
Abstract
Disability is a common worldwide health challenge and it has been increasing over the past 3 decades. The treatment paradigm has changed dramatically in inflammatory bowel diseases (IBDs) from control of symptoms towards full control of disease (clinical and endoscopic remission) with the goal of preventing organ damage and disability. These aims are broadly similar to rheumatoid arthritis and multiple sclerosis.
Since the 1990s, our attention has focused on quality of life in IBD, which is a subjective measure. However, as an objective end-point in clinical trials and population studies, measures of disability in IBD have been proposed. Disability is defined as ‘…any restriction or lack (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being.’ Recently, after 10 years of an international collaborative effort with the World Health Organization (WHO), a disability index was developed and validated. This index ideally would assist with the assessment of disease progression in IBD.
In this review, we will provide the evidence to support the use of disability in IBD patients, including experience from rheumatoid arthritis and multiple sclerosis. New treatment strategies, and validation studies that have underpinned the interest and quantification of disability in IBD, will be discussed.
Keywords
Introduction
Worldwide evidence regarding levels and trends in disease and injury incidence, prevalence and years lived with disability (YLD) is an essential component to predict and develop global, regional, and national health policies. The Global Disease Study 2013 estimates were made to quantify disability across acute and chronic diseases, and injuries for 188 countries between 1990–2013. 1 In this landmark study, disease and injury are highly prevalent across these time periods. In the years studied, comorbidity rose substantially with age and in absolute terms from 1990–2013. In addition, significant subsequent chronic sequelae were largely attributable to noncommunicable diseases. Overall, the proportion of disability-adjusted life years due to YLDs increased globally from 21% in 1990 to 31% in 2013. 1
The treatment paradigm has changed dramatically in inflammatory bowel disease (IBD) from control of symptoms towards full control of disease (clinical and endoscopic remission) with the ultimate target of terminating disease progression and thereby preventing bowel damage and subsequent disability. The World Health Organization (WHO) has previously approved the International Classification of Functioning, Disability and Health (ICF) which is a common conceptual framework that describes and measures the dimensions of human functioning, disability and health. The WHO defines disability as ‘…any restriction or lack (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being.’ 2
IBD is known to affect physical, psychological, familial and social dimensions of life.3,4 The psychological impact of IBD may also contribute to disability.3–5 Previously, until 2010, the major focus of disease impact in IBD was on quality of life, measured by the IBDQ (IBD Questionnaire), SIBDQ (short IBD Questionnaire) and the generic SF-36. 6 However, in more recent years, more objective measures of disability have been considered.
We have learned from rheumatoid arthritis (RA) and multiple sclerosis (MS) that disability can be prevented by disease-modifying agents, whereas such evidence is lacking in IBD. Now that a validated disability index is available, ongoing and upcoming clinical studies will explore whether disability can also be prevented in IBD patients. In this review, we will discuss disability in other inflammatory conditions and IBD, and what treatments may potentially impact favorably on this outcome.
Review criteria
An electronic search of publications in English on PubMed up to June 2017 was performed using the following keywords: ‘Crohn’s disease’, ‘ulcerative colitis’; ‘inflammatory bowel disease’, ‘treatment’, ‘functioning’; ‘disability’; ‘treat to target’; ‘early disease’; ‘rheumatoid arthritis’; ‘multiple sclerosis’. Also, a hand search of abstracts from the annual meetings of Digestive Disease Week and United European Gastroenterology Week, the European League Against Rheumatism Conference and the European Committee for Treatment and Research in Multiple Sclerosis Congresses between 2011 and 2016/7 was performed. Clinical trials status was checked on: http://www.clinicatrials.gov and http://www.clinicaltrialsregister.eu.
Why is inflammatory bowel disease a disabling condition?
IBD is known to significantly reduce the health-related quality of life (HRQOL) of patients. HRQOL is a quantitative measurement of subjective perception of health state. 7 Many previous studies and disease-specific questionnaires primarily focused on the Inflammatory Bowel Disease Questionnaire (IBDQ). 6 However, this is subjective and as it was not developed and validated according to the US Food and Drug Administration (FDA) guidance for the development of patient-reported outcomes, 8 it has consequences for future new drug approval in IBD.
