
Abstract
Background
Retention is the most common complication of capsule endoscopy (CE), and is reported to occur in 0–13% of cases. To avoid retention, a PillCam patency capsule (PC) is used in patients with suspected intestinal stenosis. However, a relatively low positive predictive value of the PC examination has been reported previously. The aims of this study were to clarify the accuracy of PC examination and to evaluate clinical factors related to cases of false-positive detection.
Methods
We performed a retrospective single-center study of 282 consecutive patients referred for PC examination. Patients in which the PC could not pass through the small bowel within 33 h were classified into the ‘no patency’ group. The ‘no patency’ group was investigated for evidence of significant stenosis upon further examinations, including CE, double-balloon endoscopy, and small bowel follow-through after PC examination. Clinical factors related to small bowel patency and false-positive cases were evaluated.
Results
We included 161 male (57.1%) and 121 female (42.9%) patients with a mean age of 47.5 ± 17.7 years. Of the 282 patients enrolled, 27 patients exhibited ‘no patency’ upon PC examination. Multivariate analysis showed that clinical factors related to ‘no patency’ included Crohn’s disease, abdominal symptoms, stenosis upon imaging, and previous abdominal surgery. Upon further examination, nine cases in the ‘no patency’ group had significant stenosis. Sensitivity, specificity, and negative and positive predictive values of PC examination for detecting small bowel stenosis were 93.8%, 96.6%, 99.6%, and 62.5%, respectively, and the only clinical factor related to false-positive cases was constipation (p < 0.05).
Conclusion
We found a relatively low positive predictive value of PC examination and that constipation was related to false-positive results. To extend the implications of CE indications, clinical study focusing on these results is expected.
Introduction
With the introduction of capsule endoscopy (CE), the entire small bowel can be evaluated at one time relatively easily and non-invasively. The usefulness of CE for investigating obscure gastrointestinal (GI) bleeding, polyposis syndromes, and for diagnosing patients with diarrhea, including suspected Crohn’s disease and celiac disease, has been demonstrated. 1 – 6 The retention of the capsule in patients with intestinal stenosis, which is reported to occur in 0–13% of the cases, is the most common complication of CE. Therefore, known and suspected small intestinal stenosis is a contraindication for CE. The definition of retention is when the capsule is left in the small bowel for longer than 2 weeks after ingestion, which may require endoscopic or surgical removal. 2 , 7 – 11 It was reported that the risk of retention is increased in patients with the following factors: a history of Crohn’s disease, long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs), abdominal surgery, and radiation therapy. 12
The PillCam patency capsule (PC) is a soluble capsule consisting of lactose and 10% barium, and is used prior to CE for patients with suspected intestinal stenosis to evaluate the patency of the small bowel and avoid capsule retention. It has been reported that small bowel follow-throughs (SBFTs) and CT scans could not detect intestinal stenosis accurately, 7 , 9 , 13 – 15 and PC examination was superior to those examinations. 16 This modality is useful to reduce the risk of capsule retention 15 , 17 – 19 and expand the indication of CE to all cases of small intestinal disease.
In the official recommendation from the company, the definition of patency of the small bowel is that PC is passed out of the body within 33 h or observed in the colon on a radiograph or CT scan at least 30–33 h after being swallowed. All other cases in which the PC is observed in the small bowel are not considered patent and are contraindicated for CE.
According to this criterion, we had some patients who were determined to have no indication for CE by the results of PC in spite of having no stenosis in the GI tract. A relatively low positive predictive value of PC examinations has been previously reported, 20 but there have not been enough reports to discuss PC examination from this aspect. The aim of this study was to clarify the rate of significant stenosis in cases that were determined to be ‘not patent’ on PC examination, to evaluate clinical factors related to false-positive cases of PC examination by retrospectively investigating findings on additional examinations, and to suggest management of those cases.
Methods
Patients
In Nagoya University Hospital, 288 consecutive patients who underwent PC examination (PillCam® PC, Covidien Japan Inc., Tokyo, Japan) prior to CE (PillCam® SB2plus/SB3, Covidien Japan Inc., Tokyo, Japan) between January 2010 and December 2015 were enrolled.
