
Abstract
Background:
The clinical outcome of patients with obscure gastrointestinal bleeding (OGIB) during antithrombotic drug therapy has not been fully investigated.
Methods:
Patients who underwent video capsule endoscopy (VCE) for the investigation of OGIB at Okayama University Hospital from January 2009 to March 2016 were enrolled. We evaluated the VCE findings, the patterns of OGIB, and the rate of rebleeding within 1 year in antithrombotic drug users and antithrombotic drug nonusers.
Results:
A total of 181 patients were enrolled. Among the antithrombotic drug users, the rate of VCE positivity in the patients with overt OGIB was significantly higher in comparison with patients with occult OGIB (45% versus 16%, p = 0.014), whereas there was no significant difference among the antithrombotic drug nonusers (27% versus 26%, p = 1.0). Among the antithrombotic drug users, the rate of rebleeding among the VCE-positive patients was significantly higher in comparison with the VCE-negative patients (50% versus 5.9%, p = 0.011). Moreover, among antithrombotic drug users who did not receive therapeutic intervention, the rate of rebleeding among the VCE-positive patients was significantly higher in comparison with the VCE-negative patients (75% versus 6.3%, p = 0.001). However, among the antithrombotic drug nonusers who did not receive therapeutic intervention, the rebleeding rate of the VCE-positive patients was not significantly different from that of the VCE-negative patients (20% versus 9.4%, p = 0.43).
Conclusion:
Therapeutic intervention should be considered for patients with overt OGIB who are VCE positive and who use antithrombotic drugs due to the high risk of rebleeding.
Introduction
Oral antithrombotic therapy has been used to reduce the risk of thromboembolic complications. 1 On the other hand, it might cause gastrointestinal bleeding by inducing mucosal damage, impairing mucosal healing, or by aggravating blood loss from pre-existing lesions. 2 In daily practice, we encounter antithrombotic drug users with obscure gastrointestinal bleeding (OGIB), and it is often difficult to diagnose the origin of their bleeding. Furthermore, some patients suffer from rebleeding events. OGIB is defined as bleeding of unknown origin that persists or recurs after esophagogastroduodenoscopy, colonoscopy, or the radiological evaluation of the small bowel. 3 OGIB accounts for 5% of all cases of gastrointestinal bleeding, and is often caused by small bowel lesions. 4 In patients presenting with OGIB, the diagnostic yield of video capsule endoscopy (VCE) ranges from 38% to 93%,5,6 and is superior to other diagnostic modalities, including push enteroscopy, computed tomography, and angiography. 7 Thus, VCE is recommended as the initial investigation to detect sources of bleeding.6,8
There have been some reports on the clinical outcomes or risk factors for rebleeding in patients with OGIB.9–11 Additionally, some authors have described an increased relative risk of recurrent OGIB in patients under anticoagulant therapy.12–14 However, the clinical outcome of patients with OGIB during antithrombotic drug therapy has not been investigated in detail.
The aim of this study was to elucidate the clinical outcome of patients with OGIB according to their antithrombotic drug use.
Methods
Study design and patients
This was a single center, retrospective, observational study. Patients who underwent VCE for the investigation of OGIB at Okayama University Hospital from January 2009 to March 2016 were enrolled. Patients in whom the source of bleeding was proven to be outside the small intestine were excluded. All patients underwent upper and lower gastrointestinal endoscopy before VCE, and it was confirmed that the examinations were negative or insufficient to explain the bleeding. Balloon-assisted endoscopy (BAE) was carried out as a therapeutic intervention, or diagnostic biopsy was performed, as necessary. In patients who underwent VCE two or more times, only the first examination was included in the present study. Written informed consent was obtained from all patients for inclusion in the study. This study protocol was approved by the Okayama University Hospital Ethics Committee in April 2017 (approval number 1706-011).
Variables
The clinical parameters of the patients including age, sex, comorbidities (hypertension, chronic kidney disease, liver cirrhosis, ischemic heart disease, and hematologic disease), antithrombotic drug use (antiplatelet or anticoagulant), concomitant drug use [nonsteroidal anti-inflammatory drugs (NSAIDs), proton-pump inhibitor (PPI), histamine-2 receptor antagonist (H2-RA), and mucoprotective agent], VCE findings, patterns of OGIB (overt bleeding or occult bleeding), treatment methods, and rebleeding rate within 1 year were analyzed. OGIB is often further subclassified into two types: obscure–occult, characterized by recurrent iron-deficiency anemia or positive fecal occult blood testing, and obscure–overt, characterized by the passage of visible blood, melena, or hematochezia.3,15
We classified the enrolled patients into the antithrombotic drug user and antithrombotic drug nonuser groups, and compared their clinical outcomes. First, we evaluated the rates of VCE positivity according to the patterns of OGIB. Second, we evaluated the rebleeding rates according to the VCE findings among the overt bleeding cases and the occult bleeding cases. Third, we evaluated the rebleeding rates among patients who received no therapeutic intervention.
