
Abstract
Background:
Readmission shortly after discharge is indicative of an increased disease severity for patients with ulcerative colitis (UC) and ineffectiveness to medical therapy, which may contribute to a dismal prognosis.
Objectives:
This study aimed to explore prognostic variables with a nomogram to predict unplanned UC-related readmission within 1 year after discharge.
Design:
A retrospective cohort study.
Methods:
Electronic medical records of all UC patients treated at our center between 1 January 2014 and 31 June 2021 were reviewed. A comprehensive analysis of various characteristics, such as demographics, comorbidities, medical history, follow-up appointments, admission endoscopy, histopathologic features, etc., was used to determine the primary end point, which was unplanned UC-related calendar year readmission.
Results:
We found that the unplanned UC-related readmission rate within 1 year was 20.8%. In multivariable cox analysis, the predictors of the Elixhauser comorbidity index [Hazard ratio (HR): 3.50, 95% confidence interval (CI): 1.93–6.37], regular follow-up (HR: 0.29, 95% CI: 0.16–0.53), any history of corticosteroid use (HR: 3.38, 95% CI: 1.83–6.27), seral level of C-reactive protein (HR: 1.01, 95% CI: 1.00–1.02), and the UC endoscopic index of severity (HR: 1.29, 95% CI: 1.05–1.57) independently predicted calendar year readmission after discharge. The established nomogram had a consistently high accuracy in predicting calendar year readmission in the training cohort, with a concordance index of 0.784, 0.825, and 0.837 at 13, 26, and 52 weeks, respectively, which was validated in both the internal and external validation cohorts. Therefore, UC patients were divided into clinically low-, high-, and extremely high-risk groups for readmission, based on the calculated score of 272.5 and 378.
Conclusion:
The established nomogram showed good discrimination and calibration powers in predicting calendar year readmission in high-risk UC patients, who may need intensive treatment and regular outpatient visits.
Key points
Previous studies described the potential risk factors for 30-day or 90-day readmission, including steroid use for chronic condition, Charlson comorbidity index, extensive colitis, and use of benzodiazepines for patients with ulcerative colitis.
Our work found that the Elixhauser comorbidity index, regular follow-up, any history of corticosteroid use, seral level of C-reactive protein, and the ulcerative colitis endoscopic index of severity independently predicted calendar year readmission after discharge.
Based on the five key risk factors, we established a novel nomogram for the prediction of calendar year readmission in UC patients, who are at high risk for readmission and may need intensive therapy and regular outpatient visits.
Introduction
Inflammatory bowel disease (IBD), a complex disorder, is characterized by vulnerable patients with susceptibility genes, environmental factors, bacterial translocation, and dysregulated immunity.1,2 Two major forms of idiopathic IBD are ulcerative colitis (UC) and Crohn’s disease (CD). The incidence and prevalence of these diseases have undergone significant shifts in North America and European countries. 3 In China, the reported prevalence rates are 4.59–57.3 per 100,000 and the incidence rates are 0.42–4.6 for UC (annual percentage change: +4.8%).3,4 The majority of mid-term complications of IBD include IBD-related surgery, hospitalization, and bowel damage, contributing to the considerable direct and indirect healthcare burden.5–7 The cumulative admission rate in UC ranged from 9% to 33% at 1 year and from 18% to 54% at 5 years after diagnosis, which accounted for 10–36% of costs for UC (annual mean cost per patient-year €2088). 8 The rehospitalization rates were 23.7%, 55.8%, and 74.6% during the follow-up period of 1, 5, and 10 years, respectively. 9 Readmission shortly after discharge reflected disease severity and a lack of response to medical therapy, which was often associated with colectomy and mortality with a dismal prognosis. 9 A significant proportion of patients were readmitted for UC-related causes such as gastrointestinal symptoms and extraintestinal manifestations. Main UC-related causes for hospitalization were diagnostic procedures (8–26.7%), disease relapse (43%), disease activity (22.4–49.6%), UC-related surgery (2.5–4.8%), medical therapy adjustment (22.4%), or infection/sepsis (27.8%).9–12 Readmission was significantly associated with hospital performance, increasing costs, irregular outpatient visits, and prolonged disease course.12,13
Previous studies have identified various potential risk factors associated with 30-day, 90-day, or 1-year readmission, such as steroid use for chronic condition, Charlson comorbidity index, extensive colitis, and use of benzodiazepines in UC.12,14,15 The Agency for Healthcare Research and Quality of the Elixhauser Comorbidity (AHRQ-Elixhauser index) ⩾3 16 and nonattendance to gastroenterologist outpatient follow-up 17 have been linked to 30-day readmission and calendar year mortality. In addition, mechanical ventilation for more than 24 h, human immunodeficiency virus, alcohol abuse disorder, and previous history of Clostridium difficile infection have been found to be independent predictors of 90-day readmission in UC patients. 18 Nghia H reported that pain interference, prior surgery, the need for biological agents, and any history of corticosteroid use were also predictive of high risk of rehospitalization within 1 year. 19 Furthermore, intensive care unit stay, male gender, black race, and outside hospital transfers have been shown to predict the risk for 1-year readmission. 20
To reduce the healthcare cost and improve UC patient prognosis, it is imperative to identify risk factors associated with calendar year readmission in UC patients. Unfortunately, there is a scarcity in recent literature on clinical risk factors associated with 1-year readmission in UC patients. Therefore, we conducted a systematic cohort study on risk factors for calendar year readmission in UC patients treated at our center.
