
Abstract
Background:
Upper gastrointestinal bleeding (UGIB) accounts for 400,000 hospital admissions in the US each year. Despite advances, mortality rates remain high and are estimated to be 5–10%. Early therapeutic endoscopy is widely recommended as a means of reducing morbidity and mortality. The Rockall and Blatchford scores are clinical scoring systems devised to assist in risk stratifying patients with UGIB. In a prior study we found that rapid live bedside video capsule endoscopy (VCE) utilizing Pillcam ESO® correctly identified patients with high-risk stigmata of bleeding seen on upper endoscopy. In this study, we compare the accuracy of the Rockall and Blatchford scores with Pillcam ESO® in predicting high-risk endoscopic stigmata.
Methods:
Pre-endoscopy Blatchford and Rockall scores were calculated for 25 patients (14 males, 11 females) presenting to the emergency room with acute UGIB. The average patient was 66 years of age. A total of 24 out of 25 patients underwent upper endoscopy within 24 hours. One patient did not undergo endoscopy due to clinical instability. The timing of endoscopy was based on clinical parameters in 12 patients, and on live view VCE with Pillcam ESO® in the other 13 patients. Positive VCE was defined as red blood, clot or coffee grounds. Mean Rockall and Blatchford scores for all 24 patients were compared to determine potential differences between high- and low-risk patients. Rockall and Blatchford scores were also compared with VCE findings.
Results:
Of 24 patients, 13 had high-risk stigmata on upper endoscopy. The mean Rockall and Blatchford scores were 3 and 13, respectively. In the 11 patients without stigmata, the mean Rockall and Blatchford scores were 2 and 11, respectively. There was no statistically significant difference between the Blatchford scores of the two groups (95% confidence interval [CI] −5.1 to 1.3; p = 0.22). There was no statistically significant difference between the Rockall scores of the two groups (95% CI −2.3 to 0.3; p = 0.11). In the subgroup of 12 patients who underwent VCE prior to endoscopy, 8/12 had positive findings, which were all confirmed at endoscopy. All 4 patients with negative VCE had no high-risk stigmata at endoscopy.
Conclusion:
In emergency room patients with acute UGIB, neither the Rockall nor the Blatchford scores were able to differentiate high- and low-risk patients identified at endoscopy. Live view VCE, however, was accurate in predicting high-risk endoscopic stigmata, and may be better suited as a risk stratification tool. Additional studies with a larger cohort will be required to validate these findings.
Keywords
Introduction
Upper gastrointestinal bleeding (UGIB) accounts for 400,000 hospital admissions in the US each year. The most common source of nonvariceal hemorrhage is peptic ulcer disease. Despite advances, mortality rates remain high and are estimated to be 5–10% [Lewis et al. 2002; Gralnek et al. 2008]. Early therapeutic endoscopy is widely recommended as a means of reducing morbidity and mortality [Gralnek et al. 2008; Chiu and Ng, 2009]. Identifying high- and low-risk patients with acute UGIB enables appropriate triage to urgent endoscopy.
Historically, nasogastric tube (NGT) aspiration with lavage in conjunction with clinical assessment has been used to risk stratify patients with UGIB. However, the sensitivity of NGT has been reported as low as 42%, thereby limiting its usefulness as a risk stratification tool [Pitera and Sarko, 2010]. A negative nasogastric tube aspiration (no blood or coffee grounds) does not rule out gastrointestinal bleeding. In fact, 15% of these patients have high-risk lesions on endoscopy [Gralnek et al. 2008]. Its associated risks include epistaxis, aspiration, pneumothorax, and perforation [Pitera and Sarko, 2010]. As noted by Pitera and Sarko, a diagnostic test is most helpful when it is simple, accurate, and directs management [Pitera and Sarko, 2010].
The Blatchford [Blatchford et al. 2000] and Rockall [Rockall et al. 1996] scores are clinical scoring systems devised to assist in risk stratifying patients with UGIB. The Blatchford score was designed to predict which patients require clinical intervention (blood transfusion, endoscopy, or surgery), whereas the Rockall score focuses on rebleeding and mortality prediction. The risk of rebleeding and the mortality rate increases as the score increases. Both scoring systems have been previously validated in prior studies [Stanley et al. 2009; Vreeburg et al. 1999].
The Blatchford score assigns points to measures of systolic blood pressure, blood urea nitrogen (BUN), hemoglobin, and other variables, such as pulse, melena, syncope, hepatic disease, and cardiac failure. A possible Blatchford score ranges from 0 to 23, with higher scores indicating higher risk. Patients with a Blatchford score of greater than 0 are considered to require clinical intervention [Blatchford et al. 2000].