PC indication and procedure, definition of confirmation of patency and no patency
Our indications for PC evaluation were as follows: known or suspected Crohn’s disease; long-term use of NSAIDs; a history of small bowel ileus; abdominal symptoms suspected to be related to intestinal stenosis, including fullness and pain after meals; stenosis suspected on SBFT or CT scan; history of abdominal surgery; chronic inflammatory diseases including radiation enteritis; and known small bowel tumor. ‘History of abdominal surgery’ included intestinal resection, gynecologic surgery, and other surgeries that can cause stenosis on anastomosis or passing failure due to postoperative adhesion. Details of surgical history were intestinal resection (126), gynecologic surgery (11), surgery for peritonitis caused by severe cholecystitis and appendicitis (9), and surgery for abdominal injury (1). ‘Stenosis on SBFT or CT scans’ included stenosis that was suspected to be too severe to be passed by CE on the basis of the SBFT and CT scan findings, including narrowing of the lumen with wall thickening or edematous change and dilatation of the intestinal diameter suggestive of intestinal obstruction. Findings that were indicative of slight stenosis were not considered.
According to health insurance coverage in Japan, contraindications to CE were patients who had known small bowel stenosis, which were thought to result in capsule retention, patients with pacemakers or other implanted electromedical devices, patients with swallowing disorders, and patients who were allergic to barium.
Patients did not undergo special bowel preparation nor did they take any medicine to motivate or slow down their bowel mobility specifically for this procedure. Sixteen patients who regularly used medications to regulate bowel motility continued their medication while undergoing PC examination. There was no limitation to having food and drink before and after PC ingestion. In accordance with official recommendations, patients who excreted the PC within 33 h and those who retained the PC in their colon were classified in the ‘confirmation of patency’ group, while all others were placed in the ‘no patency’ group. For patients who did not excrete the PC within the timeframe, radiographs were first acquired to confirm the location of the PC. If we could not clearly confirm the location from the radiograph alone, CT scans were performed (Figure 1).

Determination of presence of patency on patency capsule (PC) examinations. Xp: X-ray photography; CT: computed tomography.
Definitions and evaluations
The following clinical factors were screened among patients scheduled to undergo CE and investigated from their medical records retrospectively: abdominal symptoms, a history of surgery, age, sex, BMI, use of prokinetics, constipation, activities of daily living (ADLs), and stenosis on imaging. Abdominal symptoms were defined as any symptoms that made us suspect intestinal stenosis, such as abdominal pain and bloating after meals. A low ADL was defined as bedridden patients for a poor general condition. Constipation was defined as patients who did not defecate over 2 days without medication or regular use of prokinetics to motivate intestinal movement. In patients whose GI patency could not be established, further examinations using other modalities were usually performed.
Clinically significant stenosis was defined as a case in which double-balloon endoscopy (DBE, EN-580T or EN-450P5, Fujifilm Co., Tokyo, Japan) could not pass through the stenosis, the capsule was retained in front of the stenosis, and the stenosis induced dilatation of the oral side of the intestine. If even one of their stenoses met the criteria, the patients were defined as having significant stenosis. ‘No stenosis’ was defined as patients who have none of the findings described above and no occurrence of small bowel obstruction for at least 6 months after evaluation.
The primary endpoint was the factors related to false-positive rates on PC tests. The secondary endpoint of this study was the accuracy of PC examination for detecting small bowel stenosis. This study was approved by the ethics committee of Nagoya University Hospital (IRB No. 2015-0485). The ethics committee does not require informed consent for inclusion in retrospective studies. However, the study details were posted on the Nagoya University Hospital website and on the display board of the Department of Gastroenterology of Nagoya University Hospital from April 2016 to May 2017.
Statistical analysis
SPSS for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Univariate and multivariate logistic regression analyses were used to analyze factors related to the presence of patency and false-positive rates in the ‘no patency’ group. The Mann–Whitney U test and chi-squared test were used in univariate analysis. p-value <0.05 was determined to be statistically significant.
Results
Of the 288 patients who were enrolled, six patients were excluded because an evaluation of their PC location was not completed within 30–33 h. Table 1 shows the characteristics of the subjects. The subjects comprised 161 men (57.1%) and 121 women (42.9%) with a mean age of 47.5 ± 17.7 years and a mean BMI of 20.4 ± 2.8 kg/m2. Indications for CE were history of abdominal surgery (50.7%), Crohn disease (44.7%), abdominal symptoms suspected to be related to bowel stenosis (30.1%), suspected stenosis on SBFT or CT scans (21.6%), and others. Of the 282 patients, 152 (53.9%) secreted an intact PC within 33 h of ingestion. The other 130 patients underwent abdominal-pelvic radiographic examination and/or a conventional radiation abdominal-pelvic CT scan without contrast; the PC reached the colon in 103 cases on radiograph or CT. We defined these 255 cases as the ‘confirmation of patency’ group, and the other 27 cases that had their PCs still in the small bowel as the ‘no patency’ group (Figure 1).
