test decreased to 2% in the Fagan nomogram. These results suggested that Ang-2 had good applicability as a marker of OF in patients with AP.
Detecting the source of threshold heterogeneity is a key step in a diagnostic meta-analysis, and the only homogeneous studies can be merged. 38 To detect heterogeneity, we carried out the I2 test on the pooled specificity and sensitivity. The heterogeneity of the six studies was obvious, but the Spearman correlation coefficient was not significant (r = −0.464, P = 0.294) and the sROC did not show a “shoulder-arm” distribution, implying that the threshold effect was not the source of heterogeneity. Therefore, we used a subgroup analysis to examine other potential sources of heterogeneity, including sample size, study design, geographical location, definition of OF, Ang-2 sampling time of admission, and admission time relative to AP onset. The subgroup analysis showed that admission time relative to AP onset was the source of heterogeneity. The sensitivity analysis indicated that the best prediction by Ang-2 might occur between 24 and 72 hours after the onset of AP, which further confirmed the subgroup analysis. However, the subgroup analysis demonstrated that other factors had some effect on sensitivity or specificity, including sampling time after admission, definition of OF, and sample size. Therefore, future studies that assess the use of Ang-2 in AP should pay attention to these aspects.
Increased concentrations of Ang-2 have been shown in AP and have been closely associated with time from onset in more severe cases of AP.17,31,34 Whitcomb et al. 17 showed that Ang-2 level within 72 hours of pain onset with a cutoff value of 1.910 ng/mL resulted in AUC, sensitivity, and specificity of 0.940, 83%, and 91%, respectively, to predict OF in 28 patients with AP. However, an Ang-2 level at admission with a cutoff value of 2.396 ng/mL had AUC, sensitivity, and specificity of 0.790, 93%, and 63%, respectively, to predict OF in 123 patients with AP. The difference of diagnostic accuracy in these two populations may reflect the different time of onset of AP in addition to the fluid resuscitation protocol affecting the value of Ang-2. Unfortunately, the time of pain onset was not recorded in the cohort of 123 patients in Whitcomb et al. 17 Espinosa et al. 34 collected blood samples at 12 hours after admission, and patients were included up to 72 hours from the onset of symptoms of AP. In that study, Ang-2 was the best predictor of AP with OF among several markers of endothelial dysfunction, and the cutoff point was 10 ng/mL, with high sensitivity (100%), specificity (88%), and AUC (0.9). In contrast, Buddingh et al. 31 included patients within 72 hours of AP onset but collected samples on day 5 after admission. Although high concentrations of Ang-2 were observed in patients with clinically diagnosed OF, that study had a low AUC (0.784), with sensitivity and specificity of 72.2% and 73.2%, respectively. Therefore, it is possible that the diagnostic accuracy of Ang-2 does not extend beyond 72 hours after onset. Kolber et al. 30 stated that an elevated serum Ang-2 level was not significant (P = 0.1) in predicting severity of AP on day 1 of onset but could predict (P = 0.041) severity of AP on day 2. Dumnicka et al. 29 reported that the AUC of Ang-2 for predicting moderately severe acute pancreatitis (MSAP) and SAP was 0.719 at 24 hours from the onset of pain. Subsequently, a sub-study was carried out in 66 patients, of which 20 had MSAP+SAP; the onset to admission time of 9 patients was 18 to 21 hours, whereas that of 11 patients was 22 to 24 hours, and the AUC of MSAP+SAP of 18 to 21 hours was 0.632. Compared with that on the first day (P = 0.006), the elevated serum Ang-2 level had greater significance (P < 0.001) on day 2 after onset. These results seem to indicate that the association between Ang-2 concentration and AP with OF is stronger after 24 hours from onset of AP. More recently, Zhang et al. 32 included 120 patients with AP, collected blood samples at 48 hours, and admitted patients within 48 hours of onset. The AUC of Ang-2 for predicting OF was 0.808 when the cutoff was 3.31 ng/mL, with sensitivity and specificity of 75.68% and 79.52%, respectively. According to the sensitivity analysis, we speculate that some of the patients in the Zhang et al. 32 study may have been less than 24 hours from onset of AP.
