
Abstract
Background:
Community-acquired pneumonia is among the most common infections affecting ulcerative colitis and Crohn’s disease patients. Data regarding epidemiology and outcomes of pneumonia in inflammatory bowel disease patients is lacking. We aimed to identify predictors of adverse outcomes among inflammatory bowel disease patients treated for pneumonia.
Methods:
This was a retrospective cohort study that included adult patients admitted to Sheba Medical Center for pneumonia between 2012 and 2018. Data was collected from an electronic repository of all emergency department admissions and included tabular demographic and clinical variables and free-text physician records. Pneumonia cases were extracted using the International Classification of Diseases (ICD-10) coding.
Results:
Of 16,732 admissions with pneumonia, 97 were inflammatory bowel disease patients (45 Crohn’s disease; 52 ulcerative colitis). We found a similar rate of 30-day mortality among inflammatory bowel disease and non-inflammatory bowel disease patients (12.1% versus 11.3%, p = 0.824) and between Crohn’s disease and ulcerative colitis patients (11.1% versus 11.5%, p = 0.947). There was an increased hospitalization rate among inflammatory bowel disease patients (92.8% versus 85.6%, p = 0.045), but similar hospitalization duration (4 versus 4 days, p = 0.384). Crohn’s disease patients had a shorter hospitalization duration compared with ulcerative colitis patients (3 versus 5.5 days, p = 0.029). Bronchiectasis (adjusted odds ratio 60.95, 95% confidence interval 2.72–1364.39, p = 0.01) and opioids use (adjusted odds ratio 13.21, 95% confidence interval 1.29–135.18, p = 0.03) were associated with an increased 30-day mortality rate in inflammatory bowel disease patients.
Conclusion:
This is the first study to identify predictors of mortality in inflammatory bowel disease patients with pneumonia. The rate of mortality and hospitalization duration of stay were similar among inflammatory bowel disease and non-inflammatory bowel disease patients. Use of opioids and presence of bronchiectasis were associated with a higher risk of mortality in inflammatory bowel disease patients with pneumonia.
Keywords
Introduction
The incidence and prevalence of inflammatory bowel disease (IBD) is increasing worldwide, 1 especially in newly industrialized countries. 2 In western countries the incidence of IBD is stable and even falling, and the prevalence is estimated at 0.3%. 2 Though IBD patients should not be routinely considered immunocompromised, 3 they are at increased risk for infectious complications. Because of the chronic nature of the disease, most of the patients require long-term therapy including corticosteroids, immunomodulators or other biologicals. Hence, they are at increased risk for infections.3–7 In addition, based on genome wide association studies, the innate immune system might be impaired in IBD patients. 3 Community acquired pneumonia (CAP) is the second most common cause of hospitalization and the most common infectious cause of death in United states.8,9 CAP is among the top three infectious diseases affecting IBD patients 7 and accounts for significant morbidity and mortality. Previous studies found that IBD patients have a higher risk for complications following bacterial pneumonia 5 including Hemophilus influenzae pneumonia, and also following influenza virus pneumonia.6,10 Older age, chronic obstructive lung disorder, proton pump inhibitors (PPIs) use, corticosteroids use and tumor necrosis factor alpha inhibitors use are known to be associated with increased risk for pneumonia among IBD patients.5,6,11 A recent United States nationwide cohort found that elderly IBD patients with pneumonia have an increased hospitalization rate. 12 To date, no study has described and evaluated the outcomes of pneumonia among IBD patients. We investigated the epidemiology, natural history and predictors of adverse outcomes in IBD patients treated for pneumonia.
Materials and methods
Study design and patient selection
This was a retrospective, data-based cohort study that included adult patients admitted to Sheba Medical Center for pneumonia between 2012 and 2018. Data was collected from an electronic repository of all emergency department admissions and included tabular demographic and clinical variables and free-text physician records. The cohort consisted of IBD patients and non-IBD patients. Patients under 18-years-old were excluded. Moreover, for each patient, only the first admission during that period of time was taken into account, while other additional admissions were excluded. IBD and pneumonia cases were extracted using the International Classification of Diseases (ICD-10) coding.
