
Abstract
Background:
The high-flow nasal cannula (HFNC) is a relatively recent method that provides high-flow, heated, humidified gas delivery.
Objectives:
We compared HFNC (group HF) and conventional nasal cannula (NC) (group CO) during deep sedation with propofol and remifentanil for endoscopic submucosal dissection (ESD).
Design:
Single-center, retrospective observational cohort study.
Methods:
In this study, a total of 159 cases were analyzed (group CO, 71 and group HF, 88). We collected the data from electronic medical records from September 2020 to June 2021. The lowest oxygen saturation (SpO2), incidence of hypoxia (SpO2 < 90%), rescue interventions, and adverse events between the two groups were investigated.
Results:
There were significant differences between the two groups in lowest SpO2 and incidence of hypoxia [group CO versus group HF; 90.3 ± 9.7% versus 95.7 ± 9.0%, 25 (35.2%) versus 10 (11.4%); p < 0.001, p < 0.001; respectively]. Among the rescue interventions, the number of jaw thrust, patient stimulation, O2 flow increase, and nasal airway insertion were significantly higher in the CO group than in the HF group. However, postprocedural chest X-ray showed higher rates of abnormal findings (atelectasis, aspiration, and pneumoperitoneum) in group HF than in group CO [group CO: 8 (11.3%) versus group HF: 26 (29.5%), p = 0.005]. In multivariable analysis, besides group CO, difficult type of lesion was the risk factor for hypoxia.
Conclusions:
Compared to the conventional NC, HFNC provided adequate oxygenation and a stable procedure without significant adverse events during sedation for ESD. However, caution is needed to avoid complications associated with deep sedation and difficult type of lesions.
Introduction
Endoscopic submucosal dissection (ESD) is a widely performed less invasive treatment for early gastric cancer due to its relative safety, low risk of complications, and applicability compared with surgical resection. Deep sedation is often required for ESD. However, deep sedation carries risk of upper airway obstruction, respiratory depression, decreased chest wall compliance, and consequent hypoxia. 1 Moreover, it is difficult to supply oxygen efficiently due to the nature of the endoscopic procedure. Hypoxia is the most common adverse event during gastroscopy with sedation, and the incidence of hypoxia has been reported to range from 1.8% to 69%.2–5 In case of severe hypoxia, manual ventilation or tracheal intubation may be required as well as discontinuation of the procedure. Therefore, a method is needed to prevent hypoxia or detect it at an early stage during deep sedation.
In our center, oxygen has been provided using a nasal cannula (NC) during sedation for ESD. When hypoxia or upper airway obstruction occurs, methods such as increased oxygen, lifting the chin, and insertion of a nasal airway device have been used. There is a limit to the supply of high-flow oxygen through a NC, and it is difficult to measure reliable end-tidal CO2 values in endoscopic procedures. Due to these issues, unexpected hypoxia can occur.
The high-flow nasal cannula (HFNC) system recently has been developed. This system can provide extremely high-flow (up to 70 L/min), heated, and humidified gas with an adjustable temperature (31–37 °C) through a special NC. 6 Several studies of the HFNC have been published in patients with acute respiratory failure, and its advantages and disadvantages were discussed.7–10 Recently, the HFNC has been applied in gastrointestinal endoscopic cases.6,11,12 These studies demonstrated the superiority of HFNC in terms of oxygenation.
In this retrospective study, we compared groups with HFNC (group HF) and conventional NC (group CO) during deep sedation with propofol and remifentanil for ESD. In addition to analysis of hypoxia-related variables and adverse events, we also investigated the risk factors associated with hypoxia during sedation.
Materials and methods
Study design
This was a single-center, retrospective study for comparing variables related to hypoxia and to find risk factors associated with hypoxia during deep sedation for ESD. The study proposal and statistical plan were registered with the IRB before accessing patient data. The trial was conducted in accordance with the original protocol. We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology checklist for reporting observational studies. 13 All methods were performed in accordance with the ethical principles of the 1964 Declaration of Helsinki and its later amendments.