The clinical Rockall score assigns points to the variables of age, shock (heart rate and systolic blood pressure), and coexisting illness, including ischemic heart disease, congestive heart failure, renal failure, hepatic failure, or metastatic cancer. The maximum additive score is 7. Patients with a clinical Rockall score of greater than 0 are considered to be at high risk for adverse outcomes [Rockall et al. 1996]. A complete Rockall score incorporates endoscopic diagnosis and endoscopic stigmata of recent hemorrhage, for a possible maximum score of 11.
In a prior study we found that rapid live bedside video capsule endoscopy (VCE) utilizing Pillcam ESO® correctly identified patients with high-risk stigmata of bleeding confirmed on upper endoscopy [Rubin et al. 2011]. In this study, we assess the predictive value of the Rockall and Blatchford scores compared with Pillcam ESO® in predicting high-risk endoscopic stigmata.
Methods
The pilot Pillcam ESO® bleeding study was a prospective, randomized, controlled clinical trial that enrolled consecutive patients who presented with signs and symptoms of acute UGIB to an urban tertiary care academic hospital [Rubin et al. 2011].The study protocol and informed consent were approved by the hospital’s institutional review board.
Patients were considered eligible for participation if they were 18 years of age or older and had a history suggestive of acute UGIB within 48 hours prior to presentation to the emergency room. UGIB was defined as melena or hematemesis. Patients with maroon stool or rectal bleeding with hemodynamic compromise defined as heart rate greater than 100 beats per minute (bpm), systolic blood pressure less than 100 mmHg or orthostatic hypotension were also included.
Patients were excluded if they had a history of Zencker’s diverticulum, symptoms of dysphagia or odynophagia, suspected bowel obstruction, history of prior bowel obstruction, Crohn’s disease, presence of internal cardiac defibrillator, pregnancy, active hematemesis within 2 hours prior to presentation, or hemodynamic instability defined by systolic blood pressure less than 80 mmHg or heart rate greater than 150 bpm and evidence of active cardiac ischemia.
PillCam ESO 2® is an 11 mm × 26 mm video capsule which weighs less than 4 g and contains an imaging device (CMOS chip) and light source at both ends. It takes 18 images per second for a total of 3400 color images over approximately 30 min. The images are captured onto a data recorder that receives signals via a sensor array that are transmitted by the PillCam ESO® capsule as it passed through the gastrointestinal tract.
All VCE patients received intravenous metoclopramide at enrollment into the study and subsequently underwent live view capsule endoscopy at bedside with a real-time viewer. Three thoracic sensors were placed in a standard pattern and connected to the DR 2® data recorder. The data recorder was attached by USB cable to a Fujitso mini-notebook computer running Rapid Viewer®. Pillcam ESO 2® was administered in a standard fashion [Rubin et al. 2011]. The entire exam was observed live by one of the investigators and reviewed after download by a second investigator. Positive VCE (VCE+) findings were defined as coffee grounds, blood clots, red blood, or a bleeding lesion. VCE+ patients underwent emergent esophagogastroduodenoscopy (EGD) within 6 hours. All control patients and those VCE patients without signs of bleeding (VCE−) underwent endoscopy within 24 hours [Barkun et al. 2003].
In this study we assess the ability of the Rockall and Blatchford scores to predict high-risk stigmata that were identified at VCE and at endoscopy. Pre-endoscopy Blatchford and Rockall scores were retrospectively calculated for all 24 patients. The predictive value of the Rockall and Blatchford scores was assessed by comparing the mean values of patients with and without stigmata at endoscopy.
Statistical analysis
Sensitivity and specificity were calculated for the Rockall and Blatchford Scores. The Spearman correlation coefficient was used to examine the relationship among the Rockall and Blatchford scores and endoscopic and VCE findings. Logistic regression analysis was used to compare the Rockall and Blatchford scores to high- and low-risk endoscopic stigmata. To explore the sensitivity and specificity for a range of thresholds for the Rockall and Blatchford Scores an area under the curve (AUC) was calculated and a p-value determined for the significance of the AUC. An exact version of the McNamar’s test was used to examine the association between the video capsule and the upper endoscopy findings. Means for each group are rounded to the nearest integer as the Rockall and Blatchford scores are commonly expressed as integer values. Mean differences are expressed as 95% confidence intervals (CIs). A p-value less than 0.05 was considered statistically significant. No adjustment was made for multiple testing. All calculations were performed using the statistical package SAS 9.3 (SAS Institute Inc., NC).
