
Abstract
Background:
Colon capsule endoscopy (CCE) is a procedure in which capsule swallowing facilitates observation of the lumen of the entire digestive tract. It does not require an air supply, and is a noninvasive procedure with a markedly low risk of adverse events in comparison with conventional colonoscopy (CS). It reduces patient stress, and may be acceptable to patients. A limitation of this procedure is that the entire colon observation rate (CCE excretion rate, completed CCE rate) is not 100%. In this study, we prospectively investigated clinical factors important to achieve observation of the entire colon on CCE.
Methods:
The participants were 70 patients for whom CCE was scheduled, and from whom written informed consent regarding participation in this study was obtained. We selected patient background/examination factors, and analyzed all factors involved in observation of the entire colon and factors for completion of the CCE within 4 h after the start of examination using multivariate analysis.
Results:
Of the 70 enrolled patients, 64 were analyzed, excluding 6. On multiple logistic analysis, only a water intake of ⩾12.0 ml/min during examination [p = 0.025, odds ratio (OR): 46.753, 95% confidence interval (CI): 1.630–1341.248] was identified as an independent predictive factor involved in observation of the entire colon. With respect to factors involved in the completion of CCE within 4 h, multiple logistic analysis showed that a body mass index (BMI) of ⩾25 (p = 0.039, OR: 13.723, 95% CI: 1.135–165.913), the absence of constipation (p = 0.030, OR: 13.988, 95% CI: 1.287–152.047), and a water intake of ⩾12.0 ml/min during examination (p = 0.004, OR: 12.028, 95% CI: 2.225–65.029) were independent predictive factors.
Conclusions:
Completion of a CCE was most closely related to water intake per hour. In addition to water intake, CCE-promoting factors included a high BMI and the absence of constipation.
Introduction
Colonoscopy (CS) is a gold standard for the diagnosis of colorectal diseases such as colorectal cancer or inflammatory bowel disease. However, it is difficult to perform complete CS in some patients, and others hesitate to undergo CS. The cecal intubation rates on CS are reportedly 85– 95% [Anderson et al. 2000; Shah et al. 2007; Aljarallah and Alshammari, 2011; Koido et al. 2014; Dafnis et al. 2005; Fasoli et al. 2002], and other procedures will be suggested in patients with incomplete CS.
Colon capsule endoscopy (CCE) is a procedure in which capsule swallowing facilitates observation of the lumen of the entire digestive tract. It does not require an air supply, and is a noninvasive procedure with a markedly low risk of adverse events in comparison with conventional CS. It reduces patient stress, and may be acceptable to patients [Saito et al. 2015].
Another option of colorectal examination is computerized tomography (CT) colonography (CTC). The sensitivity and specificity of CTC is high in the diagnostic yield of colorectal polyps, suggesting the usefulness of CTC [Johnson et al. 2008; Graser et al. 2009; Regge et al. 2009]. On the other hand, a study indicated that the sensitivity and specificity of CCE for colorectal polyp detection were favorable in patients with incomplete CS, and that the colorectal polyp detection rate was higher than that of CTC [Spada et al. 2015]. As such, demands for CCE have been increasing and the role of CCE will become more important in the future.
However, issues to be clinically resolved have been raised: the entire colon observation rate on CCE (excretion rate, completed CCE rate) is not 100%. According to previous clinical studies, the rate ranges from 70–90% [Eliakim et al. 2006; Schoofs et al. 2006; van Gossum et al. 2009; Herrerías-Gutiérrez et al. 2011; Spada et al. 2011a]. To improve the excretion rate, preparation regimens have been discussed. However, no clinical study has been conducted into the types of patient that can complete CCE. In other words, factors influencing complete CCE have not been reviewed. It is essential to select the patient who is suitable for CCE.
Even CS could not achieve total colon observation in all patients, though it is the gold standard of colon examination. Factors associated with incomplete CS have been reported in the literature: sex (female) [Anderson et al. 2000; Shah et al. 2007; Koido et al. 2014; Dafnis et al. 2005; Cirocco and Rusin 1995], age (elderly) [Shah et al. 2007; Aljarallah and Alshammari 2011; Koido et al. 2014; Dafnis et al. 2005], previous abdominal or pelvic surgery [Shah et al. 2007; Koido et al. 2014; Cirocco and Rusin 1995], and diverticulum [Dafnis et al. 2005]. However, considering the characteristics of CCE, factors involved in difficulty in CCE excretion may differ from these factors. These factors should be investigated to understand whether the patient is suitable for CCE. If factors influencing complete CCE are clarified, patients in whom a CCE can be readily excreted can be selected; for such patients, the dose of a cleaning liquid can be reduced. It may be possible to establish order-made regimens appropriate for individual patients in the future. For patients in whom completion of the CCE procedure is difficult, and who do not wish to undergo CS, other colorectal examinations, such as CTC, may be adequately performed, and this may finally increase the proportion of patients undergoing CS.