Materials and methods
Study design and participants
This study was conducted at the Affiliated Drum Tower Hospital of Nanjing University Medical School, a tertiary teaching hospital with a large, established Digestive Endoscopy Center. All medical records diagnosed with colitis between 1 January 2014 and 31 June 2021 were reviewed. Inpatient admission and readmission for UC patients were evaluated and determined by attending gastroenterologists in the outpatient clinical setting. All UC patients admitted to the hospital underwent a comprehensive assessment, including general physical examinations, vital signs, blood tests, colonoscopy with mucosal biopsy, histopathology, and other relevant investigations. Upon discharge, every patient was given a detailed discharge summary, containing the detailed information on hospital course, outpatient clinical schedules, investigation results, medication changes, and follow-up management plan. Data collected over the study period were randomly divided into the training set and the internal validation set. The external validation set was carried out at the Wuxi People’s Hospital between 1 June 2017 and 1 June 2020.
Careful consideration was given to ensuring the maximum coverage of UC patients at outpatient clinic visits. The study exclusion criteria included (1) only with outpatient clinical visit records (without hospitalization); (2) incomplete information; (3) lost to follow-up within a year; (4) age <16 or >80 years; (5) initial admission for non-UC diseases or elective purposes; (6) maternal admissions, (7) benign or malignant tumor diagnosis; (8) UC-related surgery less than 3 months prior to initial admission; (9) severe systemic diseases; (10) patients who died at admission; and (11) missing readmission time information. In accordance with the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis guidelines, 21 we meticulously designed the study with the training, internal, and external validation cohorts, satisfying the same inclusion and exclusion criteria.
Definitions and predictors
Non-IBD colitides included ischemic colitis, microscopic colitis, eosinophilic colitis, segmental colitis associated with diverticula, radiation colitis, Behcet’s colitis, diversion colitis, etc. 22 Severe systemic diseases included congestive heart failure, chronic obstructive pulmonary disease, acute respiratory distress syndrome, end-stage chronic kidney disease (stage 5), acute renal failure, and acute or chronic liver failure. 23 The diagnoses were confirmed and validated based on the International Classification of Diseases, Tenth Revision, Clinical Modification. The research team captured various characteristics of each initial admission, including demographics, disease course, comorbidities, medical history, admission reasons, follow-up schedule, clinical findings at admission, medication history, laboratory test results, admission colonoscopy, biopsy histopathology, etc. Patients who were smoking or drinking at the time of initial admission were identified as active smokers or active drinkers. IBD-related surgery was referred to as colostomy, ileostomy, colorectal resection, ileocolic resection, ileal pouch-anal anastomosis, etc. AHRQ-Elixhauser index 24 is defined as a sum of individual composite scores based on the 38 comorbidities, such as iron-deficiency anemia, diabetes mellitus, hypertension, etc., which are related to readmission. The two major reasons for UC-related admission were gastrointestinal symptoms (diarrhea, purulent or bloody stool, abdominal pain, nausea, vomiting, loose stool, tenesmus, abdominal distension) and extraintestinal manifestations (erythema nodosum, pyoderma gangrenosum, arthritis, arthralgia, oral ulcers, fever, perianal disease). Regular follow-up was defined as monthly outpatient visits with attending gastroenterologists before admission. The Montreal disease extent and the UC endoscopic index of severity (UCEIS) were evaluated by two experienced gastrointestinal endoscopists according to the European Crohn’s and Colitis Organisation and the European Society of Gastrointestinal and Abdominal Radiology Guidelines 25 and histopathologic features determined by two experienced gastrointestinal pathologists according to the simplified Geboes score. 26
End point
The primary end point was the unplanned UC-related calendar year readmission where readmission was triggered by an IBD flare characterized by a deterioration of symptoms such as diarrhea, abdominal pain, bloody stool, or fever as defined before, 17 after an initial UC-related admission. ‘Calendar year readmission’ was considered as a time-to-readmission within a calendar year.
Statistical analysis
All statistical analyses were performed with SPSS version 26.0 (SPSS, Inc., Chicago, IL, USA) and R version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria). To analyze the baseline characteristics, continuous variables are reported as mean ± standard deviation (SD) (for parametrically distributed data) or median (interquartile range, IQR) (for nonparametrically distributed data). Any selective predictors that had missing data exceeding 15% were excluded. Missing categorical data were input based on an assumption that being missing was equal to the presence, while for continuous variables, missing data were replaced with either the mean (for normally distributed data) or median (for nonnormally distributed data). Univariable cox analysis was utilized to calculate the unadjusted hazard ratios (HRs) for the calendar year readmission. Multivariable cox analysis was performed with the selective predictors that were significant in the univariable cox analysis with a p value of <0.05 or seemed relevant to calendar year readmission with p > 0.05. Cumulative hazard of calendar year readmission among different subgroups in UC patients was estimated by Kaplan–Meier curves. Sex, age, and significant predictors were selected to establish a novel nomogram. To measure the predictive power of the nomogram, we evaluated the discrimination and calibration with a time-dependent receiver operating characteristic (ROC) curve and a calibration plot. The concordance index (c-index) was used to evaluate the predictive accuracy of the nomogram. The calibration function was evaluated by plotting the observed probability versus the predicted probability of readmission at different time points based on the nomogram. Two-sided p values <0.05 were considered significant.