Video capsule endoscopy
VCE was later performed with a video capsule endoscopy device (PillCam SB2, Given Imaging Ltd., Yokneam, Israel). The capsule was swallowed with a solution of dimethicone after overnight fasting, without any other preparation. At 2 h) and 4 h after swallowing the capsule, the patients were allowed to drink clear liquids and to eat a light meal, respectively; at 8 h after swallowing the capsule, the sensor array and recording device were removed. The images were analyzed on a RAPID 6.5 workstation using with the Rapid Reader 6 software program (software and workstation from Given Imaging Ltd.). Two experienced endoscopists made the diagnoses after reaching an agreement with each other.
The definition of the video capsule endoscopy findings and rebleeding
The VCE findings were classified according to the P0-P2 system, 16 where P0 are less-relevant lesions that are definitive but not likely to be the cause of OGIB; P2 lesions are highly relevant lesions considered to be the cause of OGIB, such as angioectasia, varix, the presence of active bleeding, ulceration, multiple (⩾3) erosions, diverticulum and tumor. Examinations that revealed one or more P2 lesions were recorded as VCE positive.
An episode of rebleeding was defined as evidence of bleeding within 1 year after the index bleeding in cases of obscure–overt bleeding, or within 1 year after VCE in the patients with obscure–occult bleeding. 17 Bleeding was defined as a documented fall in the Hb level of 2 g/dl from the baseline level, the need for transfusion, or evidence of melena or hematochezia. 18
Statistical analysis
The sequential data were expressed as the median and interquartile range (IQR). The categorical data were compared using the chi-squared test or Fisher’s exact test. Bonferroni correction was performed when comparing more than two groups. Nonparametric data were compared using the Mann–Whitney U test. Two-tailed p values of <0.05 were considered to indicate statistical significance. All of the statistical analyses performed using the JMP Pro for Windows software program (version 12).
Results
Clinical characteristics
Figure 1 shows a flowchart of the present study. A total of 186 patients were diagnosed with OGIB during the study period. Five cases were excluded because the sources of bleeding were outside the small intestine. A total of 181 patients were finally enrolled in this study.
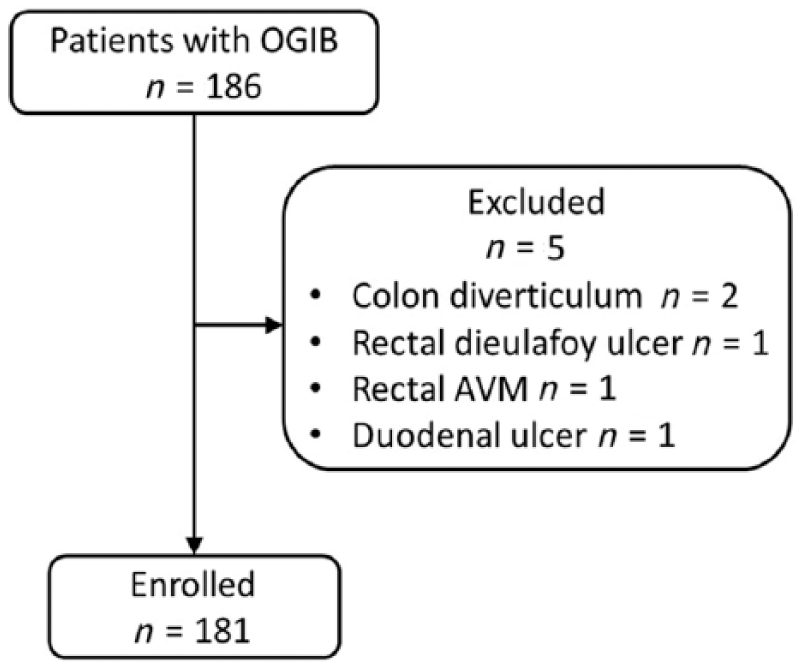
A flowchart of the present study.
