
Abstract
In the absence of secondary causes, eosinophilic esophagitis (EoE) is a chronic, local, progressive, T-helper type 2 immune-mediated disorder characterized by symptoms of esophageal dysfunction and eosinophil-predominant inflammation. In the last 20 years, the incidence and prevalence of EoE have risen sharply, and the chances of encountering affected patients in clinics and endoscopy rooms have increased. Nevertheless, it is estimated that the mean diagnostic delay of EoE is 4–6 years in both children and adults. Unfortunately, the longer the disease stays unrecognized, the likelier it is for the patient to have persistent or increased esophageal eosinophilic inflammation, to complain of non-resolving symptoms, and to develop fibrotic complications. Early detection depends on the recognition of initial clinical manifestations that vary from childhood to adulthood and even among patients of the same age. The disease phenotype also influences therapeutic approaches that include drugs, dietary interventions, and esophageal dilation. We have herein reviewed epidemiologic, clinical, endoscopic, and histologic features and therapeutic options of EoE focusing on differences and similarities between children and adults that may certainly serve in daily clinical practice.
Introduction
Eosinophilic esophagitis (EoE) is a chronic, progressive, T-helper type 2 (Th2) immune-mediated disorder characterized by symptoms of esophageal dysfunction and eosinophil-predominant inflammation, in the absence of secondary causes of eosinophilia.1–3 The inflammatory response is restricted to the esophagus as the stomach and the duodenum are never involved. 4 The pathogenesis relies on a complex interaction between genetics and environment 5 triggering an immune response against the insult of food allergens penetrating through a defective esophageal mucosal barrier. 6 In patients who are predisposed to EoE, the exposure to environmental allergens induces a chronic inflammatory esophageal response mediated by both the innate and the adaptive immune systems, which involves the participation of eosinophils, mast cells, dendritic cells, basophils, T and B lymphocytes, immunoglobulins (Ig), and mediators such as IL (Interleukin) -4, IL-5 and IL-13, which act in concert causing progressive organ dysfunction.
Genes have an estimated contribution of 14.5% to the pathogenesis of EoE and this is supported by high rates of proband concordance, which is 58% and 36% in monozygotic and dizygotic twins, respectively. 5
Most of the genes involved in the pathogenesis of EoE influence Th2 lymphocytes-mediated responses or epithelial barrier integrity, being key players in such mechanisms the thymic stromal lymphopoietin, encoded on locus 5q22 -, 7 CAPN14, encoded on locus 2p23 -, 8 and the epidermal differentiation complex encoded on locus 1q21. 9
To date, 31 independent EoE risk loci have been associated to EoE; 10 however, it has been estimated that environmental contribution to the variance of EoE heritability is larger than genetics, which is around 81%. 5 Environmental risk factors associated with EoE include maternal fever during pregnancy, cesarean delivery, use of antibiotics, or acid-suppressive therapy during infancy. 11 Factors that are negatively associated to the disease include living with a furred pet at home and the Helicobacter pylori infection,11–13 although a recent multicenter case-control study did not confirm this negative association. 14 Interestingly, no association between EoE and breast-feeding, maternal smoking, maternal use of folic acid or multivitamin supplements has been found to date. 11
Although the incidence and prevalence of EoE were believed to be rare prior to the past two decades, they have sharply increased over years 2 and now constitute a prevalent disease, with rates comparable to Crohn’s disease. 15 Notably, several population-based studies from the United States16,17 and Europe17,18 have provided evidence of a true increase, rather than a mere increase in recognition or biopsy rate.15,19
EoE is considered the most frequent eosinophilic gastrointestinal disorder. 20 The estimated incidence in adults and children is 7.0 and 5.1 per 100,000/year, respectively; the estimated overall pooled prevalence is 22.7/100,000; it is higher in adults (32.5/100,000) than in children (19.1/100,000). 21 EoE is more common in males, with a 3:1 male to female ratio at all age groups.21,22 The peak incidence is between 20 and 40 years of age. 21 Up to 22% of patients undergoing upper endoscopy for non-obstructive dysphagia23,24 and over 50% of patients referred for food impaction receive a diagnosis of EoE.25,26 Most patients have co-occurring allergic rhinitis, asthma, IgE-mediated food allergies and atopic dermatitis, and children show higher hypersensitivity against food antigens. 27
Symptoms vary according to the age of diagnosis. Non-specific symptoms affect children, while dysphagia and food impaction are predominant in adults. Endoscopic features change from childhood to adulthood; this is because chronic inflammation drives a progressive fibrosis and esophageal remodeling. 28
Treatment options include drugs (Table 1), and dietary and endoscopic interventions. Approaches depend on clinical features and the age of patients, but also reflect on the preferences of the recruiting center.