The purpose of this study was to investigate clinical factors important to prospectively achieving completion of the CCE procedure and find CCE-matched patients.
Material and methods
Patients
We selected patients that were at least 20 years old, for whom a CCE was scheduled between June 2015 and February 2016, and from whom written informed consent regarding participation in this study was obtained, regardless of sex. We excluded patients with stenosis of the digestive tract, those definitively diagnosed with Crohn’s disease, those who had undergone abdominal radiotherapy, those with pacemaker insertion, those with dysphagia, those with a history of hypersensitivity to drugs for examination, those in whom acute abdomen was suspected, those with spastic constipation, those with severely hard stools, and those with an electrolyte imbalance. The primary endpoint of this study was to prospectively clarify factors important to achieve completion of the CCE procedure. Its secondary endpoint was to clarify factors involved in the completion of a CCE within 4 h. The protocol of this study was approved by the Ethics Review Board of Nagoya University Hospital, Japan (2014-0255), and registered at the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (UMIN000015277).
To patients for whom a CCE was scheduled, the purpose and contents of this study were explained, and informed consent was obtained. We took a blood test for checking the electrolyte imbalance related to the oral administration of several kinds of cleaning liquids and prokinetics. Prior to this study, a questionnaire survey of each patient’s background regarding factors involved in entire colon observation was conducted. A pedometer (Lifecorder GS; Suzuken Co. Ltd, Nagoya, Japan) was attached to a waist belt immediately before examination. A CCE was performed according to the bowel preparation regimen presented in Table 1. This regimen is currently one of the Japanese standards because sodium phosphate (NaP) is not available in Japan. Polyethylene glycol (PEG) is frequently used as the main booster in Japan.
Schedule of bowel preparation used in the study.

CCE, colon capsule endoscope; PEG, polyethylene glycol.
Definitions in this study
‘Non-CCE excretion’ refers to cases in which a CCE is not excreted within the battery time, and does not mean retention of the capsule. Patients receiving any laxatives regularly, regardless of fecal property or frequency, were regarded as having ‘constipation’. ‘Previous abdominal surgery’ refers to abdominal surgery without intestinal resection. In this study, there was no patient who had undergone intestinal resection. ‘Abdominal symptoms’ refer to the presence of symptoms, such as abdominal pain, distension or discomfort, for 3 days or more per month, within the past 3 months. Patients receiving drug therapy for diabetes regardless of HbA1c or those with an HbA1c of ⩾6.5% were regarded as having diabetes. The number of steps during examination and amount of water intake involving cleaning liquids were calculated every hour and reviewed in the analysis.
Colon cleansing level
In accordance with a previous article, we used ‘excellent/good/fair/poor’ to categorize the colon cleansing level [Leighton and Rex 2011]. ‘Excellent/good’ levels were evaluated as adequate, and ‘fair/poor’ as inadequate. We evaluated the colon cleansing level by dividing the colon into four segments: right colon (cecum, ascending colon), transverse colon, left colon (descending colon, sigmoid colon), and rectum.
Statistical analysis
All data were analyzed using SPSS version 23.0 statistical software (IBM, Tokyo, Japan). Logistic regression was used to estimate the hazard ratio (HR) and the 95% confidence interval (CI) of various factors associated with achieving completion of the CCE. Differences with values of p < 0.05 were considered statistically significant.
Results
Patient characteristics
During the study period, 70 patients were enrolled. This analysis was performed in 64 patients. Of the 6 that were excluded, 2 were excluded because the capsule could not reach the cecum within the examination time, 2 dropped out during examination because they were unable to take the amount of cleaning liquids, and 2 were excluded due to machinery problems.