Characteristics of subjects (n = 282).

BMI, body mass index; NSAIDs, nonsteroidal anti-inflammatory drugs; PC, patency capsule; SBFT, small bowel follow-through.
Clinical factors related to ‘no patency’ group
We analyzed which factors significantly affected GI patency. Univariate analysis showed that Crohn’s disease, abdominal symptoms, stenosis on imaging, constipation, low ADL, and previous abdominal surgery were related to ‘no patency’ classification. Multivariate analysis showed Crohn’s disease, abdominal symptoms, stenosis on imaging, and previous abdominal surgery were statistically significant factors (Table 2).
Clinical factors related to ‘no patency’ group.
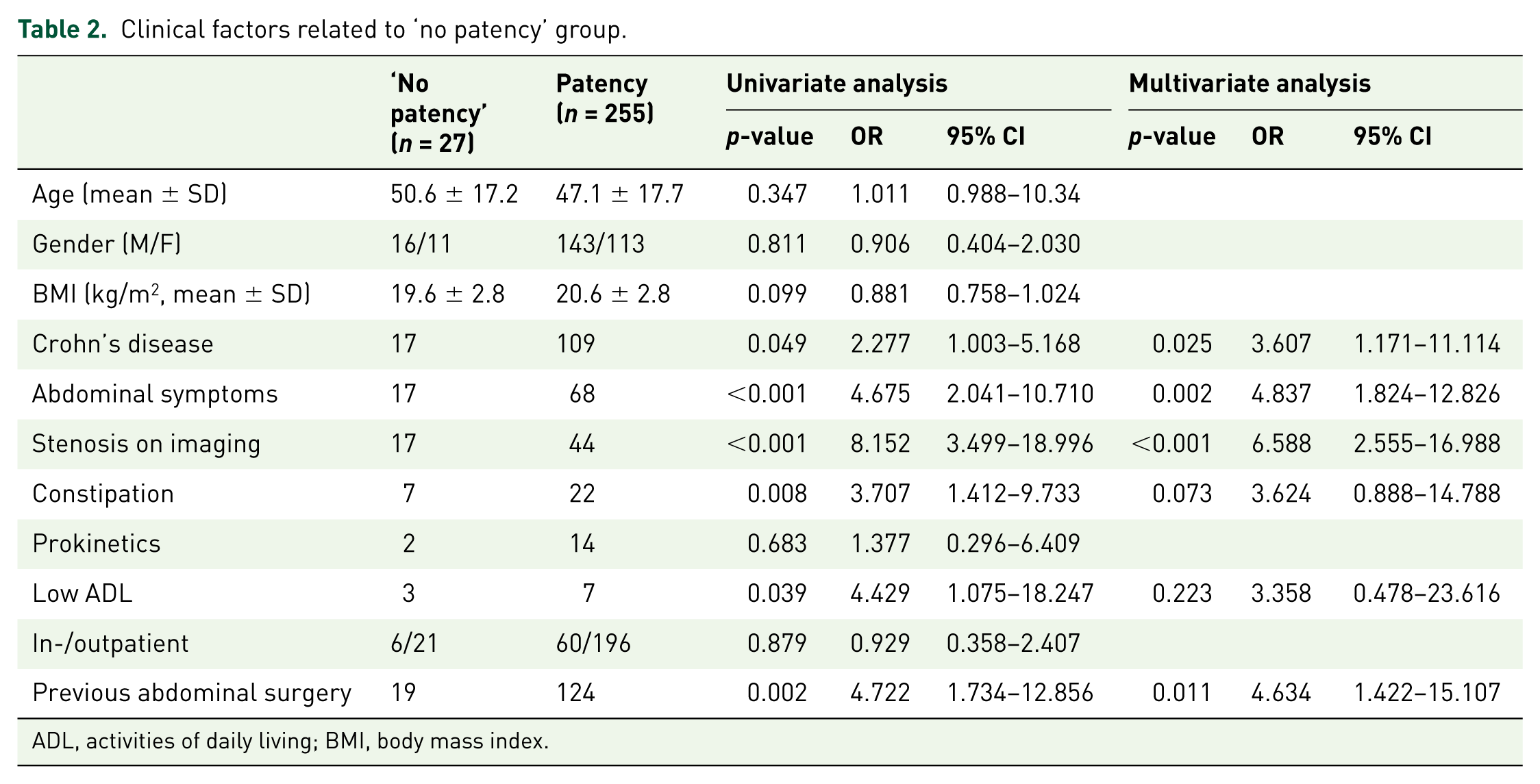
ADL, activities of daily living; BMI, body mass index.