Fatigue is a commonly reported symptom in IBD and has been shown to negatively impact the HRQOL in these patients.9–13
Pain has also been shown as prevalent in IBD patients during disease flares and also with extraintestinal manifestations of the disease.14–17 Many chronic conditions are known to lead to chronic pain which thereby impacts on HRQOL,18–21 which is also observed in IBD.3,22 A large proportion of IBD patients require opioid analgesia. 23 Patients with IBD also experience frequent concomitant anxiety and depression, 5 and some studies have reported that patients with Crohn’s disease (CD) have higher rates of anxiety and depression, than ulcerative colitis (UC) patients.10,24 There also appears a need to compare HRQOL indices in order to compare disease burden and impact across various disease states.3,8,25–27 These data have a high impact with regards future governmental health resource allocation.
With regards work disability in IBD a Swiss cohort study identified certain factors which contributed to this temporarily and permanently. In patients with CD, temporary work disability was associated with gender, disease duration, disease activity, C-reactive protein level, smoking, depressive symptoms, fistulas, extraintestinal manifestations and the use of steroids/immunosuppressants. In patients with UC, temporary work disability was associated with age, disease duration, disease activity, and the use of steroids/antibiotics. Overall, in this cohort study in all patients with IBD, permanent work disability was only associated with disease activity. 28
In another cohort study from the IBSEN group, patients with IBD had an more of a relative risk (RR) for requiring a disability pension than the ‘normal’ population in the 10 years after disease onset (RR: 1.8 and 2.0, for UC and CD, respectively). 29 Accordingly, the impact of IBD on social and professional life was included in the recently developed IBD disease severity index. 27
Overall, disability is high in both CD and UC and contributes to disease burden in IBD, but a validated tool to objectively measure this was lacking.