Summary and dosage of PPIs and steroids in EoE patients. 29

It has been shown that children could be kept in remission with Esomeprazole 1 mg/kg daily and that adults could be kept in remission with Esomeprazole 20 mg daily. 30
Topical steroids may be administered in single or split dose. 29
Budesonide 0.5 mg daily could keep in remission for 50 weeks 36% of adults included in a randomized double-blind placebo-controlled trial. 31
PPIs, proton pump inhibitors.
The following sections discuss clinical, endoscopic, histologic, and therapeutic differences and similarities between children and adults.
Search strategy and study selection
According to the aim of this narrative review, we provided an overview of the evidence from original research articles, reviews, and randomized controlled trial (RCT) data, describing the main differences in clinical presentation and diagnostic and treatment approach to EoE among adult and pediatric patients. We conducted a literature review using the electronic databases PubMed/MEDLINE and the Cochrane Library. Search terms used included “eosinophilic esophagitis,” “epidemiology,” “pathogenesis,” “clinical presentation,” “dysphagia questionnaires,” “upper endoscopy,” “histology,” “proton pump inhibitor,” “topical steroids,” “budesonide,” “fluticasone,” “biological treatment,” “monoclonal antibodies,” “dietary interventions,” and “endoscopic dilation.” The term “eosinophilic esophagitis” was used as the MeSH term. Two authors independently reviewed all manuscripts published from January 1990 to April 2020. All RCT trial data as well other literature was included, based on a consensus decision of scientific merit by the reviewing authors.
Clinical presentation in children and adults
Symptoms of EoE follow a hierarchal and pyramidal pattern from early childhood to adulthood (Table 2). Clinical presentation in young children is reported and filtered by the caregiver. Infants and toddlers usually present non-specific symptoms such as reflux-like symptoms, vomiting, nausea, abdominal pain, food refusal, and failure to thrive. 32 It has been widely described that clinical presentation varies by age: failure to thrive in the youngest children (median age 2.0 years), vomiting in older children (median age 8.1 years), abdominal pain in young adolescents (median age 12.0 years), and dysphagia (mean age 13.4 years) and food impaction (median age 16.8 years) in older adolescents. 16

Adolescents >13 years old have a similar clinical presentation to adults
In contrast, adults predominantly complain of dysphagia to solids, followed by food impaction. The impaction of a food bolus is a typical and recurring symptom 33 which sometimes requires an emergency upper endoscopy for unblocking. 3 EoE can mimic gastroesophageal reflux disease (GERD) in its presentation with heartburn and regurgitation. Exercise-induced chest pain is also common among adults. 34 Some patients report minimal symptoms, and in such cases, the clinician should investigate dietary and behavioral modification, that is, eating slowly, excessive mastication before swallowing, drinking often to push the bolus down while eating, and avoidance of solid foods; this is so that patients spontaneously adapt to the reduced distensibility of the esophagus.
Both children and adults have higher rates of allergic diathesis than the general population27,32 and most patients have asthma, eczema, or allergic rhinitis. 35 Accordingly, EoE is more commonly associated to IgE-mediated food sensitization in children, and milk, eggs, soy, wheat/rye, beef, and peanuts are the main triggers. 36 In adults, hypersensitivity to aeroallergens such as pollens is also common. 37 Despite such strong evidence of IgE-mediated hypersensitivity, EoE is not directly mediated by IgE 38 and eosinophils, mast cells, lymphocytes and other inflammatory cells and cytokines are also involved. 4
Monitoring symptoms in EoE: scoring systems in children and adults
Patient-reported outcome measures have been proposed as co-primary therapeutic outcomes in EoE, along with histologic and endoscopic improvement.39,40 This is similar to what has been done with inflammatory bowel diseases. 41 The standardization of EoE activity measurement through patient reported and clinical outcome measures will also allow comparisons of the efficacy of different treatment modalities and will aid in the definition of clinically relevant endpoints that still need to be standardized. 40
Several scoring systems have been developed for the comprehensive evaluation of EoE.
In adults, the Eosinophilic Esophagitis Activity Index was found to have the best validity and responsiveness in a recent systematic review: 39 this tool focuses on dysphagia induced by food of different consistencies and behavioral adaptation in daily life.
The Pediatric Eosinophilic Esophagitis Symptom Score correlates with histologic activity, and the Pediatric Quality of Life Inventory EoE is the most valid symptomatic measure in children.
The aforementioned indexes are useful in monitoring symptoms and quality of life; nevertheless, clinicians should not rely solely upon symptoms to make assumptions on the biological activity of EoE, as their predictive value is currently scarce. 29
Endoscopic features and histology
Noninvasive tests that diagnose EoE or monitor its activity are currently considered inaccurate, 29 thus esophago-gastroduodenoscopy (EGD) and esophageal biopsies are crucial in the diagnosis and assessment of responsiveness to treatments both in children and adults.