Further examination and diagnosis of the small bowel in the ‘no patency’ group
Table 3 shows the characteristics of the ‘no patency’ group. The subjects comprised 16 men (59.3%) and 11 women (40.7%) with a mean age of 50.6 ± 17.2 years and mean BMI of 19.6 ± 2.8 kg/m2. Indications for CE included a history of abdominal surgery (70.4%), Crohn disease (63.0%), abdominal symptoms suspected to be related to bowel stenosis (63.0%), suspected stenosis on SBFT or CT scans (63.0%), and others. In the ‘no patency’ group, the modalities for further examinations of the small bowel were DBE in 10 patients, SBFT in eight patients, and CE in six patients. The mean duration between PC and these examinations was 11.5 ± 12.9 days. Three patients did not agree to undergo any additional examinations. Table 4 shows the small bowel diagnosis and treatment of these cases. Six patients who underwent CE had agreed to participate in another clinical study. In that study, CE could be chosen for patients who excreted an intact PC within 72 h after swallowing the PC, even if the PC was found in their small bowel or if the PC was not assessed for location at 30–33 h. Accordingly, six patients underwent CE, and none of them experienced any CE-related complications, including retention. Total small bowel observation was not possible in one of the six patients (total rate of small bowel observation, 83.3%). Four of the six patients had constipation. The mean gastric transit time and small bowel transit time in the five patients in whom total small bowel observation was possible were 23.2 ± 9.5 min and 271 ± 56.3 min (mean ± SD), respectively (Table 5).
Characteristics of ‘no patency’ group (n = 27).

BMI, body mass index; NSAIDs, nonsteroidal anti-inflammatory drugs; SBFT, small bowel follow-through.
Further small bowel examinations and outcome in 24 patients in the ‘no patency’ group (n = 24).*

Except for three patients without any further examination for small bowel after PC examination, including double-balloon endoscopy, SBFT, or CE.
Patients who excreted an intact PC body 33–72 h after swallowing the PC.