Data extraction
The following data was collected from the electronic health record of Sheba Medical Center:
Demographic factors – age (years), sex.
Background chronic medications – antiplatelet drugs, anticoagulants, anti-hypertensive medications, β-blocking agents, insulin and oral blood glucose-lowering medications, HMG-CoA reductase inhibitors, opioids, PPIs, benzodiazepine-derivative medications.
Disease characteristics (disease activity, extent of disease, history of IBD surgeries). Disease activity status was extracted from free text summaries following gastroenterologist visits. As many of the included patients are not actively followed in our center and were only hospitalized for pneumonia, disease characteristics were available only partially.
IBD-related medications – amino salicylic acid and similar agents (5-ASA), corticosteroids, immunomodulators such as azathioprine, mercaptopurine and methotrexate. Biologicals including tumor necrosis factor alpha inhibitors and anti-adhesion medications such as vedolizumab.
Comorbidities – congestive heart failure, ischemic heart disease, hypertension, diabetes, smoking, alcohol abuse, gastroesophageal reflux disorder, bronchiectasis, chronic obstructive pulmonary disorder, asthma and cerebrovascular ischemic disease.
Outcomes
Primary outcome – mortality within 30 days.
Secondary outcomes – hospitalization rate, hospitalization duration and recurrence of pneumonia within 1 year.
Data analysis and statistical methods
Patients’ characteristics are presented as median and interquartile range (IQR) for continuous variables, while categorical variables are expressed as proportions. Outcome comparisons between IBD patients and non-IBD patients, and between Crohn’s disease (CD) patients and ulcerative colitis (UC) patients were performed using two-tailed Student’s t-test for continuous variables. Chi-squared test was used for categorical variables. For each demographic factor, background disease and medication, we conducted univariate analyses related to 30-day mortality rate. We then constructed a model by logistic regression analysis composed of the highly associated variables to 30-day mortality outcome. A value of p ⩽ 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics (IBM, Armonk, NY, USA).
Study ethics and patient consent
This study was carried out in accordance with the ethical guidelines of the Declaration of Helsinki. The study was approved by the Sheba Medical Center ethics committee. Approval was granted for Helsinki protocol 4530 on 28 April 2019. Since this was a retrospective analysis, no informed consent was obtained.
Results
Patient characteristics
Our cohort consisted of 25,254 admissions to Sheba Medical Center for pneumonia between 1 January 2012 and 31 December 2018. Of them, 16,732 admissions met the inclusion criteria. There were 97 IBD patients. Among them, 45 were CD patients and 52 were UC patients. To mention, there were 997,873 admissions to Sheba Medical Center in that period, of them 800,904 non-IBD patients and 6599 IBD patients 18-years-old or older. Pneumonia accounted for 2.1% and 1.5% of these admissions for non-IBD patients and IBD patients, respectively (p-value = 0.001). (Figure 1).

Study flow chart.