Results
Baseline and clinical characteristics
We identified 3475 consecutive patients diagnosed with colitis at the Nanjing Drum Tower Hospital between 1 January 2014 and 31 June 2021 and 1034 consecutive patients at the Wuxi People’s Hospital between 1 June 2017 and 1 June 2020. The study inclusion and exclusion criteria for two hospitals were depicted in Figure 1, resulting in 432 eligible patients for analysis. The data from the Nanjing Drum Tower Hospital were randomly divided with a 7:3 ratio for the training set (N = 237) and the internal validation set (N = 103). The external validation set (N = 92) was collected from the Wuxi People’s Hospital. The calendar year readmission rates were 20.3% (48/237), 20.4% (21/103), and 22.8% (21/92) in the training set, internal, and external validation sets, respectively. The comparation of the reasons for the initial admission among three cohorts is shown in Supplemental Table 1.
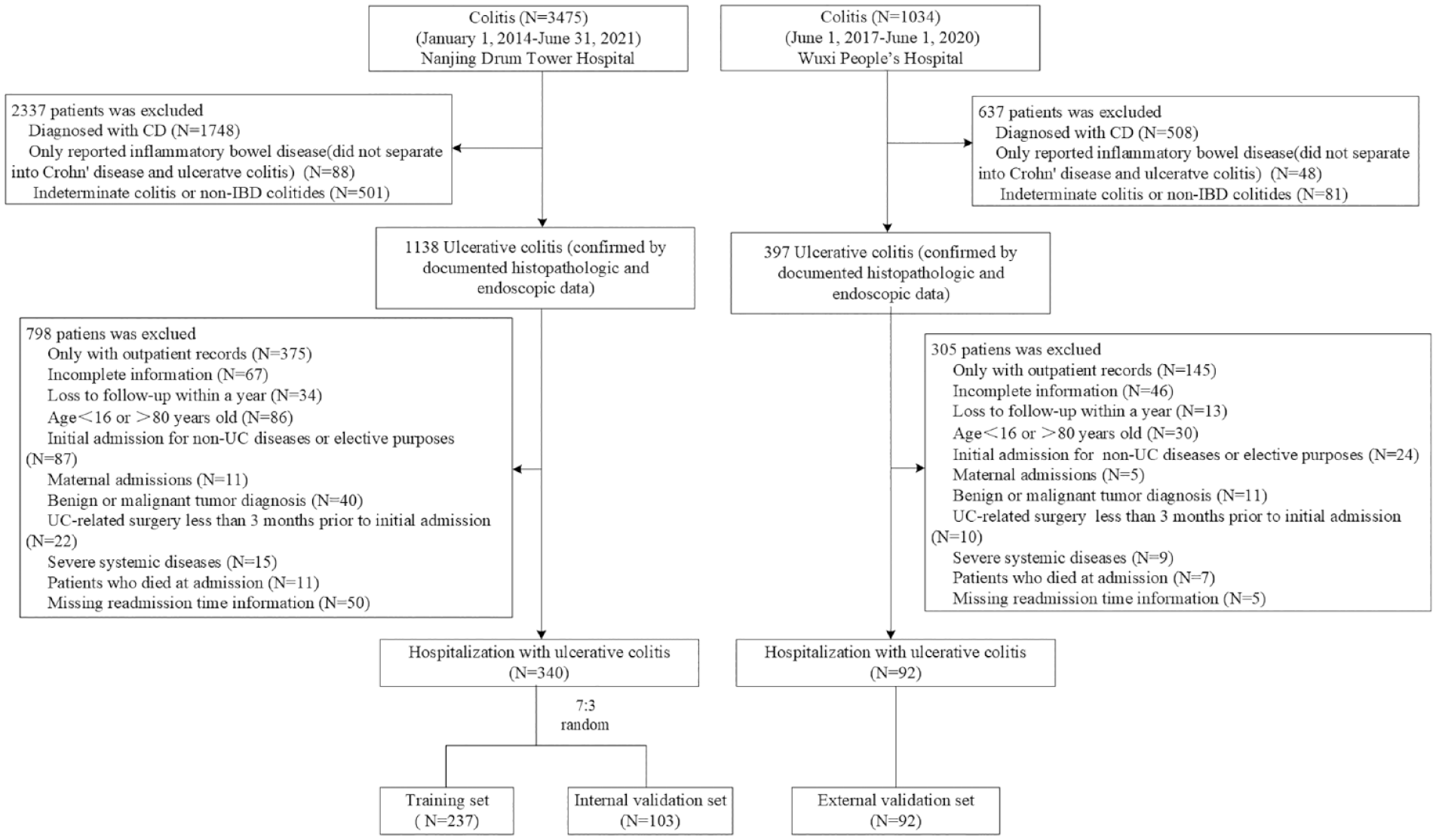
Flow diagram representing the study design with the inclusion and exclusion criteria.