Concerning the patient background, the mean age was 57.8 years, and the patients consisted of 36 males and 28 females, with a mean body mass index (BMI) of 22.7. The proportion of patients with constipation was 25.0%. Those who had undergone abdominal surgery accounted for 35.9%, those with abdominal symptoms accounted for 40.6%, those with diabetes accounted for 12.5%, and those with ulcerative colitis accounted for 15.6%. To assess the severity of comorbidity, we used Charlson comorbidity index [Charlson et al. 1987], and the mean index was 0.66 (Table 2).
Patient characteristics.

BMI, body mass index.
CCE results
With respect to the results of CCE, overall, the excretion rate (completed CCE rate) was 81.3% (52/64). The mean gastric transit time was 44.6 min, and the mean small intestinal transit time was 61.0 min [Hejazi et al. 2016]; shorter than conventional small intestinal capsule endoscopy. The mean colorectal transit time was 134.7 min, and the mean duration of all examinations was 355.5 min. Concerning the colon cleansing level, right colonic, transverse colonic, left colonic, and rectal levels were evaluated as adequate in 95.9%, 98.0%, 95.9%, and 89.8% of the patients, respectively. Patients with any findings accounted for 95.3%: diverticulum was observed in 62.5%, and colorectal polyps in 50.0%. There were no CCE-related adverse event, such as retention, or adverse reaction to cleansing liquids, such as nausea, vomiting or abdominal pain, in any patient. In the nonexcretion group, the final sites of CCE arrival were the left colon in 96.3% (11/12) of the patients and right colon in 8.7% (1/12). The mean total water intake was 3895.8 ml (Table 3).
Results of CCE procedure.
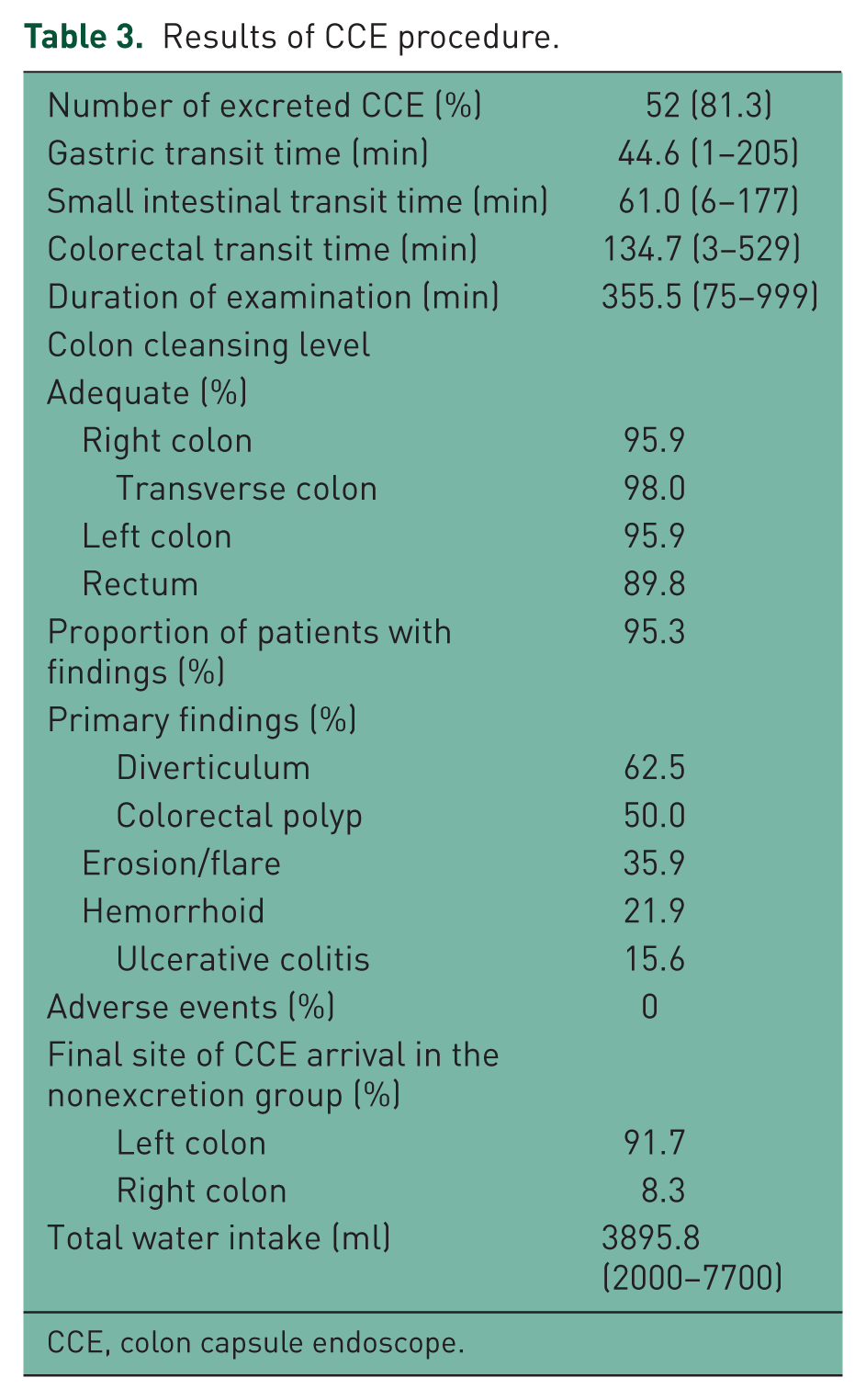
CCE, colon capsule endoscope.