Development and validation of the inflammatory bowel disease disability index: a World Health Organization initiative
The International Classification of Functioning, Disability and Health (ICF) is a common conceptual framework which describes and measures the dimensions of human functioning, disability and health that was approved by the WHO in 2001.30,31 The ICF framework of classifying function and disability is multidimensional and includes factors that affect functioning, such as personal and environmental factors. IBD is known to affect physical, psychological, familial and social dimensions of life.3,4
In an attempt to quantify disability, the ‘IBD Disability Index’ (IBD-DI) (Table 1) was developed in collaboration with the WHO.32,33 This international collaboration was commenced in 2007 and the IBD-DI has recently been validated in a French population-based study. 33 The IBD-DI demonstrated high internal consistency, interobserver reliability and construct validity, and moderate intraobserver reliability. It comprises 14 questions, with scores ranging from 0–100. In this study, 150 patients with CD and 50 patients with UC completed the IBD-DI validation phase. IBD-DI scores were highly correlated with the IBDQ (–0.82; p < 0.001) and SF-36 (–0.61; p < 0.05) scores. Female gender (p < 0.001), clinical disease activity (p < 0.0001) and disease duration (p = 0.02) were associated with higher IBD-DI scores. The responsiveness of the IBD-DI is being evaluated in ongoing prospective studies such as CURE [EudraCT Number: 2013-003199-11] and the ICARE [ClinicalTrials.gov identifier: NCT02377258] studies. It is expected that the IBD-DI should be a major secondary endpoint in clinical practice and future disease-modification trials, but this requires further longitudinal evaluation. 34
Disability index in inflammatory bowel disease (IBD), the IBD disability index (IBD-DI). 33
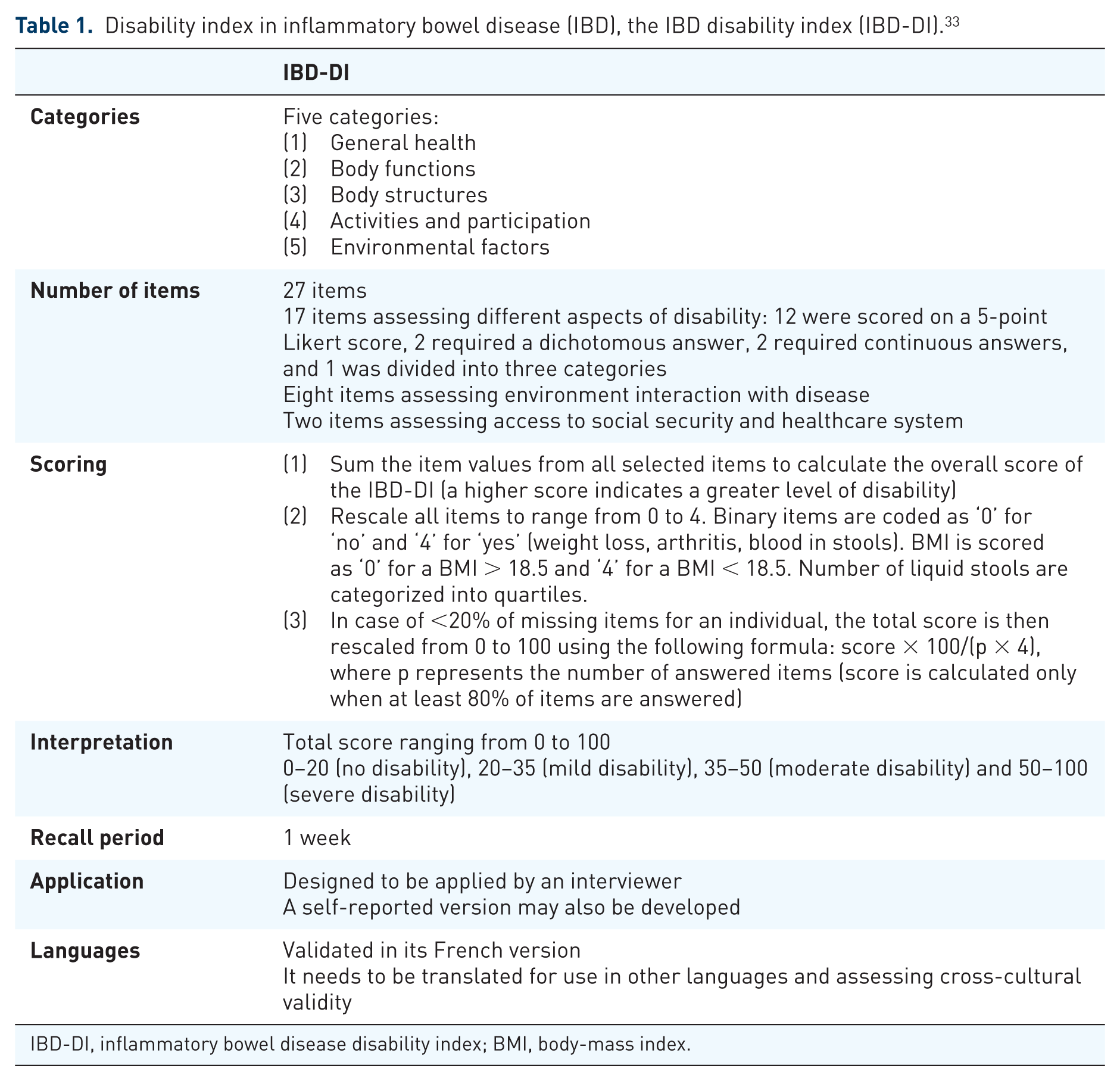
IBD-DI, inflammatory bowel disease disability index; BMI, body-mass index.