Table 1 shows the clinical characteristics of the patients. The median age was 67 years, and the male-to-female ratio was approximately 1:1. Hypertension accounted for the highest proportion of the comorbidities. A total of 118 patients were antithrombotic drug nonusers, and 63 were antithrombotic drug users. The proportions of P0, P1, and P2 VCE findings were 46, 26 and 28%, respectively. The incidence of overt OGIB was 59%, which was higher than that of occult OGIB (41%).
The clinical characteristics of whole study population.

H2-RA, histamine-2 receptor antagonist; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drug; OGIB, obscure gastrointestinal bleeding; P0–P2, lesion classification; PPI, proton-pump inhibitor; VCE, video capsule endoscopy.
Table 2 shows the clinical characteristics of the antithrombotic drug users and the antithrombotic drug nonusers. The median age of the antithrombotic drug users was higher than that of the antithrombotic drug nonusers (72 years versus 65 years, p < 0.001). In the antithrombotic drug user group, the proportions of male patients and patients with hypertension, ischemic heart disease, diabetes mellitus, and concomitant PPI use were significantly higher in comparison with the antithrombotic drug nonuser group. There were no significant differences between the antithrombotic drug users and the antithrombotic drug nonusers with regard to the proportions of the VCE findings, vascular lesions, erosive or ulcerated lesions, patterns of OGIB, type of treatment, or the rate of rebleeding within 1 year.
The clinical characteristics of the antithrombotic drug users and the antithrombotic drug nonusers.

APC, argon–plasma coagulation; H2-RA, histamine-2 receptor antagonist; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drug; OGIB, obscure gastrointestinal bleeding; PPI, proton-pump inhibitor; VCE, video capsule endoscopy.
Difference of obscure gastrointestinal bleeding patterns according to the variety of antithrombotic drug
Table 3 shows the difference of OGIB patterns according to the variety of antithrombotic drug. The rate of overt bleeding cases in both the antiplatelet and anticoagulant drug users was significantly higher in comparison with that in the antiplatelet drug users (80% versus 36%, p = 0.029). In contrast, the rate of overt bleeding cases in both the antiplatelet and anticoagulant drug users was not significantly higher in comparison with that in the anticoagulant drug users (80% versus 45%, p = 0.12).
Difference of obscure gastrointestinal bleeding patterns according to the variety of antithrombotic drug.

OGIB, obscure gastrointestinal bleeding.
The rate of video capsule endoscopy positivity according to the patterns of obscure gastrointestinal bleeding
Figure 2 shows the rate of VCE positivity according to the patterns of OGIB. Among the antithrombotic drug users, the rate of VCE positivity in the patients with overt OGIB was significantly higher in comparison with that in patients with occult OGIB (45% versus 16%, p = 0.014), whereas there was no significant difference among the antithrombotic drug nonusers (27% versus 26%, p = 1.0).
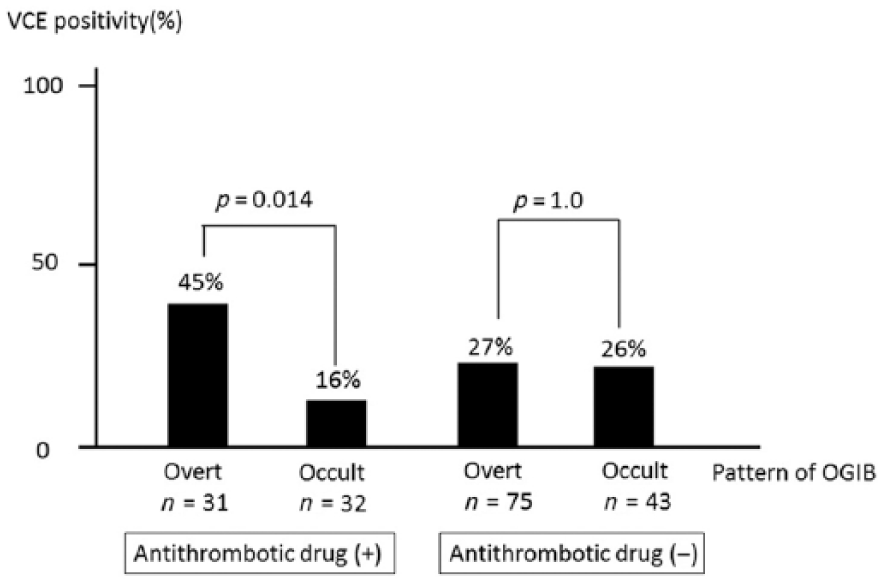
The rates of video capsule endoscopy positivity according to the patterns of obscure gastrointestinal bleeding.