Results
Rockall, Blatchford, and endoscopy
A total of 24 sequential patients with signs and symptoms of acute UGIB were randomized in the emergency room into two groups of 12 patients each. There were 14 male and 10 female patients. The average patient was 66 years of age. Patient demographics and baseline characteristics are listed in Table 1. There were no differences in the two groups except for baseline pulse which was 102 beats per minute in the VCE group and 86 in the control group (p = 0.03).
Patient demographics and baseline characteristics.
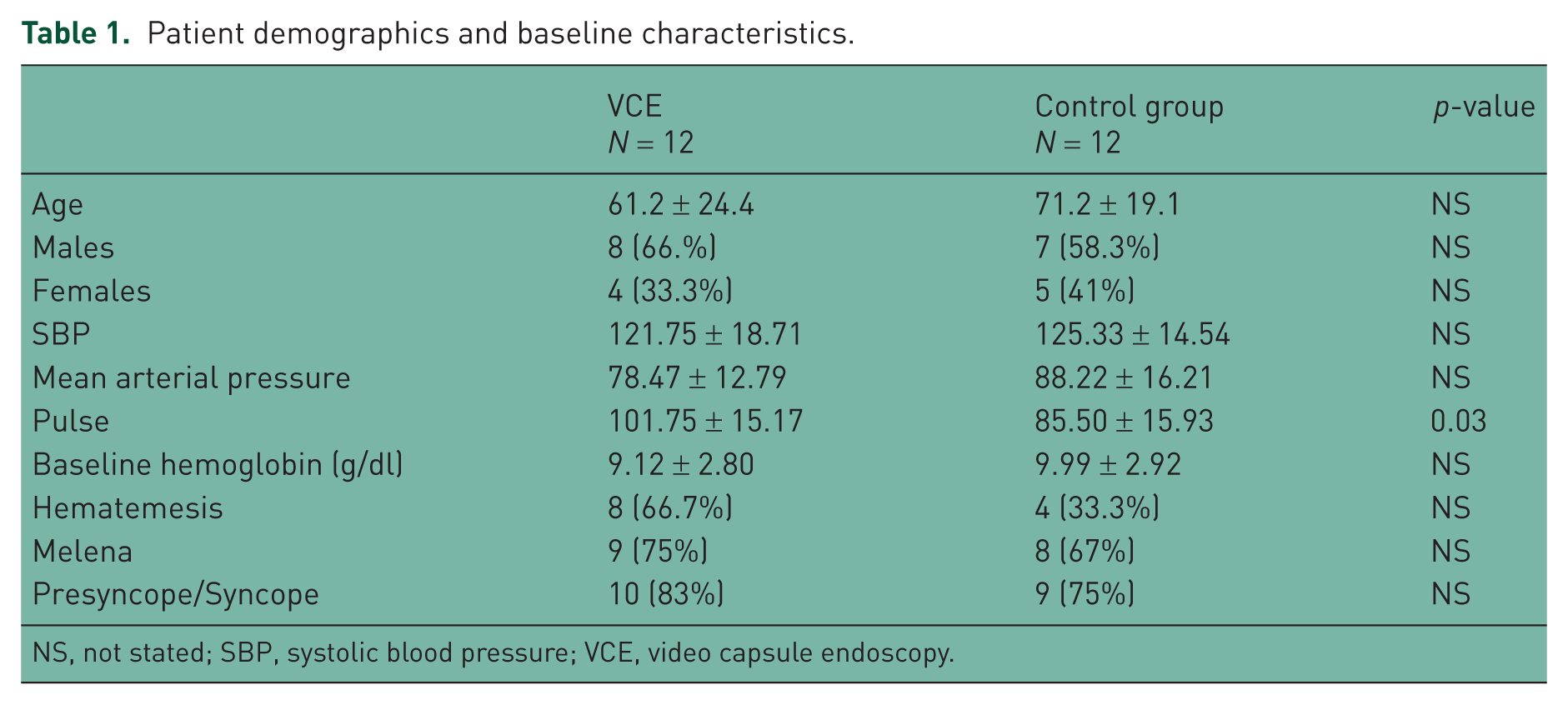
NS, not stated; SBP, systolic blood pressure; VCE, video capsule endoscopy.
Of 24 patients, 13 had high-risk stigmata on upper endoscopy. The mean (rounded to the nearest integer and standard deviation) Rockall and Blatchford scores were 3 (1.5) and 13 (3.1), respectively. In the 11 patients without stigmata, the mean Rockall and Blatchford scores were 2 (1.6) and 11 (4.2) (Figure 1). There was no statistically significant difference between the Blatchford scores of the two groups (95% CI −5.1 to 1.3; p = 0.22).There was no statistically significant difference between the Rockall scores of the two groups (95% CI −2.3 to 0.3; p = 0.11). There was no statistically significant association between Blatchford and EGD (Spearman’s r = 0.28; p = 0.18) or Rockall and EGD (Spearman’s r = 0.35; p = 0.10). There was also no linear association between the Blatchford and Rockall scores (Spearman’s r = 0.33; p = 0.12).