Patient records
We collected study data from electronic medical records at our institution consecutively from patients who underwent ESD under deep sedation performed by an anesthesiologist between September 2020 and June 2021 (n = 159). The primary objective was to compare the lowest oxygen saturation (SpO2) value during sedation between HFNC (group HF) and conventional NC (group CO) groups.
The following information was collected from electronic medical records: baseline characteristics of age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, snoring mentioned by family, obstructive sleep apnea (OSA), smoking, previous pulmonary diseases, type (A, B, or C) of lesion, and baseline SpO2.
Intraprocedural data were collected including the SpO2 values (lowest and mean during the procedure), incidence of hypoxia (SpO2 < 90%) and mild hypoxia (90 ⩽ SpO2 < 95%), percutaneous CO2 (PtCO2) value at the end of the procedure, incidence of hypercapnia (PtCO2 > 60 mmHg), and rescue maneuvers during sedation (patient stimulation, drug adjustment, jaw thrust, oxygen flow increase, nasal airway insertion, and mask ventilation and/or intubation including laryngeal mask airway).
Postprocedural data were procedure time, total drug doses (midazolam, propofol, and remifentanil), discharge with oxygen supply, hospital stay, chest X-ray, and complications.
Sedation procedure
Upon arrival in the endoscopy room, patients were monitored for pulse oximetry, noninvasive blood pressure, and electrocardiography and moved to the left lateral decubitus position. CO2 was measured percutaneously (PtCO2) in the patient’s earlobe (Sentec®, SenTec AG, Therwil, Switzerland). In the conventional NC (group CO) group, 100% oxygen was administered at 6 L/min via a NC throughout the procedure. In the HFNC (group HF) group, 100% oxygen was administered at 30 L/min via an HFNC system (OptiFlow THRIVE, Fisher and Paykel Healthcare, Panmure, Auckland, New Zealand) throughout the procedure. Since only one of the two endoscopy rooms has an HFNC device, the associated group was randomly determined. A bolus of 1–1.5 mg midazolam was delivered followed by continuous infusion of propofol and remifentanil using a target-controlled infusion pump. The targeted level of sedation was equivalent to the Modified Observer’s Assessment of Awareness and Sedation score less than 3 in all patients. If sedation or analgesia was insufficient, a midazolam of 0.5 mg was additionally administered, or propofol/remifentanil concentration was adjusted. Any interventions including drug adjustment, patient stimulation, oxygen flow increase, jaw thrust, nasal airway insertion, or conversion to manual/mechanical ventilation were performed at the anesthesiologist’s discretion based on the presence of desaturation or apnea.
ESD procedure and postprocedural process
The type of lesion was previously determined as A, B, and C in the order of difficulty according to location, size, and degree of fibrosis through gastroscopy prior to ESD. Five gastroenterologists performed all gastric ESD procedures using standard techniques. First, a circumferential mark was made around the lesion using a needle knife or a dual knife. Thereafter, fluid [normal saline (100 mL), epinephrine (1 mL), and 0.8% indigo carmine (0.1 mL)] was injected into the submucosal layer. A circumferential mucosal precut was made, and the submucosal layer was dissected using various types of knives. Endoscopic hemostasis was performed simultaneously whenever bleeding was observed.
After the procedure, patients were moved to a recovery room and monitored for vital signs and adverse events. After staying in the recovery room for about 30 min, the patients underwent chest X-ray examination to identify complications such as pneumoperitoneum. Postprocedural atelectasis or aspiration was diagnosed by radiological examination after ESD. To identify them, the chest radiographs before and after ESD were reviewed by two radiologists who were blinded to the endoscopic procedure. After examination of their chest radiographs, patients were discharged to the ward.
Primary end point: Lowest SpO2
The lowest oxygen saturation measured via pulse oximetry during the procedure was recorded. When the oxygen saturation was continuously changed, the value maintained for more than 10 s was recorded.