CE, capsule endoscopy; EBD, endoscopic balloon dilation; SBFT, small bowel follow-through.
Details of further small bowel examinations of patients with ‘no patency’ without small bowel stenosis.
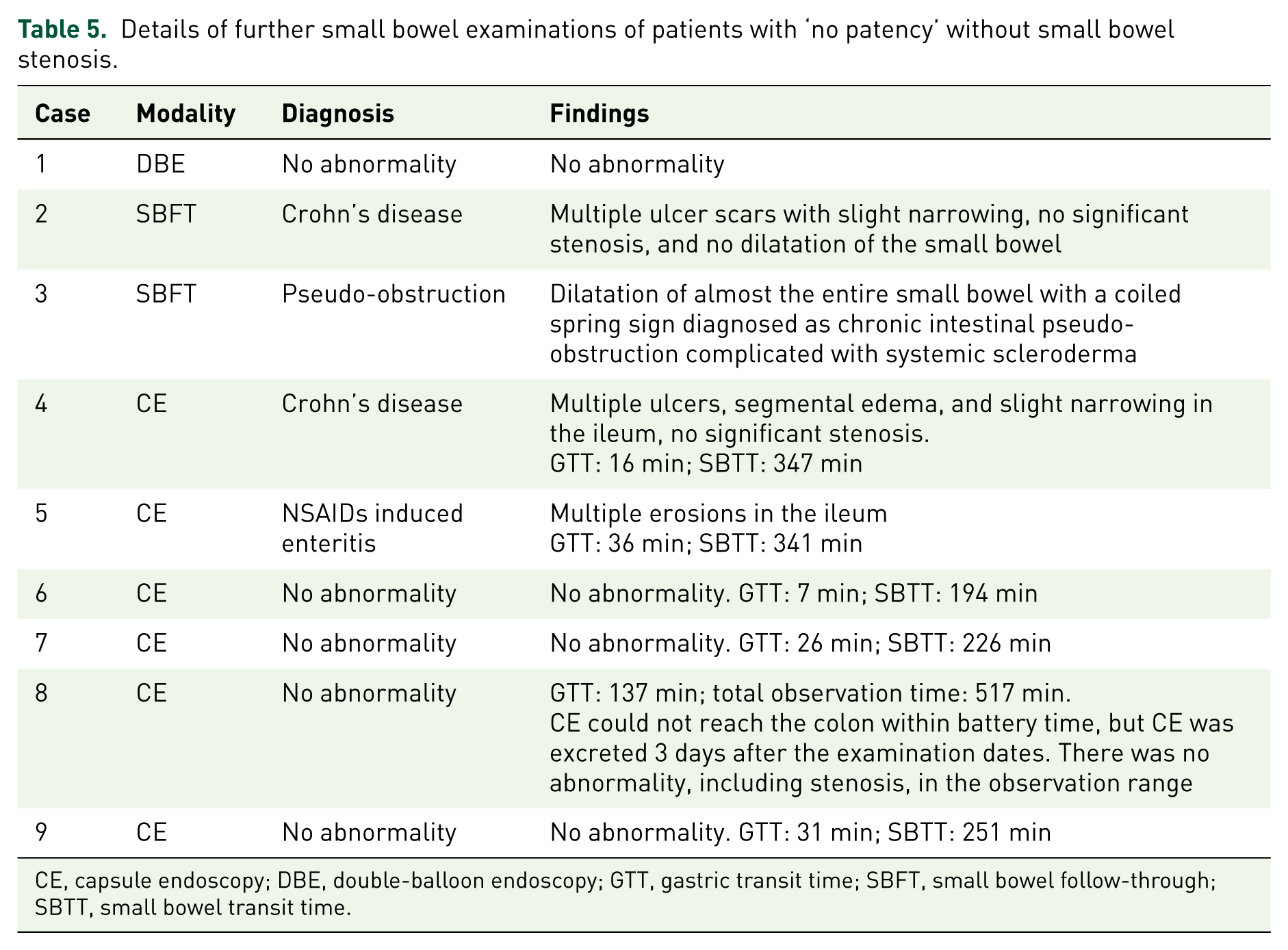
CE, capsule endoscopy; DBE, double-balloon endoscopy; GTT, gastric transit time; SBFT, small bowel follow-through; SBTT, small bowel transit time.
Of the 24 cases that underwent further examination, 15 cases were detected to have significant small bowel stenosis and the remaining nine cases had no stenosis. The small bowel diagnoses of the stenosis group were Crohn’s disease (12), malignant lymphoma (1), ischemic enteritis (1), and small bowel tuberculosis (1). Nine of these cases required surgical treatment or endoscopic balloon dilation for the stenosis.
Table 5 shows the diagnosis and findings of subsequent small bowel examinations in nine patients in the ‘no patency’ group. Five of these nine patients had no abnormality. Two patients with Crohn disease had multiple ulcers, erosions, and slight narrowing of the small bowel. Patients with systemic scleroderma had dilated small bowels and the coiled spring sign, which indicated chronic intestinal pseudo-obstruction. One patient had multiple erosions in the ileum and was diagnosed with NSAID-induced enteritis due to previous drug-use history, but had no significant stenosis.
Accuracy of PC examination for stenosis
CE was performed in all patients with confirmed GI patency, and we experienced one case of retention. The patient had a history of Crohn’s disease, abdominal surgery, abdominal pain, and stenosis on CT. Since PC was excreted out of the body within 30 h, CE was performed 7 days later. After the endoscopic capsule was retained, we performed DBE and successfully retrieved the capsule. The patient had multiple ulcers and fibrotic stenosis in the pelvic ileum. The sensitivity, specificity, and negative and positive predictive value of the PC examination for detecting small bowel stenosis were 93.8%, 96.6%, 99.6%, and 62.5 %, respectively (Table 6).