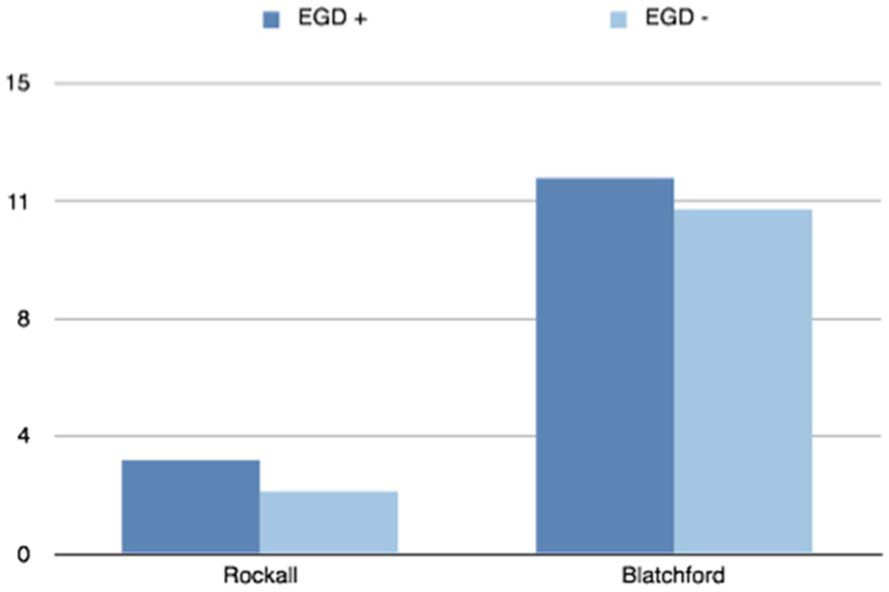
Endoscopy compared to clinical scoring systems.
The sensitivity and specificity of the Blatchford score was 100% and 0%, respectively. The patients who were truly negative for high-risk stigmata on endoscopy were still identified as high risk by the Blatchford score. Among patients with positive or negative EGD results, the Blatchford was not a statistically significant predictor of EGD findings (AUC = 0.66; p = 0.16). The sensitivity and the specificity of the Rockall score was 92.3% and 18%, respectively. Among patients with positive or negative EGD results, the Rockall was not a statistically significant predictor of EGD status (AUC = 0.70; p = 0. 0.07).
Rockall, Blatchford, and VCE
In the subgroup of 12 patients who underwent VCE prior to endoscopy, 8 had positive findings (67.7%), which were all confirmed at endoscopy. An exact version of the McNamar’s test revealed that video capsule data and EGD results were identical (p = 1.00). In this high-risk group, the average Rockall and Blatchford scores were 3 (1.4) and 13 (3.0), respectively. In all four patients with a negative VCE, no high-risk stigmata were seen at endoscopy. For these four patients the average Rockall and Blatchford scores were 1 (0) and 13 (1.0). There was a statistically significant difference in the Rockall scoring system between the positive and negative capsule endoscopy groups (95% CI −3.0 to −0.7; p = 0.01. The lack of variance in the four VCE negative patients makes this result unreliable. There was no statistically significant difference in the Blatchford scoring system between the positive and negative capsule endoscopy groups (95% CI −3.7 to 3.4; p = 0.94 (Table 2).
Endoscopy compared with VCE. An exact version of the McNamar’s test revealed that video capsule data and EGD results were identical, p = 1.00.