Statistical analysis
Independent t-test or the Wilcoxon rank-sum test was used to determine significant differences in continuous variables. The chi-square test or Fisher’s exact test was used to compare categorical variables. Patient demographic and clinical data were summarized as a frequency (percentage) for categorical variables and mean (standard deviation) for continuous variables. The normality of the continuous variable was evaluated using the Shapiro–Wilk test.
Logistic regression was used to assess protective factors for hypoxia. Variables with p < 0.2 in the univariable analysis were included in the multivariable analysis. 14
The reported p values were two-tailed, and p < 0.05 was considered statistically significant. All statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA).
Results
Characteristics of patients and procedure
The analysis cohort comprised all 159 patients who underwent ESD between September 2020 and June 2021 at a single institution. Baseline patient and procedure characteristics compared between the CO (n = 71) and the HF (n = 88) groups are shown in Table 1. Patients with OSA who were using positive pressure devices were indicated. The duration of the ESD procedure and drug dosages were not significantly different between the two groups.
Baseline characteristics of the study population.

The qualitative data are presented as no. (%), and the numerical data are presented as the mean (SD).
There were no significant differences between the two groups in any of the characteristics listed.
ASA-PS, American Society of Anesthesiologists physical status classification; BMI, body mass index; OSA, obstructive sleep apnea.