Endoscopic abnormalities may be present in up to 93% of patients with EoE. 42 Typical endoscopic findings include fixed rings (“trachealization”), transient rings (“felinization”), white plaques or exudates, furrows, edema, strictures, and mucosal fragility on the passage of the endoscope (referred to as “crêpe-paper esophagus”) and a narrowed esophageal caliber. 43
The prevalence of such findings varies by age. Children commonly show an inflammatory-predominant esophageal pattern with exudates, furrows, and edema, whereas adults more frequently present rings and strictures, 42 although different patterns may coexist in the same patient. 4 The switch from an inflammatory to a fibrotic phenotype reflects the progressive remodeling of the esophagus led by chronic inflammation.28,44,45
In 2012, Hirano et al. validated a grading system for EoE called endoscopic reference score (EREFS) (Table 3); it is based on five major endoscopic features (exudates, rings, edema, furrows, strictures), but minor features are also evaluated (felinization, narrowed caliber and crêpe-paper sign). 46 The application of the EREFS score in adults led to an excellent prediction of EoE in a prospective study, with an area under the curve (AUC) of 0.934 using receiver operating characteristic analysis. 47
Endoscopic reference score of eosinophilic esophagitis. 46

Another prospective study on children showed that with a composite EREFS score (made up of the sum of the maximal overall score for each individual sign), children with EoE with an AUC of 0.93 were identified. The score identified children with active EoE before treatment (AUC of 0.81) and after treatment (AUC 0.79). 48
Further, a composite EREFS inflammatory score (considering the three inflammatory endoscopic features of EoE, namely edema, exudates, furrows) has shown to be highly correlative with eosinophilia and to effectively identify EoE versus controls and differentiate active versus inactive disease in children. 48
Unfortunately, up to 25% of patients do not show endoscopic abnormalities,17,49 and this is more common in children. 43 Moreover, although useful, endoscopic features alone do not establish a reliable diagnosis of EoE or assess disease activity. 29
Unlike endoscopic features, histology is similar between children and adults, although collagen deposits increase with the patient’s age.43,50
Biopsies are currently mandatory to evaluate eosinophil infiltrates and optional additional histological markers such as eosinophils microabscesses, basal zone hyperplasia, dilated intercellular spaces, eosinophil surface layering, papillary elongation, and lamina propria fibrosis 29 which, when systematically evaluated adopting the EoE histology scoring system, allows an objective assessment of histologic changes beyond the number of eosinophils. 51
It is recommended that at least six biopsies be taken from two different locations in the esophagus (usually proximal and distal halves). Since esophageal eosinophilia has a patchy nature, 52 biopsy sampling should primarily focus on areas with endoscopic mucosal abnormalities 29 which are associated with higher peak eosinophil counts. 53 When there is clinical suspicion of EoE and the endoscopic appearance is normal, biopsies should be randomly taken from the proximal, mid and distal esophagus. 42 In addition, biopsies from the duodenum and stomach should be collected to rule out eosinophilic gastroenteritis.29,54
The histological diagnosis is confirmed when 15 or more eosinophils are counted per high-power field (HPF) in biopsy specimens from proximal/mid esophagus. 29 However, the lack of a standardized diameter for the HPF on microscopes can lead to variations in the eosinophil density. 55 The threshold of 15 eosinophils/HPF has shown to have a sensitivity of 100% and specificity of 96% 56 and to reliably distinguish EoE from GERD, 19 which is associated with lower counts of eosinophils and usually involves the distal part of the esophagus. However, EoE and GERD may coexist, although their relationship is not completely understood.29,57
Abnormal eosinophilic esophageal infiltration could be related to secondary causes, thus GERD, eosinophilic gastroenteritis, hyper-eosinophilic syndrome, Crohn’s disease, celiac disease, connective tissue disorders, achalasia, infections, graft-versus-host reactions, and causative drugs should be excluded. 1
Endoscopy with biopsies is required to assess the effectiveness of treatments. Biopsy sampling should be repeated to confirm histologic remission (eosinophils < 15/HPF) after 6–12 weeks from the initial therapeutic interventions;2,29 this is because resolution of symptoms is not reliable in defining disease activity. 54 This finding has been recently confirmed in a multicenter study that showed a significant discrepancy between the presence of symptoms and endoscopic or histological response to drug therapy. 58 A diagnostic/therapeutic flow-chart has been reported in (Figure 1).