Interestingly, in a recent large French nationwide survey of patient-reported outcomes in IBD, 1185 patients were included in the analysis. In total, half of patients reported poor quality of life (SIBDQ < 45:53%), severe fatigue (Functional Assessment of Chronic Illness Therapy (FACIT) < 30:47% and/or depression (hospital anxiety and depression (depression component) (HAD)-D > 7:49%). One third of patients reported anxiety (Hospital Anxiety and Depression (HAD)-A > 7:30%) and /or moderate (22%) or severe (12%) disability. Around half of patients had moderate-to-severe loss of work productivity and loss of activity. This study demonstrates that disease burden is very high in IBD, and disability is prevalent in one third of patients. 26
In a recent study of 84 patients with restorative proctocolectomy, the IBDQ was compared with the IBD-DI, and they found them to be highly correlated (r = 0.84, p < 0.01).33,35 Worse quality of life and disability were found in those who had their position affected at work (both p < 0.01) and those who had more than 100 days off work in the last year (p < 0.01 for quality of life and p = 0.012 for disability). Lower quality of life and disability scores were associated with higher indirect and total costs (p < 0.01). 35
Patients with UC, and familial adenomatous polyposis and subsequent ileoanal pouch anastomosis had less disability than those with CD (as a final diagnosis). This led to several conclusions, including the finding of higher disability in patients with CD versus UC and lower disability scores in patients with restorative proctocolectomy with ileal pouch anal anastomosis compared with medical-treated patients.35,36 In another study, HRQOL and the IBD-DI was compared in patients with UC (86 who had surgery and 119 patients who were receiving anti-TNF therapy). The authors reported that pouch patients had better overall health compared with the anti-TNF group, and patients who had surgery had more gastrointestinal symptoms than those treated with anti-TNF therapy. However, overall median IBD-DI scores were similar between the groups. 37
Despite perceived improvements in quality of life with pouch surgery, 38 bowel functioning and quality of life are not normal in many patients, as patients frequently experience unwanted side effects, for example, leakage, fecal urgency, and pouchitis, indicating that surgery does not prevent future disability in many of these patients. 39 More recently, a self-reported version of the IBD Disability Index (IBD-DI) has been validated in a population-based cohort of IBD patients. 40 Disability, in general, is associated with lower earnings, indirectly and directly, it also has been associated with reducing access to education and can lead to social exclusion. This impact of disability on society is challenging for health promotion, as disability can be preventable or ameliorated. 41 Disability is a major factor of disease burden in IBD, and the main associations with disability of disease severity are: the impact of the disease on the individual, disease burden, and the disease course. A disease severity classification including disability is being developed and validated by the The International Organization for the Study of Inflammatory Bowel Diseases (IOIBD). 42
The inflammatory bowel disease disk, a simple tool for routine practice
As the IBD-DI evaluates functional status it is used mainly in the clinical trial setting. A more recent IBD disk (see Figure 1 and Table 2) was developed, which is a shortened, self-administered adaptation of the validated IBD-DI. This should permit immediate visual representation of patient-reported The International Organization for the Study of Inflammatory Bowel Diseases (IOIBD)-related disability. In the preparatory phase, the IBD CONNECT group (30 health care professionals) ranked IBD-DI items in the perceived order of importance.

Disability in inflammatory bowel disease (IBD) components of disability according to the IBD disk consensus agreement. 43
Description of the inflammatory bowel disease disk: a simple way to capture the patients’ perspective? 43 .

IBD, inflammatory bowel disease.
The steering committee then selected 10 items from the IBD-DI to take forward for inclusion in the IBD disk. In the consensus phase, the items were refined and agreed by the IBD Disk Working Group (comprising 14 gastroenterologists) using an online Delphi consensus process. After consensus agreements, 10 items were agreed for inclusion in the IBD disk including: abdominal pain, body image, education and work, emotions, energy, interpersonal interactions, joint pain, regulating defecation, sexual function and sleep.
The IBD disk tool lacks validation but has the potential to be a valuable outcome measure for use during routine clinical visits and may be able to accurately capture specific disability-related issues and correlate changes in disability over time. 44
Can we prevent disability? Lessons from disease-modification trials in non-inflammatory bowel disease conditions
Rheumatoid arthritis
Rheumatic diseases (including RA) are chronic and progressive and they cause damage to the locomotor system leading to disability in patients. 45 In patients with RA, around half received legal disability status, with around one third considered to be severely disabled in the long term. 46 The healthcare costs associated with sick leave and permanent incapacity in RA are significant. 47 Over the past 20 years the management of RA has improved dramatically as a consequence of earlier initiation of disease-modifying antirheumatic drugs (DMARDs), better markers, and closer monitoring of disease activity and biologic therapies. 48