Outcome data including SpO2, PtCO2, and rescue interventions around the procedure are shown in Table 2. There was no difference in baseline SpO2 before preoxygenation between the two groups [97.8% (1.4) versus 97.8% (1.3); p = 0.948]. However, the lowest mean (SD) SpO2 during the procedure was different between the CO group and the HF group [90.3% (9.7) versus 95.7% (9.0), respectively; p < 0.001]. The incidence of hypoxia and also mild hypoxia was more frequent in group CO than in group HF [25 (35.2%) versus 10 (11.4%); p < 0.001, 21 (29.6%) versus 8 (9.1%); p < 0.001; respectively]. PtCO2 at the end of the procedure and the incidence of hypercapnia (PtCO2 >60 mmHg) were comparable between the two groups [56.1 (9.8) mmHg versus 57.1 (10.7) mmHg; p = 0.614, 21 (38.9%) versus 32 (52.5%); p = 0.145; respectively]. Interventions for hypoxia or apnea (rescue maneuvers) including patient stimulation, jaw thrust, oxygen flow increase, and nasal airway insertion were significantly higher in group CO than in group HF (Table 2).
Clinical data and rescue interventions during the procedure.
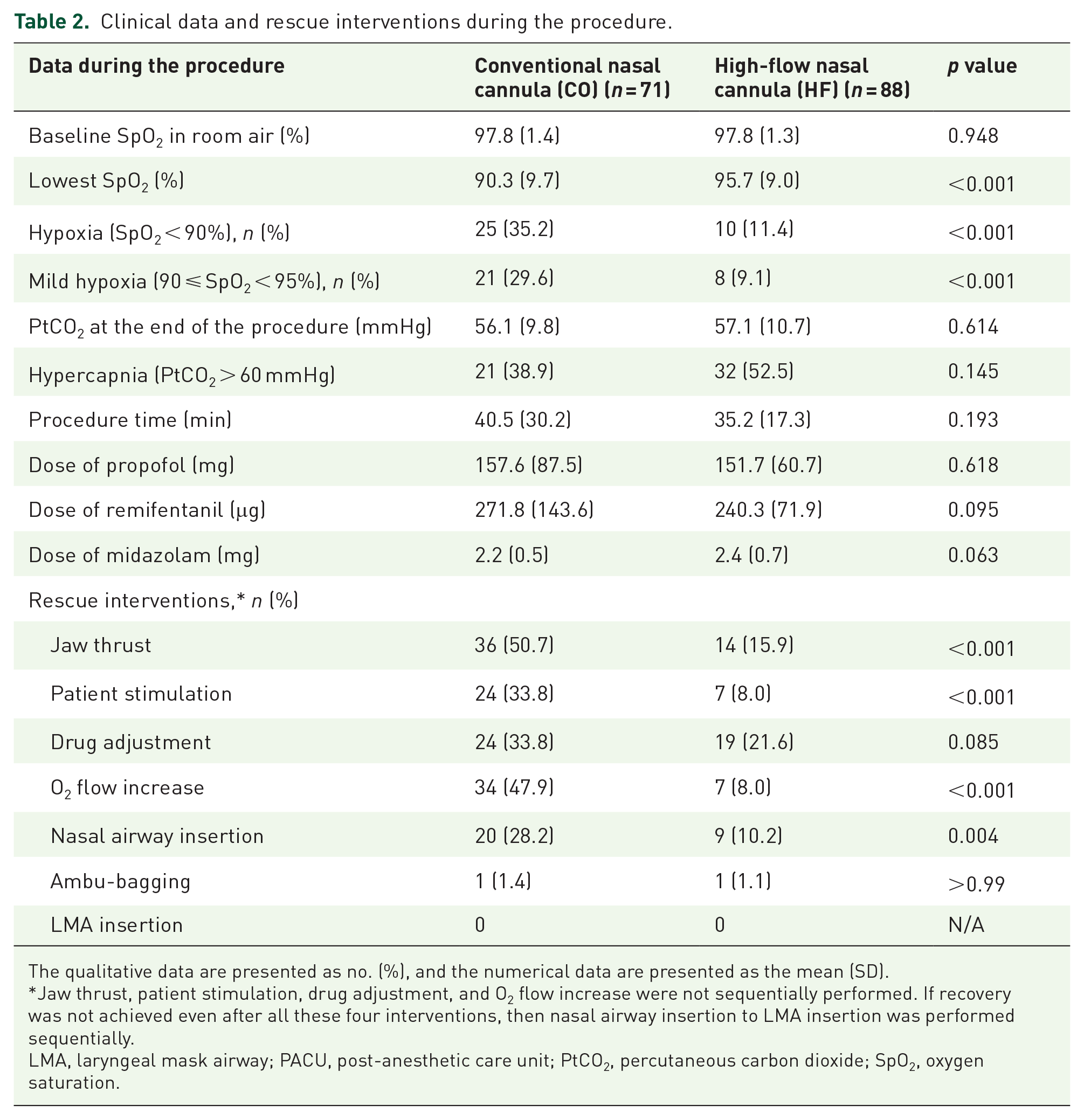
The qualitative data are presented as no. (%), and the numerical data are presented as the mean (SD).
Jaw thrust, patient stimulation, drug adjustment, and O2 flow increase were not sequentially performed. If recovery was not achieved even after all these four interventions, then nasal airway insertion to LMA insertion was performed sequentially.
LMA, laryngeal mask airway; PACU, post-anesthetic care unit; PtCO2, percutaneous carbon dioxide; SpO2, oxygen saturation.
In multivariable logistic regression analysis, the application of HF oxygen was a protective factor for hypoxia [odds ratio (OR) = 0.21, 95% CI: 0.08–0.58, p = 0.003]. Thus, difficult type of lesion (type C) was the only risk factor for hypoxia (OR = 11.31, 95% CI: 2.07–61.78, p = 0.005; Table 3).
Logistic regression analysis of risk factors associated with hypoxia.