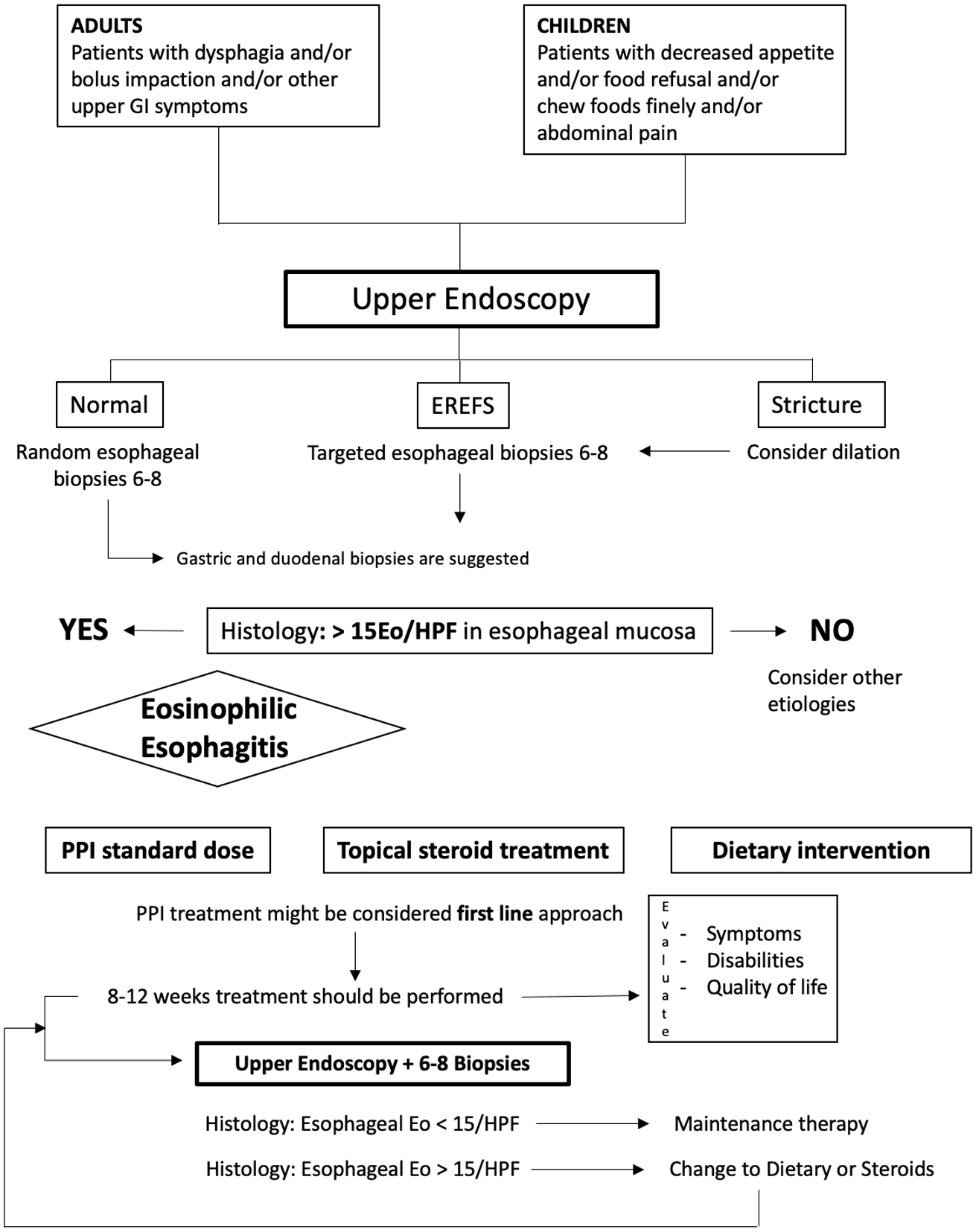
Diagnostic work-up and management of EoE patients.
Treatment endpoints and options
When treating patients with EoE, it is desirable to (i) induce and maintain remission of eosinophilic inflammation below 15 eosinophils/HPF (Table 4), (ii) control symptoms to improve quality of life and (iii) prevent and treat complications.
Efficacy of therapeutic interventions in EoE.

Data regarding the efficacy of topical steroids come from randomized placebo-controlled trials that differed in medication, dosages, administration methods, but with homogeneous cut-offs of <15eos/hpf indicating histologic remission.
One study, 17/18 patients achieved histological remission with elemental diet.
One study, 6/13 patients achieved histological remission with 4-FED.
One study, 9/15 patients achieved histological remission with 4-FED.
One study, 1/1 patient achieved histological remission with milk-free diet.
4-FED, Four Foods Elimination Diet; 6-FED, Six Foods Elimination Diet; CI, confidence interval; EoE, eosinophilic esophagitis; PPIs, proton pump inhibitors.
Therapeutic options include drugs [i.e. proton pump inhibitors (PPIs) and topical corticosteroids], dietary interventions and esophageal dilation. Any treatment may be offered as first-line and later be interchanged; 29 however, the choice should consider EoE phenotype (i.e. inflammatory versus fibrostenotic), patient’s clinical characteristics, preference and tolerance to treatment, as well as costs and available expertise.