The rate of rebleeding according to the video capsule endoscopy findings among the patients with overt and occult obscure gastrointestinal bleeding
Figure 3 shows the rate of rebleeding according to the VCE findings among the patients with overt OGIB. Among the antithrombotic drug users, VCE-positive patients showed a significantly higher rate of rebleeding in comparison with the VCE-negative patients (50% versus 5.9%, p = 0.011). Similarly, among the antithrombotic drug nonusers, VCE-positive patients tended to show a higher rate of rebleeding in comparison with the VCE-negative patients; however, the difference was not statistically significant (30% versus 10%, p = 0.064).

The rate of rebleeding among the patients with overt obscure gastrointestinal bleeding according to the video capsule endoscopy findings.
Figure 4 shows the rate of rebleeding according to the VCE findings among the patients with occult OGIB cases. Among the antithrombotic drug users, the rates of rebleeding among the VCE-positive and VCE-negative patients did not differ to a statistically significant extent (20% versus 3.7%, p = 0.29). Among the antithrombotic drug nonusers, there were no cases of rebleeding among either the VCE-positive and VCE-negative patients.

The rate of rebleeding among the patients with occult obscure gastrointestinal bleeding according to the video capsule endoscopy findings.
The rate of rebleeding among the patients who received no therapeutic intervention
Figure 5 shows the rate of rebleeding among the patients with overt OGIB who received no therapeutic intervention according to their VCE findings. Among the antithrombotic drug users, the rate of rebleeding was significantly higher in the VCE-positive patients in comparison with the VCE-negative patients (75% versus 6.3%, p = 0.001). However, among the antithrombotic drug nonusers, the rates of rebleeding among the VCE-positive and VCE-negative patients did not differ to a statistically significant extent (20% versus 9.4%, p = 0.43). Clinical information of rebleeding cases in the VCE-positive antithrombotic drug users who received no therapeutic intervention is shown in Table 4.
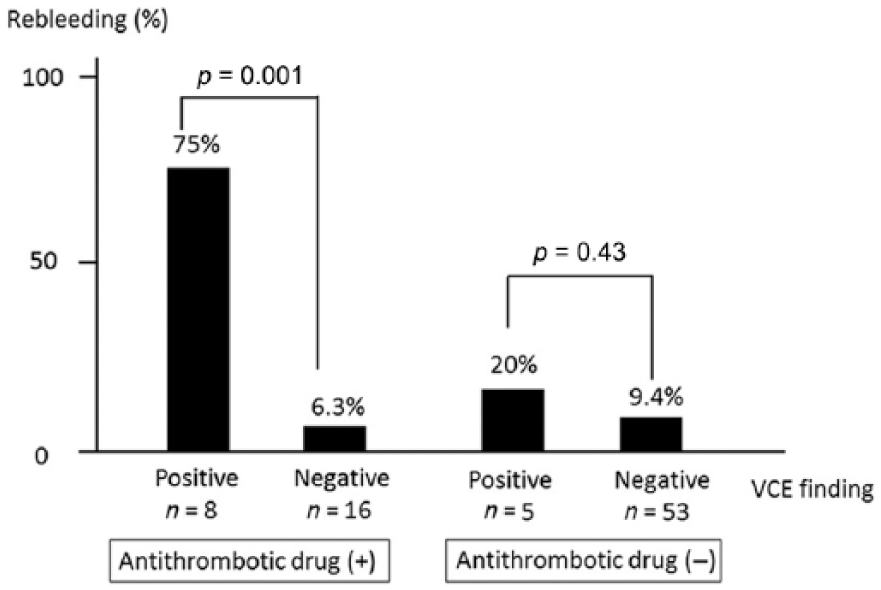
The rate of rebleeding among the patients with overt obscure gastrointestinal bleeding who received no therapeutic intervention according to the video capsule endoscopy findings.
Clinical information of rebleeding cases in the video-capsule-endoscopy-positive antithrombotic drug users who received no therapeutic intervention.