The baseline and clinical characteristics of all enrolled patients are summarized in Table 1. The median age of the selective cohorts was 43.0 years (IQR: 30.0–55.0), and the median disease duration was 2.0 years (IQR: 0.0–5.0). An AHRQ-Elixhauser index ⩾3 was seen in 22.5% (97/432) of UC patients. Prior to admission, the majority of patients (71.1%) had received 1–2 types of medication, including 39.8% for a history of corticosteroid use, 8.1% for biological agents, and 8.3% with immunomodulators. Current use of biological agents (3.7%) and immunomodulators (3.7%) was reduced, compared to the historical use. The admission endoscopy was performed in 99.5% (N = 431) of patients with a median UCEIS score of 5 (IQR: 4–6). All comparations of baseline and clinical characteristics, except for the AHRQ-Elixhauser index (p = 0.038), were not statistically significant between the training and internal validation sets (Table 2). The differences in outpatient visits, use of medication, laboratory examinations, and UCEIS scores were significant between the two hospitals (p < 0.05). The comparation between the internal and external validation sets is shown in Supplemental Table 2.
The baseline and clinical characteristics of patients with UC between 2014 and 2021.

Data not available for all subjects. The missing number (n, %) of patients for each indicator: length of stay, n (%) = 15 (3.5%); hemoglobin, n (%) = 1 (0.2%); ESR (%), n = 46 (10.6%); albumin (%), n = 9 (2.1%); CRP (%), n = 8 (1.9%); admission endoscopy (%), n = 2 (0.5%); and histologic feature (%), n = 13 (3.0%).
AHRQ, Agency for Healthcare Research and Quality of the Elixhauser Comorbidity; 5-ASA, 5-aminosalicylic acid; CRP, C-reactive protein; EN, enteral nutrition; ESR, erythrocyte sedimentation rate; IBD, inflammatory bowel disease; UC, ulcerative colitis; UCEIS, the ulcerative colitis endoscopic index of severity.
The comparations of baseline and clinical characteristics between training and validation sets.

Data not available for all subjects. The missing number (n, %) of patients for each indicator in training set and internal validation set: length of stay, n (%) = 9 (3.8%), 6 (5.8%); hemoglobin, n (%) = 0 (0%), 1 (1.0%); ESR (%), n = 33 (13.9%), 13 (12.6%); albumin (%), n = 5 (2.1%), 4 (3.9%); CRP (%), n = 2 (0.8%), 6 (5.8%); admission endoscopy (%), n = 2 (0.8%), 0 (0%); histopathologic features (%), n = 10 (4.2%), 3 (2.9%). No missing number in external validation set.
Comparation between the training and internal validation sets.
Comparation between the training and external validation sets.
AHRQ, Agency for Healthcare Research and Quality of the Elixhauser Comorbidity; 5-ASA, 5-aminosalicylic acid; CRP, C-reactive protein; EN, enteral nutrition; ESR, erythrocyte sedimentation rate; IBD, inflammatory bowel disease; UCEIS, the ulcerative colitis endoscopic index of severity.
Univariate cox analysis for readmission
In univariate analysis, basic demographics, comorbidities, medication use, laboratory examinations, and endoscopic and histopathologic features in the training set were analyzed for the calendar year readmission (Table 3). For general physical conditions recorded by the physician, the patients who were active drinkers (p = 0.001), with longer disease duration (p = 0.028) and higher AHRQ-Elixhauser index (p < 0.001), were more likely to be readmitted within a calendar year. As for medication use, the patients with any history of use of corticosteroids (p = 0.001) and immunomodulators (p = 0.022) had a higher likelihood of readmission, whereas those using 5-aminosalicylic acid (5-ASA) currently (p < 0.001) had a lower likelihood of readmission. Moreover, a lower seral level of hemoglobin (p < 0.001) and albumin (p < 0.001) and a higher seral level of C-reactive protein (CRP) (p = 0.004) and UCEIS (p < 0.001) indicated a higher risk of readmission.
Univariate cox analysis of predictors of calendar year readmission in UC patients.