Comparison of excretion and nonexcretion group
Factors that may influence excretion during a CCE were compared between the excretion and nonexcretion groups, as shown in Table 4. There were no significant differences in the age, sex, BMI, previous abdominal surgery, presence or absence of ulcerative colitis, Charlson comorbidity index, number of steps during examination, gastric transit time, small intestinal transit time, presence or absence of colorectal polyps, or presence or absence of diverticulum. There were significant differences for complete CCE excretion in the factors, constipation, abdominal symptoms, diabetes, and water intake during examination between the two groups.
Comparison of excretion and nonexcretion group.

Mann–Whitney test **Fisher’s exact method.
BMI, Body mass index.
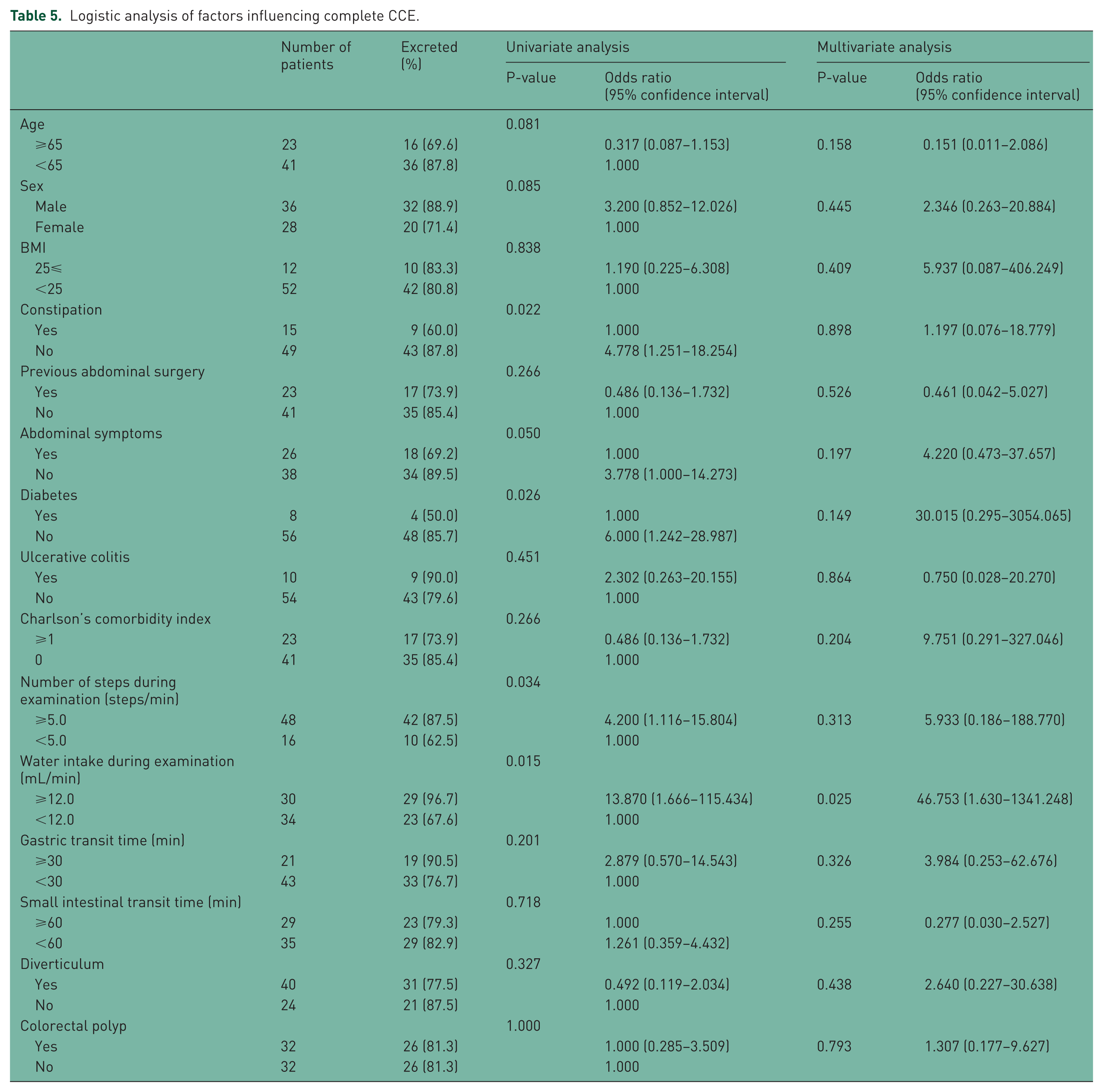
Univariate and multivariate analyses using logistic regression
The results of a review to clarify factors important to achieve completion of CCE are shown in Table 5. On univariate analysis, 4 factors were significantly associated with the excretion rate: the absence of constipation [p = 0.022, odds ratio (OR): 4.778, 95% CI: 1.251–18.254], absence of abdominal symptoms (p = 0.050, OR: 3.778, 95% CI: 1.000–14.273), a step count of ⩾5.0 per minute during examination (p = 0.034, OR: 4.200, 95% CI: 1.116–15.804), and a water intake of ⩾12.0 ml/min during examination (p = 0.015, OR: 13.870, 95% CI: 1.666–115.434). When performing multiple logistic analysis on all items, only a water intake of ⩾12.0 ml/min during examination (p = 0.025, OR: 46.753, 95% CI: 1.630–1341.248) was identified as an independent predictive factor.
Logistic analysis of factors influencing complete CCE.