Joint damage has been shown as a potential predictor of disability. A longitudinal relationship between radiographic progression and disability score (HAQ) was observed in a post hoc analysis of the TEMPO trial, evaluating etanercept in a population of patients with established RA (mean disease duration 6.4 years). 49 In the CONCERTO trial, early biologic and methotrexate-naïve RA patients were randomized to adalimumab plus weekly blinded methotrexate (MTX) (at doses of 2.5, 5,10 or 20 mg). The authors reported that increasing doses of MTX in combination with adalimumab was associated with a significant trend in improved clinical outcomes. In addition, disease measures of both functional and radiographic outcomes did not demonstrate statistical difference between treatment groups suggesting that any dose of MTX in combination with adalimumab is sufficient to determine these two important aspects of RA treatment. 50 In a large meta-analysis of anti-TNF trials (748 patients), joint damage (described as joint erosion and joint space narrowing) was associated with increasing disability scores (HAQ). 51 In a post hoc analysis of the BeSt study, evaluating the components of joint damage (joint erosions and joint space narrowing), found that erosion of the wrists was the most important independent predictor of functional disability. 52
The 2010 Rheumatoid Arthritis Classification Criteria was published by a collaborative initiative of the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR). The new classification redefined the treatment objectives of RA at high risk of chronicity and erosive damage by focusing on features at earlier stages of disease. It has been reported that patients treated early in the disease course with a DMARD and biological DMARD improve not only clinical outcomes but also have reductions in joint damage and long-term disability.50,53–56
Although structural joint damage progression is associated with the presence of clinical disease activity, several reports have underscored the presence of radiological progression in some patients with apparent clinical remission.57,58 These observations have introduced concepts and definitions such ‘complete or deep remission’. 59
The concept of treating to reach an objective target improves outcomes and has been studied in several chronic conditions like hypertension and diabetes. 60 The treat-to-target recommendations for RA were formulated in 2010 and updated in 2014.48,61 The agreed target for treatment of RA is clinical remission, defined as the absence of signs and symptoms of significant inflammatory disease activity. 61 Interestingly, studies have reported that tight control (of disease activity) by means of close monitoring of patients with objective scoring tools, and adjusting treatments towards a target endpoint, results in greater improvement and a higher percentage of patients achieving low disease activity and better outcomes in RA patients.62–66
In summary, the objectives of rheumatology physicians are to identify and treat patients earlier in their disease course to reduce inflammation, improve joint functioning and prevent or ameliorate joint damage and thereby long-term disability.
Multiple sclerosis
Disability is also common in MS.67–69 Disability in MS can be measured by several methods including: The Kurtzke Expanded Disability Status Scale (EDSS) (based on neurological examination and assessment of a range of neurological functions); the Multiple Sclerosis Functional Composite (MSFC); The Nine Hole Peg Test; and the Sloan Low Contrast Letter Acuity. 68
Several important phase III trials have confirmed the benefit of certain drugs in reducing MRI activity in MS patients with Fingolimod (sphingosine-1-phosphate receptor modulator), 70 natalizumab (anti-beta integrin monoclonal antibody) 71 and rituximab (anti CD-20 monoclonal antibody), 72 however none of these agents reduced progression of disability in these patients.
In planned subgroup analyses with rituximab, participants younger than 50 years and those with gadolinium-enhanced lesions at baseline showed benefit on disability progression. 72 Based on these results, a humanised anti-B lymphocyte monoclonal antibody, ocrelizumab, was evaluated in a phase III trial. In a recently reported trial, ocrelizumab appeared to reduce the risk of disability progression in MS by 24%. 73 This trial enrolled relatively young patients (mean age of 45 years) with short disease duration (mean disease duration of 6.4 years) and a relatively high proportion of participants had gadolinium-enhanced lesions at baseline (26%). The subgroup with gadolinium-enhanced lesions at baseline seemed to have a greater reduction in risk of disability progression, although the difference was not significant [hazard ratio (HR) 0.65; for those with enhanced lesions versus 0.84 those without]. The different results that have been reported in trials of progressive MS seem not to relate to anti-inflammatory drug effects. The result suggests that trials enrolling a study population with younger age, shorter disease duration, and greater inflammatory lesion activity tend to exhibit greater benefit.
Interestingly, in a recent study of MS patients with no disease activity at 2 years, this was associated with a positive predictive value of 78% for absence of disability at 7 years. 74 In addition, other studies have reported that clinical and radiological (magnetic resonance imaging, MRI) parameters had a better predictive value for disability progression than individual measures in MS75–77 and an inclusion of patient-reported outcome measures in these trials may further improve the accuracy of this tool in MS patients. 67
The findings abovementioned have led to greater interest in the concept of deep remission, tight control and potentially disease modification, with reduction or prevention of long-term disability in IBD as in other Immune mediated inflammatory disease (IMIDs).78–80
Can we identify early disease and modify the disease course in inflammatory bowel disease to prevent disability?