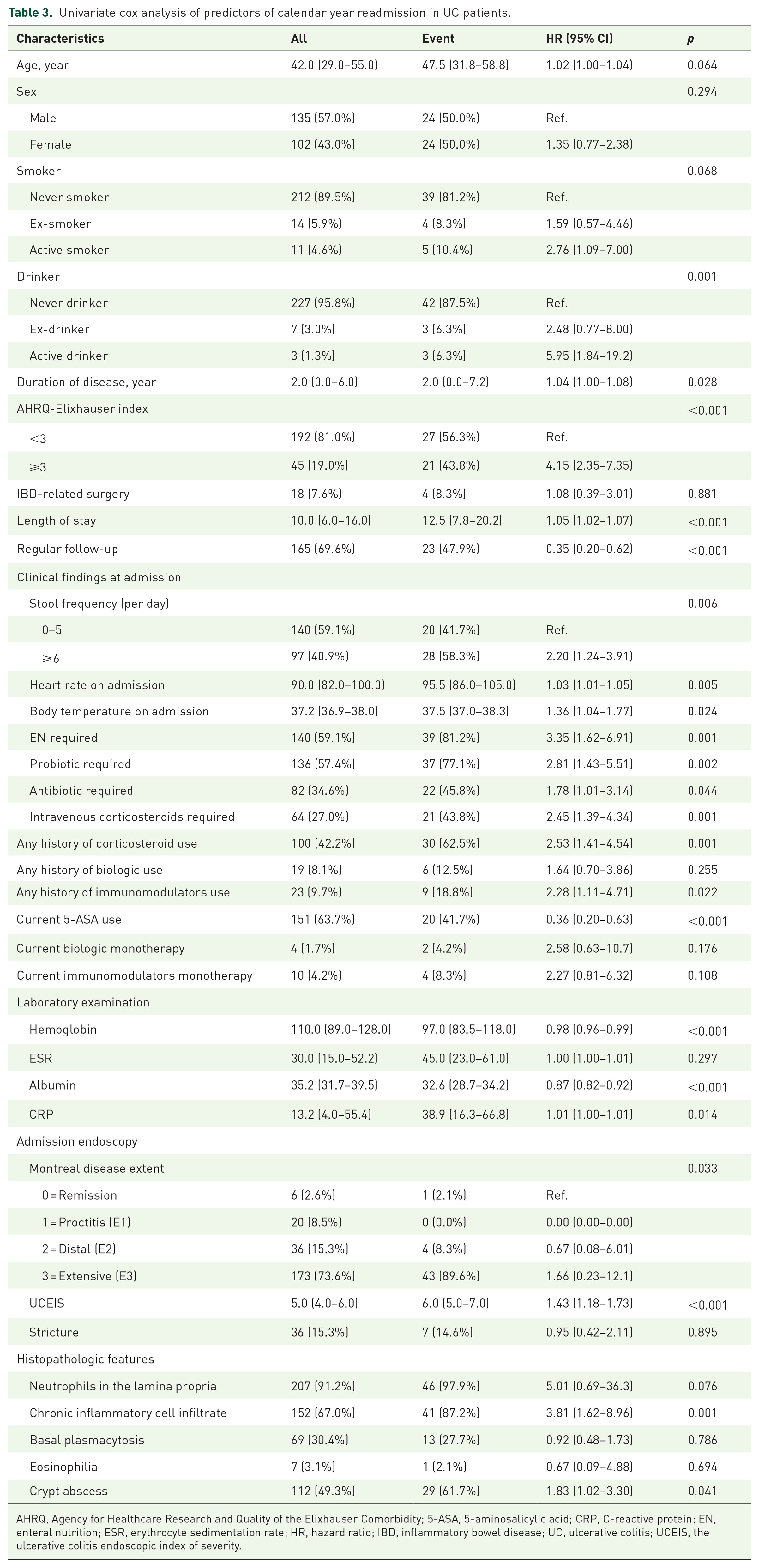
AHRQ, Agency for Healthcare Research and Quality of the Elixhauser Comorbidity; 5-ASA, 5-aminosalicylic acid; CRP, C-reactive protein; EN, enteral nutrition; ESR, erythrocyte sedimentation rate; HR, hazard ratio; IBD, inflammatory bowel disease; UC, ulcerative colitis; UCEIS, the ulcerative colitis endoscopic index of severity.
Multivariate cox analysis for readmission
With multivariate analysis, the AHRQ-Elixhauser index [HR: 3.50, 95% confidence interval (CI): 1.93–6.37], any history of corticosteroid use (HR: 3.38, 95% CI: 1.83–6.27), and higher seral levels of CRP (HR: 1.01, 95% CI: 1.00–1.02) and UCEIS (HR: 1.29, 95% CI: 1.05–1.57) were found to be independently associated with an increased risk of calendar year readmission (Table 4). The regular follow-up (HR: 0.29, 95% CI: 0.16–0.53) was associated with a reduced risk of calendar year readmission (Table 4).
Multivariate cox analysis of predictors of calendar year readmission in UC patients.