Proton pump inhibitors
It has been widely recognized that GERD and EoE are distinct entities—possibly bidirectionally related—that may coexist.29,57,64 Reflux can be favored by the fibrosis-related esophageal dysfunction of EoE, and GERD could predispose to EoE by impairing mucosal integrity. 65 EoE patients seem to be more sensitive to acid, 66 although most patients benefit from PPI therapy even if no pathological reflux is detected. 67 This latter condition used to be called PPI-Responsive Esophageal Eosinophilia, but since 2017, it is considered a part of the EoE continuum, rather than a different disease. 29 PPIs have two main effects on EoE: the reduction of the acid refluxate favors the restoration of the mucosal barrier and limits environmental allergens exposure; 68 and PPIs reduce levels of eotaxin-3, a Th-2 cytokine involved in eosinophil-mediated inflammation. 69 However, the interplay between PPIs and EoE is likely to involve other more complex mechanisms as well. The role of acid burden in EoE is supported from the evidence that vonoprazan (a potassium-competitive acid blocker) induces histologic remission in PPI non-responder patients.70,71 Although still administered off-label, monotherapy with PPIs leads to clinical and histological remission in up to 50% of both pediatric and adult patients with EoE. 72 When treatment is discontinued, EoE recurs over a 3–6-month period.2,29 Of note, transient response to PPI therapy has been reported, with relapse of eosinophilic esophageal infiltrates during therapy. 73 Because of their effectiveness in inducing and maintaining remission and favorable safety profile, PPIs are usually recommended as the first choice for treatment in EoE.29,54 Doses of 20–40 mg omeprazole or equivalent PPI twice daily are adequate for adults, whereas children should receive 1–2 mg/kg daily. 29 It is suggested that such doses should be administered for 8 weeks to assess the response.2,54,74 PPIs seem effective in maintenance therapy; in a recent prospective multicenter study, 78.6% of pediatric patients maintained a clinicopathologic remission at 1-year follow-up on PPI standard doses of esomeprazole 1 mg/kg daily. 30 Similarly, it has been shown that 83% of adult patients could be kept in remission stepping down from 40 mg to 20 mg of esomeprazole once daily. 75 However, optimal dosages and duration have not been validated yet.
Corticosteroids
Corticosteroids (CS) represent a mainstay in the EoE therapy. Steroidal anti-inflammatory activity reduces esophageal fibrosis and remodeling and improves the integrity of the esophageal mucosal barrier. 76 Both systemic and topical steroids are effective in inducing histological remission in patients of all ages with EoE, 77 yet systemic administration causes non-negligible adverse effects (i.e. hyperphagia, weight gain, cushingoid features, adrenal suppression, growth retardation, osteopenia, osteoporosis, oral and esophageal candidiasis, glucose intolerance and cataract formation).16,29,77,78 In contrast, topical CS are not associated with relevant adverse events, except for esophageal candidiasis in 15% of patients29,77 which could be promptly treated with orally administered antifungals. For these reasons, topical steroid therapy is recommended, and systemic administration should be avoided. 29 Chemical formulations of topical CS include inhaled preparations (commercialized for the treatment of asthma), viscous suspensions, and effervescent tablets. Notably, topical CS are currently prescribed off-label, except for effervescent tablets of budesonide, which have been recently approved by the European Medicines Agency (EMA) for the treatment of EoE in adults. Regardless of the method of delivery, the administration of topical CS should take place after a meal, and patients should avoid eating or drinking the following 30–60 min to minimize esophageal drug clearance. 43 When taking inhaled preparations of steroids, patients should puff the medication into the mouth while holding the breath and then swallowing. 29 Since histologic improvement depends on the CS mucosal contact time, viscous topical formulations and orodispersible tablets are considered the optimal delivery methods.60,79 Regarding children, recent guidelines suggest fluticasone propionate (FP) dosages of 880–1760 mcg/day for induction and 440–880 mcg/day for maintenance, and the suggested budesonide dosages are 1–2 mg/day for induction and 1 mg/day for maintenance. 29 In adults, the suggested doses of FP are 1760 mcg/day for induction and 880–1760 mcg/day for maintenance. Regarding budesonide, a dose of 2–4 mg/day for induction and 2 mg/day during the maintenance period are considered adequate. Daily dosages of CS are usually administered in split doses. 29 Lower dosages of viscous budesonide (2 mg/day) or fluticasone (1600 mcg/day) have been recently proposed for induction. 80 It has been suggested that 3 months is an adequate timeframe to evaluate histologic response to induction with FP; 61 further, it has been shown that the effectiveness of swallowed FP at inducing remission in children was greater in nonallergic and younger individuals 81 and that higher levels of tryptase and eotaxin-3 were associated with steroid response (FP or budesonide). 82 Several systematic reviews and meta-analysis have confirmed the effectiveness of CS at improving esophageal eosinophilic inflammation both in children and adults;83–86 however, heterogeneity among studies in dosages, duration of treatments, administered steroids and methods of delivery, largely limit a comparative analysis. 29 Regarding the improvement of symptoms during CS treatment compared with placebo, studies have shown contrasting results.60,83,86
CS are effective in maintaining remission; this is also true because discontinuation of treatment generally leads to a relapse in a few weeks’ time.77,87 In a randomized double-blind placebo-controlled trial, histologic remission was maintained with 880 mc/day of FP in 73% of children who had undergone induction with 1760 mcg/day. 61 Similarly, in a randomized double-blind placebo-controlled trial in adults, remission was kept in 36% of patients who were taking 0.5 mg/day of budesonide suspension for 50 weeks. 31 Differences in maintaining remission between children and adults should be interpreted with caution because the mentioned data are not directly comparable.