The results from the above studies (showing that the relationship between Ang-2 concentration and AP with OF is stronger after 24 hours of AP onset) are in contrast to those of Huang et al. 33 The patients in Huang et al. 33 were all within 24 hours of onset, and blood collection for Ang-2 measurement was also within 24 hours of admission. The AUC for predicting OF was 0.980, with a cutoff value of 11.76 ng/mL, and sensitivity and specificity were 100% and 95.2%, respectively. However, these findings were based on a small, single-center study, and large, multi-center studies are needed to confirm the results. The results suggest, however, that it may be better to assess the use of Ang-2 as a predictor of OF in groups based on time of collected serum and admission time of AP onset, but this was not possible because of the lack of studies and the lack of significance after grouping.
Many studies indicated that a combination of biochemical markers may improve the diagnosis of severity of AP. We could identify only one study that reported on the combination of Ang-2 and soluble fms-like tyrosine kinase-1 (sFlt-1), although the combination did not predict MSAP+SAP better than Ang-2 alone. 29 However, because of the small sample size, this result is questionable. Among other diseases, including sepsis and severe trauma, we did not find reports combining Ang-2 with other indicators to diagnose related severe diseases, which may be a research direction to follow in the future.
We note a number of possible limitations in this meta-analysis. First, we included only published studies in English and Chinese; studies published in other languages and unpublished articles were not included. Second, our results are based only on retrospective and prospective studies, which might lead to confounding. Although in general, confounding factors are primarily solved by using randomized controlled trials, such studies are not designed to analyze the natural process of a disease. Third, varying definitions of OF were used in the included studies. We solved this problem by using predefined subgroup analyses, which demonstrated the credibility of our results despite the different definitions of OF. Moreover, persistent OF has a worse prognosis than transient OF. Unfortunately, only a few early studies included data on persistent OF, thus we could not analyze this aspect of OF. Finally, different cutoff values were used among the studies. Results were based on such differences as test-kit manufacturers, generations, and ethnicities and populations, and we could not obtain the original data from the included studies. Hence, we did not pool these cutoff values in the meta-analysis, which would have led to limited application of the results. However, we did conduct a threshold analysis in advance and found that the sensitivity and specificity of the included studies were not affected by the cutoff value used.
Conclusion
We demonstrated that Ang-2 has high diagnostic accuracy for OF in patients with AP, with pooled sensitivity and specificity values of 0.93 and 0.85, respectively. The AUC of the sROC curve was 0.95 and the DOR was 83.18. Subgroup and sensitivity analyses demonstrated that the best prediction of Ang-2 may occur between 24 and 72 hours after the onset of AP. This finding indicates that Ang-2 can be used as a predictor of the severity of AP in the future.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520986708 - Supplemental material for Accuracy of angiopoietin-2 for predicting organ failure in patients with acute pancreatitis: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_0300060520986708 for Accuracy of angiopoietin-2 for predicting organ failure in patients with acute pancreatitis: a systematic review and meta-analysis by Yongcai Lv, Yanhua Yao, Qi Liu and Jingjing Lei in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_0300060520986708 - Supplemental material for Accuracy of angiopoietin-2 for predicting organ failure in patients with acute pancreatitis: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_0300060520986708 for Accuracy of angiopoietin-2 for predicting organ failure in patients with acute pancreatitis: a systematic review and meta-analysis by Yongcai Lv, Yanhua Yao, Qi Liu and Jingjing Lei in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_0300060520986708 - Supplemental material for Accuracy of angiopoietin-2 for predicting organ failure in patients with acute pancreatitis: a systematic review and meta-analysis
Supplemental material, sj-pdf-3-imr-10.1177_0300060520986708 for Accuracy of angiopoietin-2 for predicting organ failure in patients with acute pancreatitis: a systematic review and meta-analysis by Yongcai Lv, Yanhua Yao, Qi Liu and Jingjing Lei in Journal of International Medical Research
Footnotes
Author contributions
JJL and YCL designed the study; JJL, YCL, YHY, and QL acquired, analyzed, and interpreted the data; YCL drafted the initial manuscript; JJL is the guarantor and revised the article critically for important intellectual content.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was Supported by The Science and Technology Program of Guiyang Municipal Bureau of Science and Technology (No. [2018] 1-72), and The Science and Technology Program of Guiyang Baiyun District Science and Technology Bureau (No. [2017] 50).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.