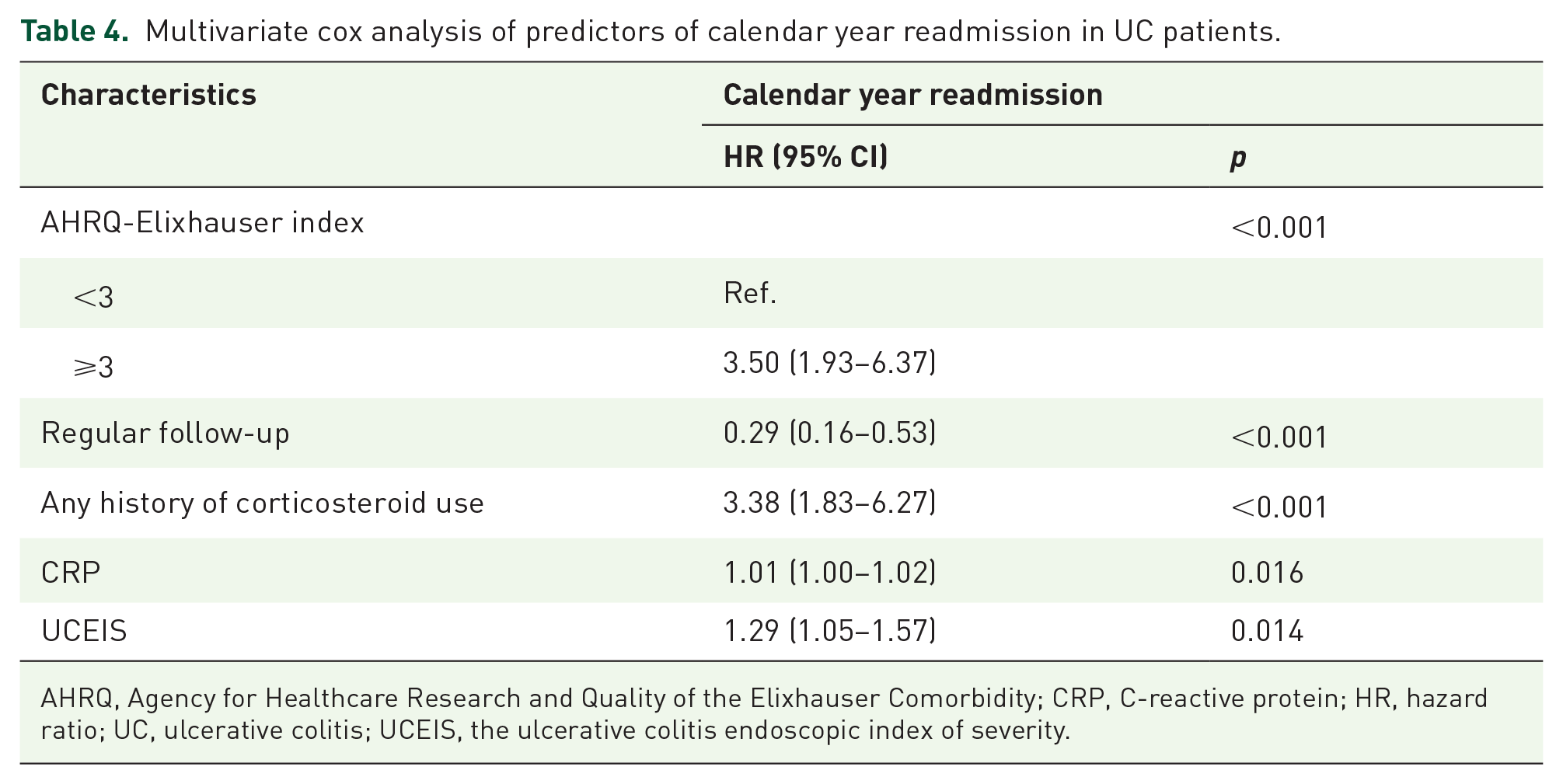
AHRQ, Agency for Healthcare Research and Quality of the Elixhauser Comorbidity; CRP, C-reactive protein; HR, hazard ratio; UC, ulcerative colitis; UCEIS, the ulcerative colitis endoscopic index of severity.
Development and validation of the predictive nomogram
By assigning a weighted score to each of the predictive variables obtained from the multivariable cox model (Figure 2), we established a nomogram to calculate the likelihood of readmission at 13, 26, and 52 weeks after discharge. The established nomogram was validated by a bootstrap resampling procedure and the integrated c-indexes were 0.784 (95% CI: 0.639–0.930), 0.825 (95% CI: 0.733–0.917), and 0.837 (95% CI: 0.772–0.910) at 13, 26, and 52 weeks of readmission, respectively (Figure 3(a)). The c-indexes were 0.914 (95% CI: 0.850–0.978), 0.782 (95% CI: 0.653–0.912), 0.764 (95% CI: 0.637–0.892) at 13, 26, and 52 weeks of readmission, respectively, for the internal validation cohort, and 0.798 (95% CI: 0.689–0.933), 0.795 (95% CI: 0.614–0.977), and 0.812 (95% CI: 0.689–0.934), respectively, for the external validation cohort (Figure 3(b) and (c)). The calibration curve (Figure 3(d)) demonstrated a high consistency between predicted probability and observed probability at different time points, as well as the internal and external validation sets (Figure 3(d)–(f)). We next divided the total score into two subgroups based on the median score of the training set (272.5), equal to the function result of restricted cubic spine (Figure 4). The readmission risk, corresponding to the median score of 272.5, was 3.3%, 6.4%, and 13.9% at 13, 26, and 52 weeks after discharge, respectively (Supplemental Figure S1). Figure 5(a) to (c) shows that the scores above the median (⩾272.5) showed a significantly higher risk than those below the median (<272.5) in all three cohorts (p < 0.001). The calculated score ⩾378 corresponded to the risk of 30-day readmission ⩾24.1%, 13-week readmission ⩾55.5%, 26-week readmission ⩾81.4%, and 52-week readmission ⩾97.7%, respectively (Supplemental Figure S1).

Nomogram for calculating likelihood of readmission in UC patients. Points are calculated for each indicator and summed, from which probability can be calculated from the bottom row.