Dietary interventions
Since food antigens are implicated in the pathogenesis of EoE,38,54 diet modification is the only therapeutic approach targeting the cause of the disease. Potentially, prolonged avoidance of trigger foods may lead to sustained clinical and histologic remission. 29 Strategies to individuate the culprit foods to induce and maintain remission include an elemental diet, an empiric elimination diet, and a food allergy testing-guided elimination diet. 88
Elemental diet
The elemental diet consists of liquid formulas containing single amino acids, carbohydrates and medium-chain fatty acids, 54 thus devoid of antigenic capacity. 88 Accordingly, such an approach has an impressive efficacy in both children and adults, leading to histologic remission in 90.8% [95% confidence interval (CI) 84.7–95.5%] patients. 63 Nevertheless, elemental diets have significant drawbacks that strongly limit clinical use. Patients should be on an exclusive elemental diet for 4–6 weeks, histologic remission should be confirmed on biopsy, and foods should subsequently be reintroduced every 5–7 days starting from the least allergenic to the most.43,89 If symptoms do not recur after reintroduction, an endoscopy should be performed to confirm histologic remission. 43 In contrast, if symptoms recur, the last introduced food should be eliminated from the diet and followed with the next challenge when the patient is symptom-free. 43 In addition to this remarkable procedural complexity, due to the poor palatability of elemental formulas, a nasogastric tube is often required in children. 88 Infants tolerate amino acid formulas better than older children; 90 however, there is the risk of delayed onset of oral motor-skills because facial muscles are not engaged in mastication. 91 Regarding adults, the need for strict avoidance of all kinds of table foods causes social, psychological and quality of life deterioration; 88 in addition, adults are likely to fail adhering to the diet in 2–4 weeks’ time. 92 Moreover, elemental formulas are expensive and not always covered by health systems. 93 Today, elemental diet should be considered an option in children with multiple food allergies and severe failure to thrive, in which a prompt remission is desirable. 90 However, because EoE has a chronic nature, exclusive elemental diet does not constitute a feasible nutritional alternative over a long period. 94
Target elimination diet
Target elimination diets are designed based on food allergy test results. Skin prick test (SPT) is used to study immediate IgE-mediated allergic reactions29,95 and atopy patch test (APT) is used to assess the presence of delayed non-IgE, cell-mediated reactions.29,96 When foods tested positive with SPT are excluded from the diet, the results are disappointing. A systematic review concluded that histologic remission is achieved in 45.5% of patients of all ages undergoing a target elemental diet. 63 Unfortunately, the reproducibility of such results was considered low in a recent meta-analysis, due to the wide heterogeneity of samples.63,88 However, children seem to respond more to target food elimination than adults (47.9% versus 32.2%) and show better outcomes when SPT and APT results are combined, with 78% patients achieving clinical and histological remission. 97 Discrepancies in response between children and adults may suggest a decreasing pathogenic role of IgE in favor of IgG4 in the transition from childhood to adulthood. 88 It is noteworthy that APT has not been validated in food allergies 29 and SPT results have an extremely low concordance with EoE food triggers when histology is monitored upon food reintroduction. 98 For these reasons, the accuracy of skin allergy tests is currently considered insufficient to guide food elimination from the diet, 29 although this point is still questionable for children.36,99,100
Empiric elimination diet
The empiric elimination diet is based on the elimination of the most common foods known to trigger EoE. After histological remission is achieved, individual foods should be introduced and an endoscopy with biopsy should be performed after 4–6 weeks for each food to confirm/exclude remission. 43 Three different empiric approaches have been developed over time: (i) In the Six-food elimination diet (6-FED) patients are instructed to avoid milk, wheat, egg, soy, nuts, and fish/shellfish. 101 6-FED is effective both in children and adults, with 72.1% of patients achieving clinical and histological remission. 63 Despite large food deprivation, the 6-FED has not been proven to cause nutrient deficiencies or growth deceleration in children. 102 Because the most common triggers in 6-FED responders were cow’s milk, wheat, egg and legumes, 29 (ii) the Four-food elimination diet (4-FED) excluding the named foods was developed. The 4-FED is more effective in children than adults (64% versus 54%) 88 and is less restrictive. (iii) The Two-food elimination diet (2-FED) was then designed based on the rationale that half of the 4-FED responders 88 and three-quarters of 6-FED responders 103 had only one or two trigger foods. In 2-FED, the alimentary restriction is limited to milk and gluten, 88 and this approach leads to remission in 43% of patients with no differences among ages, according to a recent study. 103 To reduce the high level of dietary restrictions and the large number of endoscopies required during elimination diets, it has been proposed to start with a 2-FED and step-up to a 4-FED and subsequently to a 6-FED on the basis of the response to restrictions. 103 Adopting the 2-4-6-FED step-up approach reduces the number of endoscopic procedures and diagnostic process time by 35% 29 and is effective; cumulative clinic-histologic remission ranges from 43% under 2-FED to 60% with 4-FED and achieves 79% when adopting a 6-FED. 103
Immunosuppressants and biologic agents
The introduction of biologic therapy has revolutionized the management of refractory allergic diseases such as asthma, atopic dermatitis, and nasal polyposis. Although the Th2 cytokine signature indicates an allergic etiology in EoE, the immunosuppressant and biologic agents are currently not recommended as the standard treatment of EoE. 29
Monoclonal antibodies targeting cell signaling proteins implicated in the Th2-predominant inflammation, like interleukin (IL)-5, -4, and -13, are being investigated.