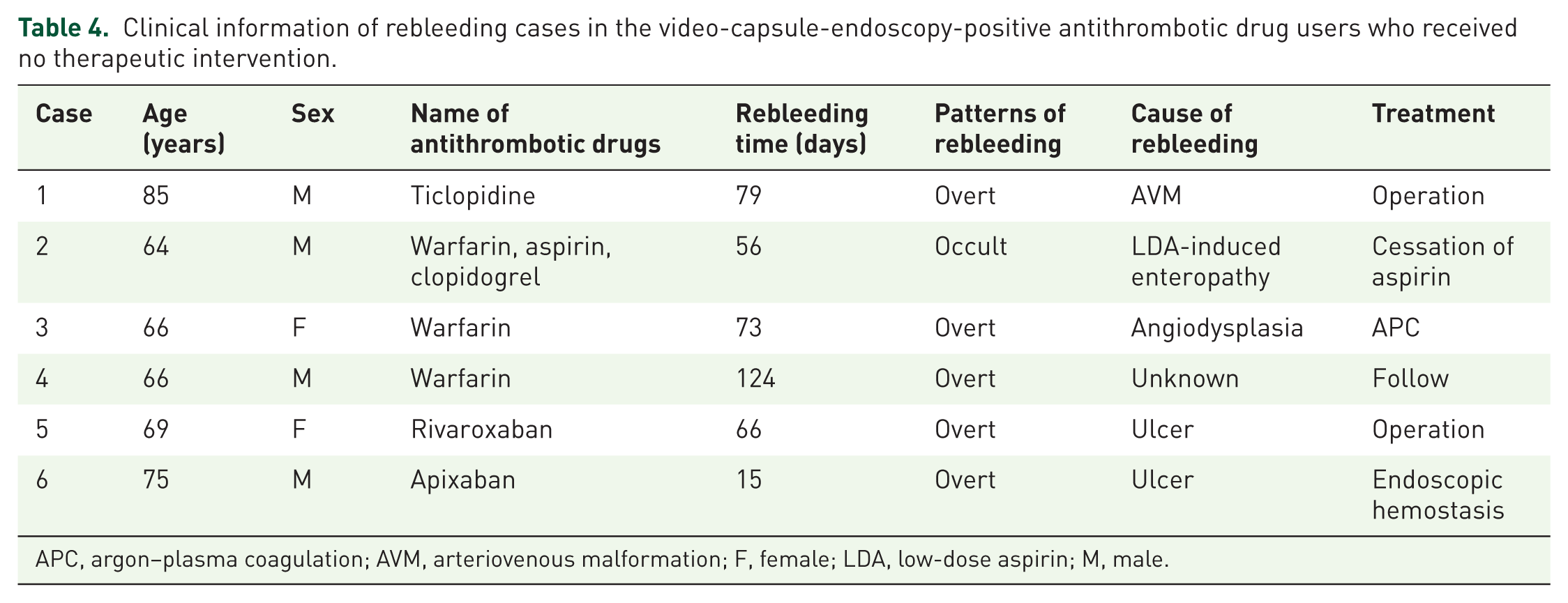
APC, argon–plasma coagulation; AVM, arteriovenous malformation; F, female; LDA, low-dose aspirin; M, male.
Figure 6 shows the rate of rebleeding among the patients with occult OGIB who received no therapeutic intervention according to their VCE findings. Among the antithrombotic drug users, the rates of rebleeding among the VCE-positive and VCE-negative patients did not differ to a statistically significant extent (25% versus 4.0%, p = 0.26). Among the antithrombotic drug nonusers, there were no cases of rebleeding.

The rate of rebleeding among the patients with occult obscure gastrointestinal bleeding who received no therapeutic intervention according to the video capsule endoscopy findings.
The clinical outcomes
As shown in Table 2, there were 22 cases of rebleeding (12%) in total. One patient received interventional radiology, and four patients underwent surgery for hemostasis; they all had good clinical outcomes. Only 6 of 63 (9.5%) antithrombotic drug users ceased taking antithrombotic drugs after the bleeding event; however, there were no thrombotic complications.
Discussion
This study demonstrated the risk of rebleeding in OGIB patients according to their use of antithrombotic drugs. Among the antithrombotic drug users, the rate of VCE positivity was significantly higher among the patients with overt OGIB than it was among those with occult OGIB, and the rate of rebleeding in the patients with overt OGIB who were VCE positive was significantly higher in comparison with that in the patients who were VCE negative. Patients with overt OGIB who were VCE positive and who used antithrombotic drugs had a greater risk of rebleeding; these factors are a good indication for a VCE survey and therapeutic intervention. Among the patients with occult OGIB who were antithrombotic drug nonusers, the risk of rebleeding was quite low regardless of the VCE findings, and no therapeutic intervention was required.