Internal and external validation of the nomogram model. (a)–(c) Receiver operating characteristic curve for the nomogram generated using bootstrap resampling (1000 times) at different time points. (a) The training set, (b) the internal validation set, and (c) the external validation set. (d)–(f) Calibration plot of observed probability versus predicted probability of readmission at different time points based on the novel nomogram. (d) The training set, (e) the internal validation set, and (f) the external validation set.

HRs for the readmission based on restricted cubic spine function for total points. The purple line represents the reference of the HRs, and the purple area represents 95% confidence intervals.
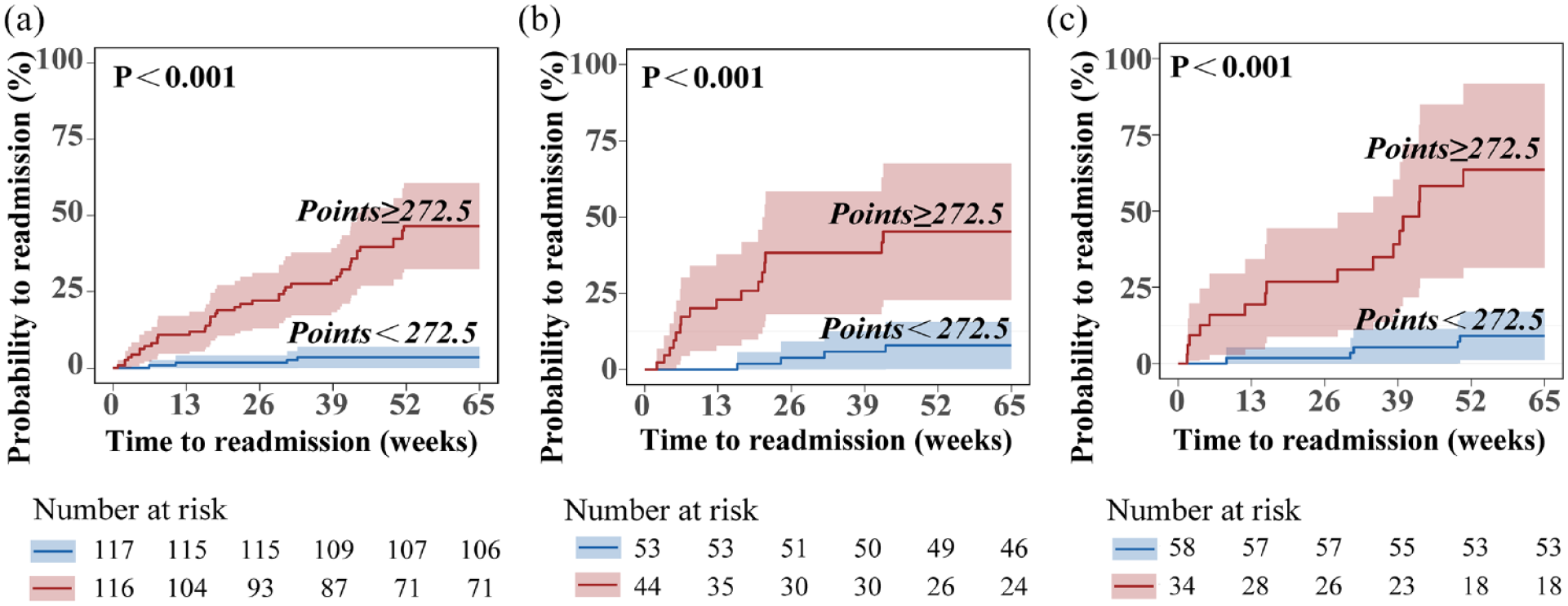
Cumulative hazard of calendar year readmission between different subgroups of total points in UC patients. (a) The training set, (b) the internal validation set, and (c) the external validation set.
Discussion
In our study, the UC-related rehospitalization rate within 1 year after discharge was 20.8%, which was consistent with that previously reported.27,28 Different studies of temporal trends of rehospitalization varied from 9% to 52.8% substantially in different countries after 1 year of follow-up.3,8 In addition, the median length of hospital stay (10.0 days, IQR: 6.0–15.0) was a bit longer than that of previous studies (5.9–8.0 days). 28 Repeated unplanned rehospitalization could exacerbate the disease course and economic burden. In our study, we established and validated a nomogram to predict the risk of calendar year readmission in UC patients. Our nomogram integrated various risk predictors, many of which have already been proven to be associated with readmission.16,17,19,29 We confirmed and expanded those risk factors, and further identified independent risk factors associated with the calendar year readmission, such as AHRQ-Elixhauser index, regular follow-up, any history of corticosteroid use, high seral levels of CRP, and UCEIS.
Our study combined clinical findings, medication use, laboratory tests, and endoscopic features to stratify the risk of calendar year readmission. Although certain variables, such as alcohol abuse, duration of disease, seral levels of albumin, and use of immunomodulators, showed predictive values individually, they were not independent risk factors in our multivariate analysis. The results of the ROC curve and calibration plot showed that our established nomogram performed well for the prediction of readmission at 13, 26, and 52 weeks in UC patients. In addition, both internal and external validation cohorts for our established nomogram also demonstrated good discrimination and calibration with the following features. First, strict inclusion and exclusion standards were used for the patient population selection. Second, both training and validation sets were obtained from the same patient population in the Jiangsu Province, where UC patients were treated similarly, according to the disease severity. Third, the difference in the readmission rate was not significant between the Nanjing Drum Tower Hospital and the Wuxi People’s Hospital. Nonetheless, the lack of adequate samples could lead to an unbiased property statistically and the strict inclusion and exclusion criteria may limit the extensive use of the established nomogram. The readmission risk cutoff score from our subgroup analysis (⩾272.5 and <272.5) (Figure 5) showed that the nomogram could be used to stratify the risk of UC patients as well.