Accuracy of PC examination for stenosis (n = 279).*
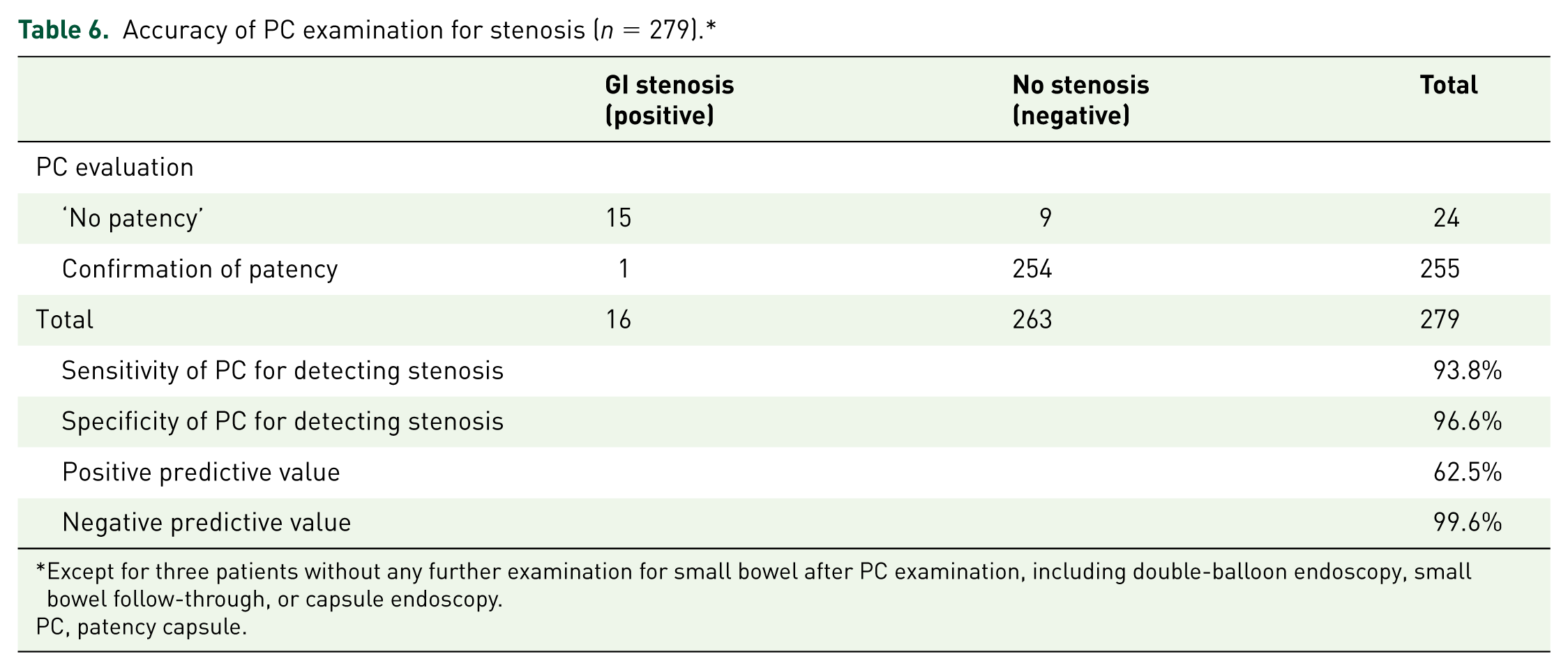
Except for three patients without any further examination for small bowel after PC examination, including double-balloon endoscopy, small bowel follow-through, or capsule endoscopy.
PC, patency capsule.
Clinical factors related to false-positive cases on PC examination
Table 7 shows the univariate and multivariate analyses of the factors related to cases without significant stenosis in the ‘no patency’ group on the PC test. Univariate analysis indicated that Crohn’s disease and constipation were related, while multivariate analysis showed constipation was the only significant factor.
Clinical factors related to false-positive cases in the ‘no patency’ group (n = 24).*

Except for three patients without any further examination for small bowel after PC examination, including double-balloon endoscopy, small bowel follow-through, or capsule endoscopy.
ADL, activities of daily living; BMI, body mass index.
Discussion
Several reports have indicated the safety and usefulness of a PC examination prior to CE. 5 , 17 , 18 In terms of accuracy in detecting significant small bowel stenosis, it has been demonstrated that the sensitivity of PC examination was superior to other examinations. 21 , 22 In contrast, there have been a few reports about the false-positive cases of the PC tests. Yadav and colleagues reported that the positive predictive value of PC was relatively low (44%). In their study, four of nine patients with a positive PC examination were surgically confirmed to have stricture, while all of the other five patients underwent CE without retention. Three of these five patients had normal CE findings. 20 However, it has been unclear which diseases and factors are related to those false-positive cases.