The results of a review to clarify factors contributing to the completion of CCE within 4 h are shown in Table 6. On univariate analysis, four factors were significantly associated with CCE excretion within 4 h: the absence of constipation (p = 0.018, OR: 5.333, 95% CI: 1.334–21.325), ulcerative colitis (p = 0.044, OR: 5.391, 95% CI: 1.045–27.812), a water intake of ⩾12.0 ml/min during examination (p > 0.001, OR: 10.679, 95% CI: 3.350–34.036), and a short intestinal transit time of <60 min (p = 0.045, OR: 2.850, 95% CI: 1.026–7.916). When performing multiple logistic analysis in all items, a BMI of ⩾25 (p = 0.039, OR: 13.723, 95% CI: 1.135–165.913), the absence of constipation (p = 0.030, OR: 13.988, 95% CI: 1.287–152.047), and a water intake of ⩾12.0 ml/min during examination (p = 0.004, OR: 12.028, 95% CI: 2.225–65.029) were identified as independent predictive factors.
Logistic analysis of factors influencing complete CCE within 4 hours.

Discussion
The morbidity and mortality rates of colorectal cancer remain high. To prevent colorectal cancer development and colorectal cancer-related death, it may be important to positively undergo colorectal examination. The sensitivity and specificity of second-generation CCE for detecting colorectal polyps measuring ⩾6 mm is 63–91% and 64–94%, respectively; this procedure proves to be useful [Spada et al. 2011b, 2011c, 2012; Eliakim et al. 2009; Hartmann et al. 2012]. On the other hand, several issues to be clinically resolved have been raised. In particular, the most important issue is that the entire colon observation rate (excretion rate, completed CCE rate) is not 100%. One idea for improving completed CCE rates was to identify the patients most suitable for CCE. Therefore, we conducted a prospective study to clarify factors important to achieve completion of CCE (Table 5).