As previously described, 30 variables such as preexisting congestive heart failure, pulmonary embolism, renal insufficiency, sepsis, and deep vein thrombosis are effective in risk stratification for 30-day readmission in UC after colectomy or proctectomy. Other factors associated with increased risk of readmission within 1 year include nonalcoholic fatty liver disease [adjusted hazard ratio (aHR): 1.65, 95% CI: 1.46–1.86; p < 0.01], frailty (aHR: 1.21, 95% CI: 1.17–1.25), and UCEIS (p < 0.01), which were also associated with a prolonged length of hospital stay (p < 0.01) and high cost of care (p < 0.01).29,31,32 A weighted logistic regression model and a discharge–readmission model have been used to assess the readmission risk score in UC patients with or without surgery.12,30 Another nomogram with several variables of in-hospital complications, long operating time, or the need for a higher level of care at discharge was reported to be quite predictive of risk for the readmission in patients who underwent general surgery. 33 However, limitations of these studies included a lack of endoscopic and histopathologic features, inadequate medication history, and incomplete dataset regarding calendar year readmission in UC patients. An accurate individualized prediction nomogram is necessary for healthcare providers to identify high-risk UC patients who could benefit from intensive in-hospital treatment, and also to decrease readmission rates, healthcare costs, and improve UC patient life quality. When the calculated risk score is ⩾272.5, according to our nomogram, patients should be followed up regularly. As previously reported, 14 when we consider only the risk of short-term mortality for the likelihood of 30-day readmission in UC patients, the intensive treatment threshold was 24.1% risk of 30-day readmission in our study, which corresponds to the risk score of ⩾378 and clinicians should be vigilant in this scenario (as indicated in Supplemental Figure S1). A combination use of 5-ASA, corticosteroids, biologic agents, and immunomodulators may reduce the levels of UCEIS and CRP during initial admission. Additional measures, such as enteral nutrition, probiotics, and antibiotics, could have beneficial effects on the balance of gut microbes. Regular follow-up and rational medical therapy could reduce the risk of readmission. The UC patients above the risk threshold should be reevaluated 1–2 weeks after the intensive medical therapy to assess the therapeutic efficacy.
There are some limitations in our nomogram proposal for predicting calendar year readmission in UC patients. First, our clinical samples are relatively small to reach definitive and concrete conclusions on the predictive power of the nomogram. We have made efforts to include comprehensive clinical information on patients, which is in line with the establishment of prediction models. Second, the data were collected only in our hospital and Wuxi People’s Hospital, which may limit the applicability of our established nomogram to UC patients treated at other hospitals. It would be valuable to test the prognostic accuracy of our model in other institutions in future studies. Third, although we have included explanatory variables as much as possible in our analysis, there were some potential predictors that were not covered, such as income, body mass index, fecal calprotectin, Charlson comorbidity index, and depression. Further studies could take these additional factors into consideration. Lastly, it is worth noting that the study was retrospective without a randomized controlled trial, which could introduce inherent biases and unknown confounders. Therefore, we recommend that prospective studies would be conducted to test the generalizability of our nomogram in large cohorts.
In conclusion, we established a nomogram on clinical factors that allowed accurate prediction of calendar year readmission in UC patients. The user-friendly graphical interfaces of the nomogram could be used to identify high-risk patients who could benefit from the intensive treatment and facilitate clinical decision-making. Moving forward, we could further test the clinical utility of the predictive nomogram in prospective randomized controlled trials.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231189124 – Supplemental material for A nomogram based on clinical factors to predict calendar year readmission in patients with ulcerative colitis
Supplemental material, sj-docx-1-tag-10.1177_17562848231189124 for A nomogram based on clinical factors to predict calendar year readmission in patients with ulcerative colitis by Ying Xiang, Ying Yuan, Jinyan Liu, Xinwen Xu, Zhenyu Wang, Shahzeb Hassan, Yue Wu, Qi Sun, Yonghua Shen, Lei Wang, Hua Yang, Jing Sun, Guifang Xu and Qin Huang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-2-tag-10.1177_17562848231189124 – Supplemental material for A nomogram based on clinical factors to predict calendar year readmission in patients with ulcerative colitis
Supplemental material, sj-tif-2-tag-10.1177_17562848231189124 for A nomogram based on clinical factors to predict calendar year readmission in patients with ulcerative colitis by Ying Xiang, Ying Yuan, Jinyan Liu, Xinwen Xu, Zhenyu Wang, Shahzeb Hassan, Yue Wu, Qi Sun, Yonghua Shen, Lei Wang, Hua Yang, Jing Sun, Guifang Xu and Qin Huang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.