The main focus on identifying early IBD to aggressively arrest inflammation, thereby preventing bowel damage and future disability, has been based on the identification of early CD. Previous studies have demonstrated that in patients with earlier CD, there appeared to be greater efficacy with regards anti-TNF therapy than in those with later or more established disease.78,81 The reasons for this disparity are unclear but should suggest processes are a greater inflammatory burden in earlier disease and differing cytokine profiles in the two stages of disease.82–85 An international consensus has proposed the ‘Paris Definition for Early Crohn’s Disease’ that defines it as disease duration ⩽ 18 months after diagnosis and without previous exposure to immunosuppressants or biological therapies. 86
The concept of identifying early disease and then modifying the natural history with drugs to avoid later disease complications and prevent disability is gaining traction in current opinion. A term that was previously introduced into the literature in 2013 was DMAIDs, that is, disease-modifying anti-inflammatory bowel disease drugs and its premise is based on DMARDs in RA.87,88 Despite their widespread use in IBD management, thiopurines have proved ineffective for disease modification in CD.89,90 The previous treatment goal for CD was to induce and then ensure steroid-free remission; this lends itself to the concept of deep remission, whereby reducing inflammation may lead to reduced surgeries, hospitalizations and ultimately, disability. Whether current drugs are able to achieve these goals will require further investigation.
In the recently reported Randomised Evaluation of an Algorithm for Crohn’s Treatment (REACT) study, community gastroenterology practices from Belgium and Canada were randomly assigned to early combined immunosuppression (Early combined immunosuppression (ECI), an anti-TNF and antimetabolite drug) or conventional management. 91 It was the first disease-modification trial in CD. 91 The primary outcome of remission rate at month 12 was similar for both groups (66% versus 62%, p = 0.52). 91 However, the 24-month composite rate of major adverse outcomes (defined as surgical intervention, hospital admission, or serious disease-related complications) was lower at ECI practices than at conventional management practices (27.7% versus 35.1%, respectively; HR: 0.73; 95% confidence interval 0.62–0.86, p = 0.0003]. 91 Unfortunately the REACT study did not assess disability as an endpoint and this may have led to more informative outcomes of different treatment strategies on long-term disability.
Perspectives
Disability is prevalent in IBD and is seen in patients with UC (before and after surgery) and in CD. The IBD-DI should become a major secondary endpoint in clinical trials. 34 This index needs to be expanded to include worldwide comparisons of disability among IBD patients in a longitudinal fashion. Future disease-modification trials in IBD should consider the inclusion of patients with early IBD, the use of the Lémann index (in CD) and the IBD-DI as defined endpoints, 92 and stratifying patients with disease severity.27,93
The recent development of the IBD disk has the potential to be a valuable tool for use during routine clinical visits and may be able to accurately capture specific disability-related issues and correlate changes in disability over time (Figure 1 and Table 2). 44
Future clinical trials will move away from simply targeting response and remission to ensure deep remission, improvement in defined patient-reported outcomes and ultimately preventing and improving disability in IBD.
The costs and safety of these new therapeutic strategies in IBD that are being developed to change the natural history of disease with earlier and effective treatments in order to reduce long-term disability in IBD patients, remain to be established; however, the potential patient and public health benefits achieved warrant consideration in their own right.88,94
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
PBA: consulting fees from Merck, Abbvie, Janssen, Ferring, Tillots, Celgene, Takeda, Norgine, GSK, Allergan. Lecture fees from Merck, Abbvie, Janssen, Ferring, Tillots, Celgene, Takeda, Norgine, GSK, Allergan.
CGR: speaker fees for Takeda France, MSD France and Ferring France.
LPB: Consulting fees from Merck, Abbvie, Janssen, Genentech, Mitsubishi, Ferring, Norgine, Tillots, Vifor, Therakos, Pharmacosmos, Pilège, BMS, UCB-pharma, Hospira, Celltrion, Takeda, Biogaran, Boerhinger-Ingelheim, Lilly, Pfizer, HAC-Pharma, Index Pharmaceuticals, Amgen, Sandoz, Forward Pharma GmbH, Celgene, Biogen, Lycera, Samsung Bioepis. Lecture fees from Merck, Abbvie, Takeda, Janssen, Takeda, Ferring, Norgine, Tillots, Vifor, Therakos, Mitsubishi, HAC-pharma.