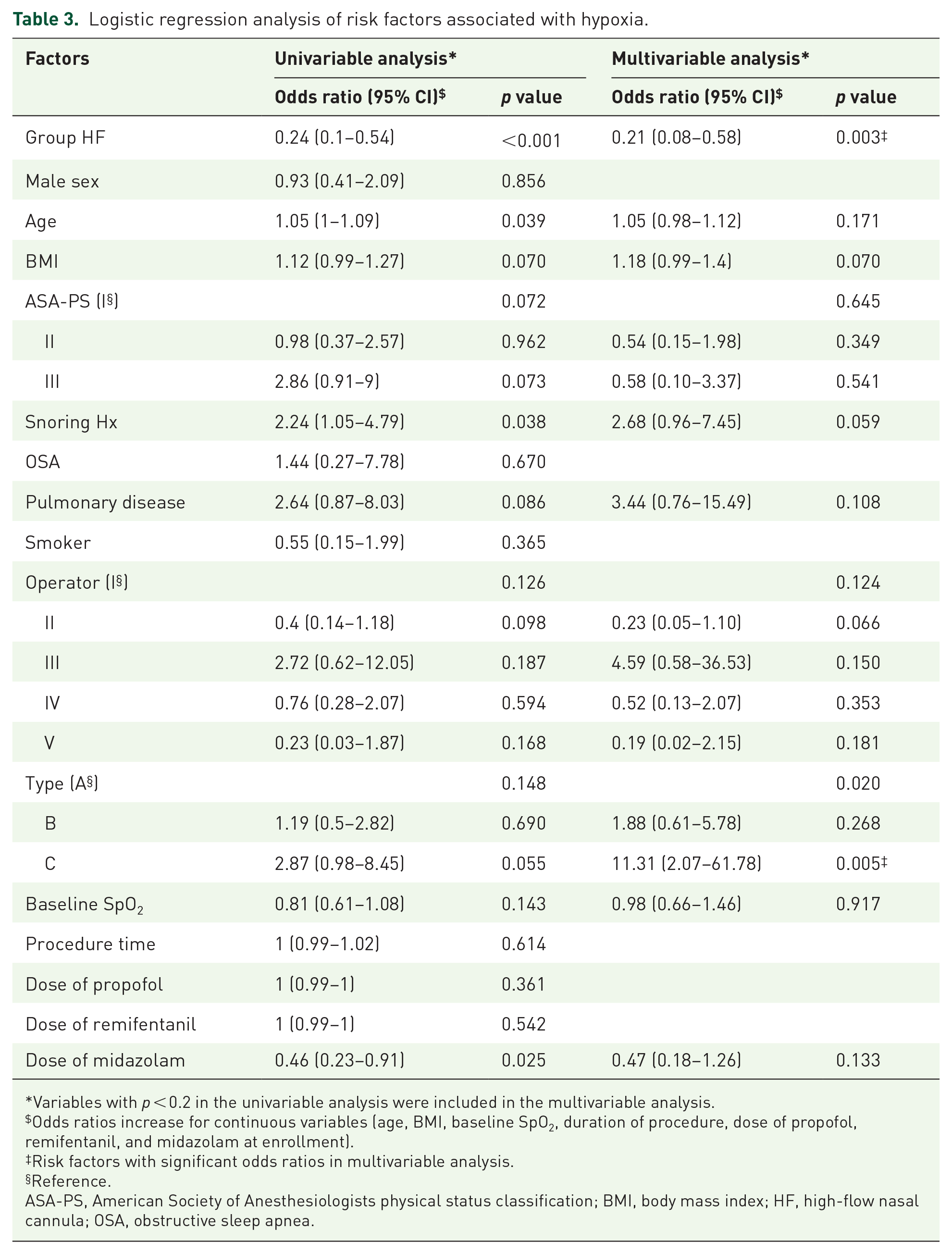
Variables with p < 0.2 in the univariable analysis were included in the multivariable analysis.
Odds ratios increase for continuous variables (age, BMI, baseline SpO2, duration of procedure, dose of propofol, remifentanil, and midazolam at enrollment).
Risk factors with significant odds ratios in multivariable analysis.
Reference.
ASA-PS, American Society of Anesthesiologists physical status classification; BMI, body mass index; HF, high-flow nasal cannula; OSA, obstructive sleep apnea.
Adverse events and complications associated with the procedure such as nausea in the post-anesthetic care unit, post-ESD bleeding, perforation, pneumonia, and hospital stay were comparable between the two groups (Table 4). Compared with group CO, group HF showed statistically higher incidence of abnormal findings (atelectasis, aspiration, and pneumoperitoneum) on chest radiography after the procedure [8% (11.3) versus 26% (29.5), respectively; p = 0.005; Table 4].
Adverse events and complications associated with the procedure.

The qualitative data are presented as no. (%), and the numerical data are presented as the mean (SD).
Fisher’s exact test was performed.