IL-5 has been recognized as a potential therapeutic target because it supports the growth and differentiation of activated B cells; in addition, its overexpression significantly increases eosinophil numbers and antibody levels predominantly from an expanded population of B-1 cells in vivo. 104
Mepolizumab, a humanized anti-IL-5 monoclonal IgG1 antibody, was first assessed in an open-label study of adults with longstanding, symptomatic EoE (four cases). Following three infusions of intravenous mepolizumab 10 mg/kg, all patients demonstrated clinical response at week 4. 105 Although a substantial decrease in eosinophils in esophageal mucosa was observed, the peak counts did not reach the goal of <15 eosinophils/HPF. An RCT, conducted by Straumann et al., 106 compared 4 weeks of mepolizumab (750 mg/week for two doses, followed by 1500 mg/week for two doses if remission was not achieved) with placebo (phase II RCT), observing a poor clinical and histological improvement. Similar results were obtained in a phase II RCT in the pediatric population tested with reslizumab, another neutralizing antibody against IL-5. 107 Due to these results, reslizumab was not found to be effective for the induction of clinical response in patients with EoE. Targeting the IL-5 pathway by the administration of benralizumab, an antibody that blocks the IL-5 receptor alpha, is a highly effective therapy for asthma; it recently received the approval of the Food and Drug Administration and EMA as add-on maintenance therapy for children (>12 years) and adults with severe eosinophilic asthma, and an RCT in patients with eosinophilic gastritis is currently ongoing (NCT03473977).
IL-13 secreted by Th2 cells and activated eosinophils play a vital role in the pathogenesis of EoE by increasing eotaxin-3 and promoting fibroblasts production of periostin, which increases eosinophil chemotaxis. 108 IL-13 seems to affect esophageal mucosal integrity, playing a crucial role in dysregulating membrane cytoskeletal proteins. 109
Dupilumab, a human monoclonal antibody against the IL-4 receptor alpha, inhibits IL-4 and IL-13 signaling. Dupilumab is effective in the treatment of allergic, atopic, and type 2-mediated inflammatory diseases.110–112
Dupilumab has been studied in a phase II trial of 47 patients who received subcutaneous dupilumab 300 mg or placebo for 12 weeks (NCT02379052). Clinical response, as measured by the Straumann Dysphagia Index, significantly improved after 10 weeks of treatment compared with placebo (45 versus 19%, p = 0.0304). Moreover, the peak eosinophil count significantly reduced in the dupilumab arm (92 versus 15%, p < 0.0001). 113 Considering these promising results, a phase III trial was initiated to determine the efficacy and safety of dupilumab in adult EoE patients and is currently recruiting (NCT03633617).
Also, mast cells are key players in EoE pathogenesis. 2 Omalizumab is a humanized monoclonal anti-IgE antibody that binds to IgE and hence prevents activation of mast cells. 114 In a prospective, randomized, double-blind, placebo-controlled trial of adults with EoE, omalizumab (0.016 mg/kg/IgE) (n = 16) or placebo (n = 14) were administrated subcutaneously every 2–4 weeks for 16 weeks. 115 Treated subjects had no significant reduction both in esophageal eosinophil and symptoms perception compared with controls. However, mast cells decreased after treatment with omalizumab.
As reported in this section, monoclonal antibodies have been proposed to overcome the currently unmet medical needs of patients with EoE. Most new drugs are imported from other Th2-mediated allergic diseases and are being suggested as potential modifiers of the disease’s natural history; however, data in this field are still scant.