Baseline characteristics of IBD and non-IBD patients are presented in Table 1. IBD patients were younger than non-IBD patients [72 (53.5–83.0) versus 75 (60.0–85.0) years (IQR), p = 0.25], but it was not significant. No significant difference in gender proportions between the groups was observed. Comorbidities such as diabetes (16.5% versus 22.8%, p = 0.142), hypertension (30.9% versus 41.4%, p = 0.037) and congestive heart failure (15.5% versus 19.2%, p = 0.350) were more prevalent among non-IBD patients (Figure 2), and some of these were statistically significant. The IBD group had a higher prevalence of bronchiectasis compared with the non-IBD group (3% versus 1%, p < 0.001). As excepted, use of immunosuppressant and biological medications was more common among IBD patients [corticosteroids (19.6% versus 9.7%, p = 0.010), azathioprine (5.2% versus 0.4%, p < 0.001) mercaptopurine (4.1% versus 0%, p < 0.001), methotrexate (3.1% versus 0.7%, p = 0.004), vedolizumab (2.1% versus 0%, p < 0.001), tumor necrosis factor alpha inhibitors (6.2% versus 0%, p < 0.001)]. Characteristics of CD and UC patients are shown in Table 2. CD patients were younger than UC patients [60 (37–76) versus 78.5 (70.25–85) years, p = 0.006]. Except for the higher rate of diabetes among UC patients (4% versus 26%, p = 0.03) no significant difference in background comorbidities was observed between the groups. Use of 5-ASA was more prevalent among the UC group (37% versus 61%, p = 0.02), while tumor necrosis factor alpha inhibitors were used only by CD patients (13% versus 0%, p < 0.01).
Baseline characteristics: IBD patients versus non-IBD patients.

CVA, cerebrovascular accident; IBD, inflammatory bowel disease; IQR, interquartile range

Background comorbidities: IBD patients versus non-IBD patients.
Baseline characteristics: Crohn’s disease patients versus ulcerative colitis patients.

CD, Crohn’s disease; CVA, cerebrovascular accident; IBD, inflammatory bowel disease; IQR, interquartile range; UC, ulcerative colitis
Outcomes
Primary and secondary outcomes are summarized in Table 3 (IBD versus non-IBD group) and Table 4 (CD group compared with UC group). IBD patients had a higher hospitalization rate than non-IBD patients (92.8% versus 85.6%, p = 0.045), while hospitalization duration [4 (3–7) days versus 4 (2–7) days (IQR), p = 0.384] did not statistically differ among the two groups. IBD patients had a similar 30-day mortality rate compared with non-IBD patients (12.1% and 11.3%, p = 0.824). CD and UC patients demonstrated the same rate of 30-day mortality rate (~11%) and hospitalization rate (~93%). CD patients had a shorter hospitalization duration [3 (2.0–5.25) versus 5.5 (3–9.75) days, p = 0.029] compared with UC patients.
Pneumonia outcomes: IBD patients versus non-IBD patients.