ESD, endoscopic submucosal dissection; PACU, post-anesthetic care unit.
In the power of sample size to address the primary outcome (the lowest SpO2 between the groups), group sample sizes of 71 (in group CO) and 88 (in group HF) achieved 89% power when the population mean difference was 5 with a standard deviation of 9.7 and with a significance level (alpha) of 0.05. It was calculated by PASS 2022 (NCSS, Kaysville, UT, USA).
Discussion
In this study, application of HFNC could improve oxygenation and reduced the incidence of hypoxia and mild hypoxia during deep sedation with propofol–remifentanil for ESD compared with conventional NC. However, group HF showed higher incidence of atelectasis or aspiration on chest radiography after the procedure. Thus, difficult type of lesion was the risk factor for hypoxia.
There have been several studies of the advantage of HFNC for effective oxygenation and prevention of hypoxia during sedation.6,11,12 One study reported no hypoxia (75% < SpO2 < 90% for <60 s) or severe hypoxia (SpO2 < 75% for any duration or 75% < SpO2 < 90% for >60 s) in the HFNC group (multicenter prospective study, n = 1994) compared with the NC group during gastroscopy with propofol sedation. 6 In another study during prone positioning for endoscopic retrograde cholangiopancreatography, hypoxia occurred only in the NC group. 11 HFNC appears to be excellent for oxygenation compared with conventional NC, especially when it is difficult to secure airway patency or when sufficient oxygen supply is limited such as in the prone or lateral position.
According to two recent meta-analyses, HFNC significantly reduced the risk of hypoxia compared to CO with a low-flow system in gastrointestinal endoscopic procedures under sedation.15,16 Findings of our study are largely consistent with these results. While the earlier published study 15 did not find a significant difference in the lowest oxygen saturation, subsequent meta-analysis 16 including one additional randomized controlled trial found that HFNC significantly improved lowest oxygen saturation, which was in line with our results. It seems clear that the use of a HFNC has an advantage in effective oxygenation and prevention of hypoxia during sedation of various endoscopic procedures compared to CO group. However, previous studies were limited in their reporting of hypercapnia, and most procedures were within 20 min. Also, there have been no studies investigating HFNC-associated complications such as findings of chest X-rays after procedure. Therefore, our study has strength in these aspects.
In contrast to other forms of oxygen therapy, HFNC enables the administration of FiO2 up to 100% at a maximum flow rate of 70 L/min via soft NC. 15 Physiologically, HFNC contributes to washout of pharyngeal dead space, reducing work of breathing, generation of a positive end-expiratory pressure, and improvement of mucociliary clearance. 17 These effects could explain the advantages of HFNC for improving oxygenation revealed by ours and other studies.
Although we showed a clear advantage of this high-flow system, the chest X-ray immediately after the procedure in this study showed that it might not be ideal. In this study, the HFNC group showed higher incidence of atelectasis and aspiration on postprocedural chest X-ray. Both atelectasis and aspiration are possible complications of deep sedation. Inadequate tidal volume and insufficient ventilation may cause atelectasis.18–20 Although it most commonly presents a benign course with spontaneous resolution within 48 h, if atelectasis persists longer, it can lead to significant morbidity and additional hospital care. 21 In one retrospective study (n = 349) using NC (2–6 L/min), radiographic atelectasis developed in 19.5% of cases. 21 In our study, the overall rate of atelectasis in both groups was 13.8%, and the rate in group HF was 19.3%.
Meanwhile, aspiration pneumonia is reported to occur in 0.3–14% of patients who had undergone ESD. 22 However, aspiration on X-rays alone cannot predict pneumonia and should be considered along with clinical symptoms and signs. In our study, only 1 of 10 patients who showed aspiration on X-ray progressed to pneumonia. In addition, one study reported that opioid (meperidine) affected the rate of aspiration. Those authors suggested that meperidine inhibited the gag reflex, which might increase the risk of aspiration. 23 Recently, a study on the scoring system that can predict aspiration pneumonia in ESD was published, reporting eight predictive factors (old age, male, higher BMI, longer procedure time, lesion located in the lower third of the stomach, larger tumor size, prolonged recovery time, and desaturation during ESD). 22 However, the type of NC was not considered in that study.