In the present study, we investigated the findings and diagnoses on further examinations of the small bowel in patients in the ‘no patency’ group and found that nine of 24 cases (37.5%) had no significant stenosis. This results in a low positive predictive value (62.5%) of the PC evaluation for detection of severe intestinal stenosis. In other words, it meant that some cases in the ‘no patency’ group, according to the present criteria, could still undergo CE. Actually, six cases did undergo CE. The other three cases showed no significant stenosis on DBE or SBFT and were candidates to be able to undergo CE.
To avoid unnecessary and invasive examinations, we thought it important to determine the reason for the low positive predictive value of PC examination and to suggest a method to improve it. Therefore, we investigated the factors that affected significant intestinal stenosis in the ‘no patency’ group. Univariate analysis indicated that Crohn’s disease and constipation were related factors, while multivariate analysis indicated constipation alone. In cases with constipation, it is possible that the low activity of intestinal movements prevents excretion of the PC within the limited time, even if there is no severe stenosis. As intestinal passage time is different between individuals, 23 the 30–33 h cutoff may be too short to evaluate the GI patency for patients with constipation. Although there was no significant difference statistically, female patients, hospital patients, and low ADL patients were relatively more frequent in the ‘no stenosis’ group. There is a possibility that those factors are related to a delayed passage time in the intestine. Thus, we considered the difference of intestinal passage time between individuals as a critical reason for the low positive predictive value of PC examinations. We identified two possible ways to improve it.
One idea is to extend the evaluation time to 60–72 h after swallowing the PC. In this study, we had performed CE for six cases whose PC was evaluated in the small bowel at 30 h or no evaluation of PC location was completed, but these patients excreted an intact body PC within 72 h. All of these patients were evaluated by CE and no complications occurred, including retention. Several articles have described patients that underwent CE who excreted the intact body of the PC within 60–72 h, and only a few cases of retention occurred. 18 , 24 In these previous reports, since the advancement of the PC was not evaluated at 30–33 h, the PC might already have reached the colon at that point. In this study, the PC was confirmed to exist in the small bowel at 30–33 h. It implies that decreased activity of the small bowel and/or gastric movement led to a delayed passage time of the PC and then the PC was in the small bowel at the evaluation period. Therefore, another idea to be considered is to use prokinetics or cleansing agents to improve GI tract mobility. With the use of these medicines, the passage time of the PC in the small bowel will be shorter and may reduce the false-positive case of PC examination.
These two ideas may improve the low positive predictive value of PC examinations and may be able to reduce radiographic examinations by increasing the rate of intact body excretion. However, there is not yet sufficient data of their usefulness and safety and no consensus about which type of medicine to use. Clinical studies to resolve these clinical points are expected.
As described previously, PC examination has good sensitivity and specificity for detection of small bowel stenosis. However, it can cause some complications such as abdominal pain, small bowel obstruction, and retention in patients who have particularly tight stenoses. 16 , 25 In fact, we experienced two cases of retention of the coating shell of the PC, and endoscopic removal was required. Therefore, we have to be careful not to perform PC examination in patients with especially tight stenoses, who may retain the PC. However, studies to detect such stenoses before PC examination have scarcely been reported. In recent studies, transabdominal ultrasonography (US) has been shown to have a high accuracy for detecting stenosis related to Crohn’s disease, and the findings of US have a good relationship with intraoperative findings. 26 , 27 In the future, US may become an option to detect stenosis in a noninvasive manner, although more studies are needed to confirm this.
Limitations of this study include a single-center, retrospective study design and a relatively small sample size of the ‘no patency’ group. Not all of the patients in the ‘no patency’ group agreed to undergo further examination of the small bowel. Although there were no patients who had symptoms that made us strongly suspect gastroparesis, we did not evaluate gastroparesis formally as a factor to extend transit time and increase the false-negative rate. We used local criteria to determine PC/CE indication.
In conclusion, this study demonstrated a low positive predictive value of PC tests for detection of small bowel stenosis. In the ‘no patency’ group, constipation was related to false-negative cases. A modified PC procedure to safely extend the indication of CE is expected for the management of the ‘no patency’ group.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.