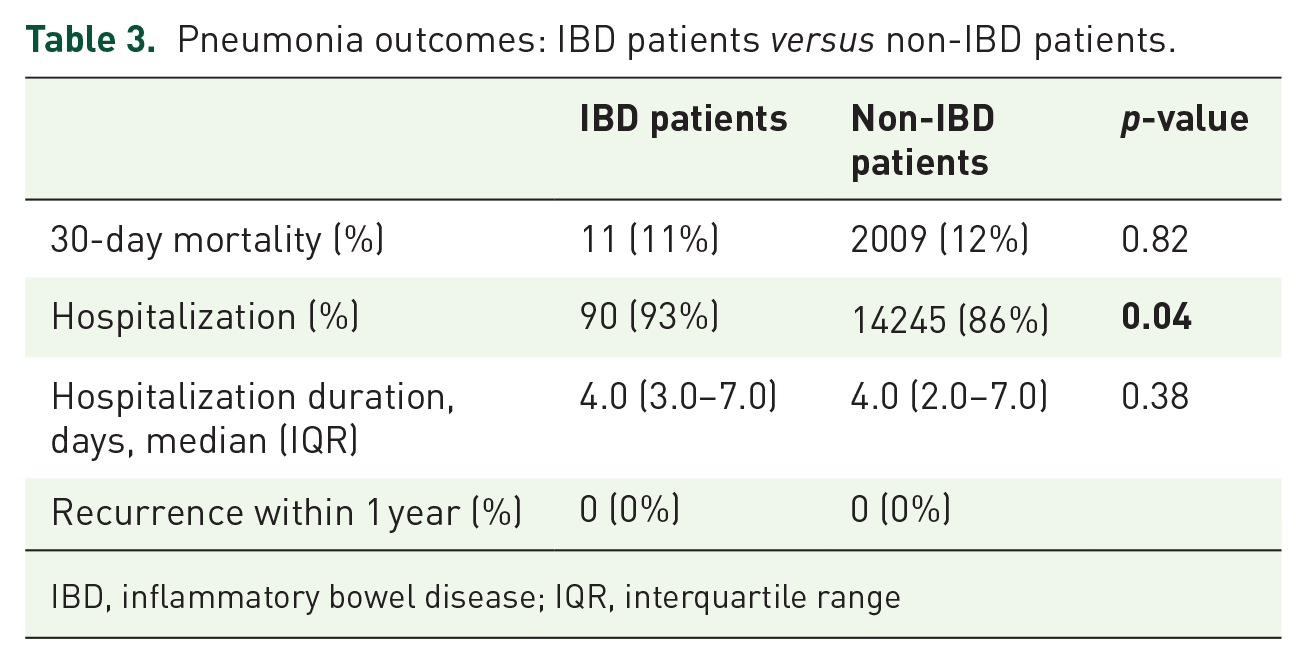
IBD, inflammatory bowel disease; IQR, interquartile range
Pneumonia outcomes: Crohn’s disease patients versus ulcerative colitis patients.

CD, Crohn’s disease; IQR, interquartile range; UC, ulcerative colitis
Predictors of mortality
Table 5 shows results of univariate analyses related to 30-day mortality rate including various demographic and clinical factors. We found bronchiectasis [odds ratio (OR) 18.88, 95% confidence interval (CI) 1.55–229.38, p = 0.02] to be significantly associated with the risk of 30-day mortality in IBD patients. Univariate analysis also demonstrated that history of IBD abdominal surgery was associated with increased risk of 30-day mortality (OR 4.18, 95% CI 0.94–18.56, p = 0.04). On the other hand, neither chronic obstructive pulmonary disorder (OR 2.96, 95% CI 0.51–16.92, p = 0.20) nor asthma (OR 0.88, 95% CI 0.81–0.94, p = 0.41) has been found to significantly correlate with increased rate of 30-day mortality. In addition, use of PPIs (OR 4.28, 95% CI 1.06–17.30, p = 0.03), opioids (OR 6.07, 95% CI 1.22–30.24, p = 0.01) and benzodiazepines (OR 4.67, 95% CI 1.24–17.61, p = 0.01) was highly associated with increased 30-day mortality rate. Neither immunosuppressants nor biological agents were found to affect 30-day mortality rate among IBD patients (Table 5). Pulmonary embolism, deep venous thrombosis episodes or anticoagulants prophylaxis during hospitalization were not associated with the risk of 30-day mortality (Table 5).
Univariate analyses: odds ratio for 30-day mortality rate in IBD patients treated for pneumonia.

Data was missing for five patients.
Data was missing for six patients.
CI, confidence interval; CVA, cerebrovascular accident; DVT, deep venous thrombosis; Hx, hospitalization; IBD, inflammatory bowel disease; PE, pulmonary embolism
The multivariate logistic regression analysis is shown in Table 6. Bronchiectasis [adjusted OR (AOR) 60.95, 95% CI 2.72–1364.39, p = 0.01] and opioids use (AOR 13.21, 95% CI 1.29–135.18, p = 0.03) were independently associated with the risk of 30-day mortality in IBD patients.
Multivariate analysis model: adjusted odds ratio for 30-day mortality rate in IBD patients treated for pneumonia.

CI, confidence interval; IBD, inflammatory bowel disease
Discussion
In this large tertial center cohort, we examined the risk factors for mortality from pneumonia in IBD patients. We found 30-day mortality rate and hospitalization duration to be comparable between IBD and non-IBD patients, while hospitalization rate was higher among IBD patients. Bronchiectasis and opioids use were associated with increased risk of mortality in IBD patients treated for pneumonia. To the best of our knowledge, this is the first study to identify predictors of mortality in IBD patients with pneumonia.