As HFNC provides continuous positive airways pressure, it theoretically is likely to be associated with reduced pharyngeal collapse and atelectasis.6,10 However, in group HF, the patient may have achieved deeper sedation while maintaining adequate oxygen saturation but insufficient ventilation by administering high-flow oxygen, resulting in the risk of atelectasis or aspiration higher than in group CO. Although not statistically significant, the incidence of hypercapnia (PtCO2 > 60 mmHg) was higher in the group HF than in the group CO [32 (52.5%) versus 21 (38.9%)]. Another possibility is high oxygen supply through HFNC. In the lateral decubitus position, lung in the dependent portion has low partial pressure of alveolar oxygen because of low ventilation/perfusion ratio.24,25 In this condition, higher FiO2 increases the net flow of oxygen from alveolar gas to capillary, and the excessive flow of alveolar gas can lead to a collapse of the lung. 25 The left lung in group HF had low ventilation and higher FiO2 with oxygen consistent 30–50 L/min supply compared to group CO with 6 L/min supply. As a result, more gas resorption might occur in the HF group.24,25
As adverse events related to HFNC, in addition to xeromycteria and rhinalgia, pharyngalgia, headache, epistaxis, and barotrauma (pneumothorax or subcutaneous emphysema) have been reported.26–29 According to one case report, a pneumomediastinum developed in a patient with coronavirus disease 2019 (COVID-19) pneumonia treated with HFNC. An increased gradient of pressure in the alveoli compared with the lung interstitium was described as a possible mechanism. 30 Therefore, the authors suggested that patients with a severe alveolar damage due to COVID-19 pneumonia and those with precipitating factors such as cough have the risk of pneumoperitonium caused by HFNC. Although they are rare, cases of pneumothorax and pneumomediastinum with possible complications of HFNC are observed in non-COVID-19 patients.31,32
In this study, difficult lesion was the risk factor for hypoxia. In our center, the gastroenterologist classifies the difficulty level into A (antrum or angle), B (body), C (fundus or cardia) considering the location, size, and fibrosis. Due to the high incidence of perforation in the upper part of the stomach, 33 the operator might have require changes in endoscopic manipulation, patient position, or gas inflation during the procedure with a type C lesion. We hypothesized that the procedure time or dose of propofol/remifentanil would have been greater in the type C lesion than in other types. However, there were no statistical differences in procedure time or dose of drugs between the two groups.
Our study has several limitations. First, this was a single-center study, and it is difficult to generalize the results. Other hospitals with different protocols may thus produce different results. Second, this was a retrospective study based on electronic medical records with a relatively small sample size. However, since an experienced anesthesiologist performed procedural sedation according to a well-established protocol, the collected data could be considered reliable. Further studies, such as prospective randomized controlled trials or a large-scale study, are required. Third, we could not measure the objective sedation depth such as bispectral index, and the degree of sedation depth in the two groups could not be reflected. Fourth, although we included various factors in analysis, we were unable to adequately control for confounders in the final model because the variable selection analysis may have excluded relevant confounders of hypoxia.
Conclusion
HFNC provided adequate oxygenation and a stable procedure without serious adverse events compared to conventional nasal flow during deep sedation of ESD. Moreover, difficult lesion was associated with the development of hypoxia. However, complications, such as pulmonary aspiration or atelectasis, that may arise from the use of an HFNC during deep sedation, should be considered.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231189957 – Supplemental material for Comparison of high-flow nasal cannula and conventional nasal cannula during sedation for endoscopic submucosal dissection: a retrospective study
Supplemental material, sj-docx-1-tag-10.1177_17562848231189957 for Comparison of high-flow nasal cannula and conventional nasal cannula during sedation for endoscopic submucosal dissection: a retrospective study by Seungwon Lee, Ji Won Choi, In Sun Chung, Duk Kyung Kim, Woo Seog Sim and Tae Jun Kim in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.