Water intake per hour during examination was identified as an independent predictive factor important to achieve completion of CCE. This suggests that if water is not ingested at a specific speed or faster, it is not effective in achieving completion of CCE. PEG solution, which was used in this study, is isotonic, and does not cause any colonic membrane-mediated changes [Keeffe, 1996]. Briefly, the oral administration of PEG solution at a specific speed or faster and intestinal retention of water involving PEG solution, may be important for CCE excretion. To achieve a complete CCE, it may also be important to select the patients who can drink enough cleansing liquids at a satisfactory speed.
Factors associated with incomplete CS, sex (female), age (elderly), previous abdominal or pelvic surgery, and diverticulum have been indicated, but, of these, no factor was identified as a factor that makes CCE excretion difficult, though both CS and CCE belong to the category of colorectal examination. One reason was that we could understand the relationship between constipation and late CCE excretion, since constipation patients have a long, spastic or very relaxed colon. Another reason was speculated that water intake during CCE significantly affected the completion of CCE with a high OR and therefore the other factors could not affect it. Our results provide useful information for selecting the colorectal examinations; for those with factors associated with incomplete CS, such as sex (female), age (elderly), previous abdominal or pelvic surgery, and diverticulum, CCE may be positively recommended, because these factors do not make CCE excretion difficult. For those who are unable to drink a sufficient volume of water, involving cleansing liquids, CS should be selected rather than CCE. For those who refuse CS despite the above conditions, appropriate examinations, such as CTC, may be selected with reference to the individuals’ characteristics.
We also reviewed factors excreting the capsule within 4 h (Table 6). A BMI of ⩾25, the absence of constipation, and enough water intake during examination were identified as independent predictive factors.
Constipation affected CCE excretion time. We defined constipation as the status of the patient who used any laxative regularly. When selecting CCE, the regular use of laxative should be ascertained prior to examination.
A BMI of ⩾25 as an independent predictive factor reflects that a CCE is more readily excreted in patients with a higher abdominal and visceral fat level. A study reported lower BMI as a factor associated with incomplete CS [Anderson et al. 2000], suggesting that abdominal wall and visceral fat prevents loop formation on colonoscope insertion, facilitating endoscope insertion in the obese patient. There may also be similar mechanism in CCE. In patients with a BMI ⩾ 25, that is, obese patients, visceral fat-related abdominal pressure may always be loaded on the intestinal tract in comparison with thin patients. This abdominal pressure can contribute to early CCE excretion. In this study, the capsule was left in the left colon, especially the sigmoid colon, in most patients in whom a CCE was not excreted out of the body. In such patients, real-time monitoring or imaging showed flexions of the sigmoid colon for a long duration. This may have been related to curvatures, and the flexions may have made it impossible for the capsule to go through the sigmoid colon. A study reviewed CTC findings in patients with incomplete CS, and indicated the length of the colon, that of the transverse colon, that of the sigmoid colon, number of curvatures, and diverticulum as factors associated with incomplete CS [Hanson et al. 2007]. The number of sigmoid colon curvatures should be examined in the future. Furthermore, another study investigated the length, maximal diameter, and surface area of the intestinal tract through enema, and reported that the maximal diameter of the sigmoid colon was the second shortest, following that of the descending colon, and that the length and surface area of the sigmoid colon were the second longest and largest, following those of the transverse colon [Sadahiro et al. 1992].
A main limitation of this study was the types of boosters. Boosters were the important factors to achieve completion of the CCE. NaP and sodium sulfate (Suprep) were not used in this regimen. Although NaP and Suprep are useful as a booster [Spada et al. 2011c; Singhal et al. 2014], they are not available in Japan; PEG is mainly used as a booster in Japan. Nevertheless, a paper reports that PEG has been proven to have a poor effect as a booster [Spada et al. 2011c]. PEG acts as a booster due to a cascade effect, whereas other boosters can act through an activation of colonic movements. With the NaP and Suprep regimen, it will be necessary to review examination-related factors along with the number of steps and water intake during examination. Furthermore, the number of patients, which was relatively small despite being a prospective study, also had limitations. The target sample size on the trial registry was 100 patients; however we analyzed the data of 70 patients and obtained significant results, and so patient recruitment was stopped. In the future, a larger number of patients should be investigated by using other regimens.
In conclusion, the completion of CCE was most closely related to water intake per hour in regimens including PEG as a booster. In addition, excretion-accelerating factors included a high BMI and the absence of constipation. However, the results of this study cannot be directly translated to regimens of preparations containing different boosters.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.