The incidence of respiratory manifestations in IBD patients is underestimated, 13 first described by Kraft et al. 14 in 1976, and its prevalence was estimated to be as high as 0.21%. Bronchiectasis is one of the most common respiratory disorders in IBD patients; its frequency ranges from 18% to 26% and it may precede or follow disease diagnosis.15,16 In our cohort three IBD patients had bronchiectasis (3%), and there were two CD patients and one UC patient. Exacerbations are usually caused by acute bacterial infections,17,18 thus, the importance of vaccinations regimen adherence cannot be overemphasized. Furthermore, bronchiectasis might be complicated by life threatening massive hemoptysis, a medical condition which may require prompt diagnostic and therapeutic procedures. 19 Therefore, gastroenterologists should be aware of the harmful effects of respiratory involvement in IBD patients, particularly bronchiectasis, although it is relatively rare. Pulmonologist consultation should be promoted early in selected patients and management should be tailored for each patient. This is well highlighted by our findings.
Pain management is a well-known challenge in treating IBD patients. While commonly used pain-killers such as non-steroidal anti-inflammatory drugs may cause a disease exacerbation, 20 narcotics (e.g. opiates) use is very prevalent in alleviating disease symptoms.20–22 Opiates prescription is increasing worldwide among patients with chronic non-cancer pain, including IBD patients. 21 In the largest population-based study of opiate use among IBD patients, by Burr et al., 30% of the patients were prescribed an opiate agent during a period of 3 years. 21 Notably, Gao et al. showed that most IBD patients use opiates. 20 IBD patients with poor quality of life are more likely to use opioids. 22 Our study demonstrated an increased odds ratio for 30-day mortality among IBD patients treated for pneumonia (AOR 13.21, 95% CI 1.29–135.18, p = 0.03). Some of the physiologic effects of opiates are reduced cough reflex, slow and shallow respirations and impaired secretions clearance,23–25 all of which may contribute to development of pneumonia. In addition, some opiate agents are known to impair the innate and adaptive immune systems, weakening the defense system against causative pathogens. 25 Burr et al. found that heavy use of strong opiates among IBD patients is associated with increased all-cause mortality. 21 In addition, it was observed that opiates use among community dwellers with Alzheimer’s disease was associated with a 34% increased risk of hospital treated pneumonia compared with non-users. 24 A recently published large cohort study of 25,392 participants demonstrated a strong, independent association between prescribed opioids and the risk of CAP requiring hospitalization. 25 Furthermore, a dose-dependent effect of this association has been demonstrated.24,25 Thus, it is crucial to consider the harmful effects of opiates when prescribing these agents, and to reduce their use as much as possible.
We did not find a significant association between immunosuppressants use (particularly corticosteroids) and 30-day mortality rate. It was true also for other immunomodulators and biological agents (Table 5). Multiple multivariate models composed of different combinations of incorporated covariates resulted in similar findings. Our results are in contrast with previous studies that demonstrated increased risk of pneumonia among IBD patients using corticosteroids, biologicals5,11 or thiopurines. 11 A possible explanation for this may be a modest sample size; otherwise it is plausible that other systemic risk factors (use of opioids and presence of bronchiectasis) had a more significant impact on the prognosis.