Based on the results of this study, we suggest that patients with OGIB should be managed according to the pattern of OGIB and their use of antithrombotic drugs (Figure 7). We recommend therapeutic intervention for patients with overt OGIB who are VCE positive because of their high risk of rebleeding, especially if they use antithrombotic drugs. On the other hand, no therapeutic intervention is needed among patients with occult OGIB who are VCE negative and who do not use antithrombotic drugs because rebleeding rarely occurs in such cases. Although the difference was not statistically significant, the rate of rebleeding was relatively high among patients with overt OGIB who were VCE positive and antithrombotic drug nonusers, and among patients with occult OGIB who were VCE positive and antithrombotic drug users. Careful follow up should be needed for such cases. We propose following these patients every 2 or 3 months with a blood test, and by performing an endoscopic examination such as VCE or BAE if the patients have anemia, or symptoms of melena or hematochezia.

A flowchart of the treatment strategy for the patients with obscure gastrointestinal bleeding (OGIB) according to the patterns of OGIB and the use of antithrombotic drugs.
With regard to the management of patients with overt OGIB who are antithrombotic drug nonusers and patients with occult OGIB who use antithrombotic drugs, the rate of rebleeding among the VCE-positive patients was relatively higher in comparison with the VCE-negative patients, despite the fact that the difference was not statistically significant. They may have a similar risk of rebleeding, and may require careful follow up or therapeutic intervention. However, the number of cases was small, and further study will be needed to clarify this issue.
There have been few studies on the clinical characteristics of OGIB patients during antithrombotic drug therapy. Shiotani and colleagues reported that the incidence of erosion and ulcers was significantly higher among patients with OGIB whose combination treatment included aspirin. 19 Our study showed that the incidence of erosive lesions in antithrombotic drug users and antithrombotic drug nonusers did not differ to a statistically significant extent. One reason for this was that not all of the patients in our study received aspirin, which may induce small intestinal injuries.
Several studies have suggested that the diagnostic yield in patients with overt OGIB is significantly higher in comparison with that in patients with occult OGIB;20,21 others have suggested that there were no significant differences between the two groups.22,23 In our study, the incidence of VCE positivity in patients with overt OGIB and occult OGIB did not differ to a statistically significant extent (32% versus 21% p = 0.13). The controversy resulted from the different definitions of VCE positivity in these studies. As for the diagnostic yield of VCE in the patients with OGIB during antithrombotic drug therapy, Boal Carvalho and colleagues reported that anticoagulants, but not antiplatelets, were associated with a significantly higher prevalence of P2 lesions in the small bowel. 24 Our study indicated different results, in that during antithrombotic drug therapy, the diagnostic yield of VCE in patients with OGIB depended on the pattern of OGIB.
There have been some reports on the risk factors for rebleeding in patients with OGIB. Koh and colleagues recently reported that there was a significant risk increase of rebleeding in patients who underwent VCE for OGIB while receiving anticoagulant therapy; 5 Kim and colleagues analyzed the risk factors for rebleeding in VCE-negative patients and identified warfarin use as an independent risk factor. 13 Our study did not show that the use of antithrombotic drugs was a risk factor for rebleeding, but demonstrated that patients with overt OGIB who were VCE positive and who used antithrombotic drugs had a greater risk of rebleeding, especially if they received no therapeutic intervention. This was an innovative insight in comparison with previous reports.
The present study is associated with some limitations. First, it was a retrospective, single-center study, and the sample size was not sufficient, especially with regard to the population of antithrombotic drug users. Second, some patients who were VCE positive did not undergo a specific treatment because of spontaneous hemostasis. They could have been at risk of rebleeding; thus, this might have influenced the rate of rebleeding. Third, some patients were followed up at other hospitals after finishing the survey in our hospital.
In conclusion, the clinical features of OGIB patients differed according to their antithrombotic drug use. Since overt OGIB patients who were VCE positive and who used antithrombotic drugs had a greater risk of rebleeding, therapeutic intervention should be considered. The patterns of OGIB and the use of antithrombotic drugs are important for treatment strategies to manage patients with OGIB.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.