Endoscopic dilation (ED)
Endoscopic balloon dilation or bougienage are the options currently available for the treatment of dysphagia associated with fibrostenotic complications in patients with EoE. Rings, strictures, and a narrowed esophageal caliber are significantly more common in adults than children,2,3 as they are present in 30–80% of adults with EoE. 116 Nevertheless, dilation may be offered in association with medical therapy (i.e. diet and CS) in children with severe dysphagia. 117 Although having no influence on esophageal inflammation, 118 a recent meta-analysis showed that a median of three dilations was effective and offered sustained symptoms relief in 95% patients of all ages undergoing the procedure for strictures or narrowed esophageal caliber. 119 In addition, the ED is a safe procedure. The same study showed that the rate of major complications after 1820 dilations was below 1% and that no deaths occurred; 119 further, the rate of perforations after ED was around 0.3%, 119 as in patients without EoE undergoing dilation. 120 However, 75% of patients experience chest pain that may last for days after the procedure, thus, patients should be forewarned. 118 It is suggested that dilation should be gradually performed over several sessions separated by 3–4 weeks and that the progression of dilation should be limited to 3 mm per session. 121 Deep mucosal lacerations following the procedure should not be regarded as complications; rather they are the intended outcome. 29 ED should be performed when symptoms persist despite medical or dietary therapy.2,29,54,122 However, when a severe stricture is encountered on an initial endoscopy or food impaction has occurred, the dilation could be performed as a first-line therapeutic approach. 54
Summary and conclusion
It is estimated that the mean diagnostic delay of EoE is 4–6 years both in children and adults2,45 and this is probably because initial manifestations of the disease may be overlooked. Early detection depends on the recognition of age-dependent characteristics that can also influence treatment. We have reviewed epidemiologic, clinical, endoscopic, and histologic features and therapeutic options of EoE, pointing out differences and similarities between children and adults to help guide clinical practice.
To summarize, early detection in children may be hampered by inadequate communicative skills, thus EoE should always be investigated in those with aspecific gastrointestinal symptoms. 32 In older adolescents and adults, dysphagia to solids, food impaction, and heartburn are the most common symptoms. 30 Allergic diathesis supports clinical suspicion. An EGD with biopsies should be performed as the first step. 4 On endoscopy, children have an inflammatory-predominant pattern, while adults usually have a fibrostenotic pattern. 42 Since EoE has a patchy nature, 52 at least six esophageal biopsies should be collected, selecting areas of mucosal abnormalities.29,53 In those with normal endoscopic appearance and typical symptoms, random biopsy sampling is warranted.17,42,49 Eosinophilic gastroenteritis should always be ruled out.29,54
Therapeutic interventions should aim to induce histologic remission, relieve symptoms, and prevent or treat complications. Drugs, dietary regimens, and EDs may be offered as first-line treatments, and are interchangeable over time and could be combined. 29
Off-label use of PPIs is effective in inducing and maintaining remission.29,54 Topical corticosteroids reduce esophageal inflammation and remodeling; 76 however, data on their clinical efficacy are conflicting.60,83,86 Long-term adverse effects and optimal maintenance dosages have not been assessed yet; however, dose reduction demonstrated efficacy both in children and adults, and adverse events are usually mild.29,31,61,77 Unlike drugs, dietary restrictions represent effective nonpharmacological therapy, practically devoid of adverse effects. Diets with amino-acidic formulas are effective both in children and adults, 63 but the clinical application is hampered by procedural complexities, costs, and scarce compliance. 92 The target elimination diet is poorly effective and not recommended in EoE. 29 A 2-4-6 FED step-up approach may have better chances of clinical application, being less restrictive. Symptoms do not always improve hand in hand with mucosal healing, 123 and anti-inflammatory or dietary therapy may not be effective when strictures or fixed rings develop; in such cases, EDs represent an effective treatment.29,92,118,122
In conclusion, EoE is an emerging disorder whose diagnosis is often delayed. Early detection may lead to anticipating treatment and preventing the disorder, or at least decelerating the development of complications. Treatment options and endpoints should be tailored individually to achieve lasting compliance. This is crucial because EoE is a chronic disease that almost invariably relapses when the treatment is withdrawn.
Footnotes
Authors’ contribution
Pierfrancesco Visaggi, Teresa Di Chio, Giusi Sciume, Francesco Bronzini: Formal analysis, writing – original draft, writing – review and editing.
Salvatore Tolone, Marzio Frazzoni, Lorenzo Bertani: Data curation, formal analysis, visualization, writing – original draft, writing – review and editing.
Matteo Ghisa, Camilla Pugno: Data curation, formal analysis, visualization.
Santino Marchi, Vincenzo Savarino, Diego Peroni, Massimo Bellini: review and editing.
Nicola de Bortoli, Edoardo V Savarino: Conceptualization, formal analysis, methodology, supervision, writing – original draft, writing – review and editing.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Guarantor of the article
Nicola de Bortoli