IBD patients had a higher rate of hospitalization compared with non-IBD patients (93% versus 85%, p = 0.04). This finding is consistent with previously published studies that show increased risk for hospitalization with H. influenzae pneumonia 6 and with other causes of pneumonia among IBD patients.7,10 Though we have not addressed disease severity among both populations, based on the similar outcomes of 30-day mortality rate and hospitalization duration (Table 3), we can conclude that pneumonia severity was similar among the groups. Thus, the decision to hospitalize IBD patients might be influenced and biased by the stigma of the complicated and immunocompromised patients. In contrast to a previous study published by Ananthakrishnan et al., 7 in which increased rate of mortality was observed among IBD patients treated for pneumonia, no increased 30-day mortality rate among IBD patients was demonstrated in our study. It might be explained by the positive shift of vaccinations adherence as mentioned previously.6,26 Also, neither Ananthakrishnan et al. nor our study included any information about the natural history and severity of the disease among the study population. Moreover, the outcomes of pneumonia might be influenced by the causative pathogen (e.g. bacterial versus viral). Future studies which will take into account disease severity and ideally the causative pathogen have to be conducted to better estimate pneumonia outcomes among IBD patients.
No difference in 30-day mortality rate was observed between CD and UC populations, though CD patients were younger than UC patients (Table 2). The age difference may have been balanced by the prevalent use of biologicals among CD group compared with UC group and the adverse events involved with it. Also, important information about disease severity among the study population was lacking. Increased hospitalization duration for UC patients compared with CD patients (5.5 versus 3 days, p = 0.029) is consistent with the older UC population and the higher rate of comorbidities such as hypertension, ischemic heart disease, congestive heart failure and diabetes among UC group (Table 2). All of these might result in a more complex hospitalization course.
Our study has some limitations. First, pneumonia cases were extracted using the ICD-10 coding system based on the electronic records. Errors during diagnosis typing might result in contamination of study population with other diseases (e.g. patients who were admitted for bronchiectasis exacerbation may have wrongly been diagnosed with pneumonia). Second, similar to previous studies in IBD patients treated for pneumonia, information about pneumonia severity was lacking in our study. Hence, reliable comparison between studies’ outcomes was very difficult to achieve. In addition, our IBD patient cohort was relatively small. A larger sample size may have allowed us to better estimate predictors of mortality of pneumonia in IBD patients by incorporating more variables into the final multivariate model. Finally, we had limited data on baseline IBD characteristics in this patient cohort, as many of the included patients are not actively followed for their IBD in our center.
There are also several strengths in our study. First, this was a large cohort composed of patients treated for pneumonia from a single tertiary medical center. Second, we collected heterogeneous baseline characteristics for each patient such as demographic features, comorbidities and a broad list of medications. This enabled us to conduct multiple analyses to examine different associations between the aforementioned factors and disease outcomes.
In conclusion, this is the first study to identify predictors of mortality in IBD patients treated for pneumonia. We found that presence of bronchiectasis and opioids use were associated with increased risk of mortality in IBD patients treated for pneumonia. No association between immunosuppressants, immunomodulators or biological agents and 30-day mortality rate was observed. Our findings highlight the need of the primary care physicians and gastroenterologists to be aware of the possible harmful effects associated with opioids use. Also, they should be familiar with the pulmonary manifestations of IBD patients, including bronchiectasis. Vaccination regimen adherence cannot be overemphasized in order to prevent initiation and exacerbations of this medical condition.
Footnotes
Author contribution
The following author contributions were made: OU and UK – conceived the study; OU, UK, EK and YB – data acquisition and analysis; OU drafted the manuscript. All others participated in data interpretation and in critical revision of the manuscript for important intellectual property. All authors have approved the final draft submitted.
Conflict of interest statement
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UK: speaker and advisory fees – Abbvie, Jannsen Takeda Medtronic; research support – Jannsen Takeda Medtronic. SBH: consulting and advisory board fees and/or research support – Abbvie, MSD, Janssen, Takeda, and CellTrion. BU: consultation fees – Takeda, Neopharm, Janssen and Abbvie. The remaining authors declare that there is no conflict of interest.
Ethics statement
This study was carried out in accordance with the ethical guidelines of the Declaration of Helsinki. The study was approved by the Sheba Medical Center ethics committee. Approval was granted for Helsinki protocol 4530 on 28 April 2019.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Since this was a retrospective analysis, no informed consent was obtained.