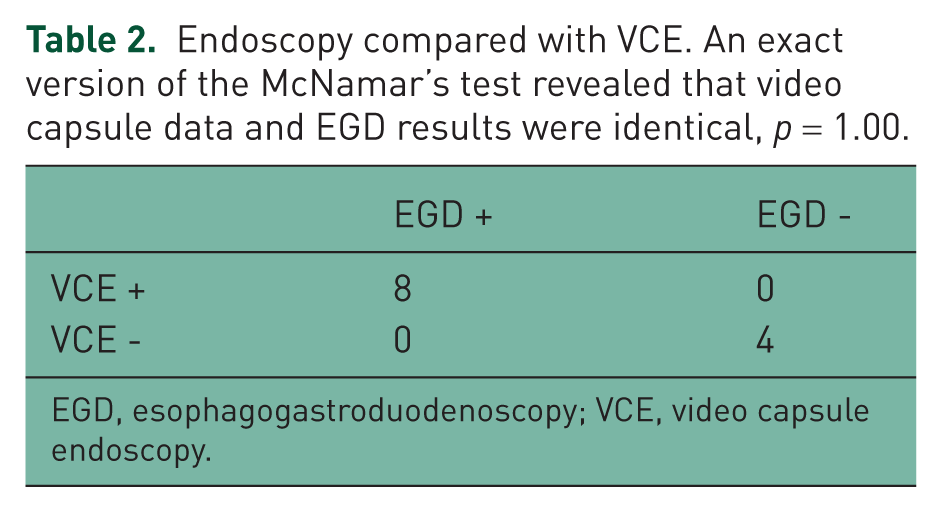
EGD, esophagogastroduodenoscopy; VCE, video capsule endoscopy.
Discussion
UGIB is a common cause of hospital visits and admissions, at a cost estimated as US$2.5 billion annually [Albeldawi et al. 2010]. It carries a mortality of up to 10% [Gralnek et al. 2008]. The patient with UGIB should be promptly resuscitated and plans should be made for urgent endoscopy. To improve the efficiency of this process the evaluation of UGIB would benefit from a risk stratification tool applied on admission. Recognition of the patients that would require urgent versus emergent endoscopy would facilitate timely treatment of the high-risk patients.
In a recent study we demonstrated the ability of live view Pillcam ESO® to identify UGIB patients with high-risk endoscopic stigmata [Rubin et al. 2011]. The Blatchford and Rockall scores, were designed to predict the need for clinical intervention and mortality, respectively, and have been well described in the literature [Blatchford et al. 2000; Rockall et al. 1996; Stanley et al. 2009; Vreeburg et al. 1999; Chandra et al. 2012; Romagnuolo et al. 2007; Pang et al. 2010; Le Jeune et al. 2011; Chen et al. 2007]. In the present study we compared the accuracy of these scoring systems to capsule endoscopy and urgent endoscopy in predicting high-risk stigmata. Our results demonstrate that neither the Rockall nor the Blatchford scores were able to differentiate high- and low-risk patients. Patients without findings of high-risk stigmata on upper endoscopy were deemed high risk by the Rockall and Blatchford clinical scoring systems. There was also no difference between the mean Blatchford and Rockall scores whether the patient was found to have a positive or negative VCE.
In concordance with our results, a recent study by Chandra and colleagues examined the Glasgow–Blatchford and Rockall scores in a US population and found that neither score was sensitive enough to use in clinical practice [Chandra et al. 2012]. A study by Romagnuolo and colleagues found that a clinical Rockall score of one or less (range 0–11) did not predict a lower frequency of endoscopic stigmata, but a Blatchford score of one or less (range 0–23) identified approximately 10% of patients with gastrointestinal tract bleeding with a low likelihood of having high-risk stigmata [Romagnuolo et al. 2007]. A recent study by Pang and colleagues also compared the Blatchford and pre-endoscopic Rockall in the decision to perform therapeutic endoscopy. This study found that the Rockall score was not a useful predictor and the Blatchford score was more useful for predicting low-risk patients, with a threshold score of 0 [Pang et al. 2010]. Our results together with these studies raise serious questions as to the clinical usefulness of these scoring systems.
VCE was clearly sensitive and specific in its ability to differentiate between those patients with high- and low-risk endoscopic stigmata. Our preliminary data suggests that live view VCE, is better suited as a risk stratification tool. In another recent study, Gralnek and colleagues reported the feasibility of using VCE in the triage of patients with UGIB [Gralnek et al. 2011].
A limitation of our study is its small sample size of 24 patients. This number was based on our original pilot study to test the feasibility of using capsule endoscopy to risk stratify UGIB patients in the emergency room. The available data allowed us to compare the gold standard of upper endoscopy with live view VCE and then the clinical scoring systems of Rockall and Blatchford. Additional studies with a larger cohort should be performed to validate these findings.
When describing the perfect diagnostic test Pitera and Sarko stated that it needs to be simple, accurate, and directly managed [Pitera and Sarko, 2010]. The clinical scoring systems of Rockall and Blatchford are rather involved, do not prove to be very accurate, as they seem to assign equally high scores to patients with high- and low-risk stigmata, and would likely result in some unnecessary urgent endoscopies. VCE has many advantages: it does not require sedation, or a hemodynamically stable patient, it poses no harm to the patient, and could enable a gastroenterologist to accurately assess a patient’s need for urgent endoscopy without being physically present at the bedside. Live VCE is a simple tool, found to be accurate as compared with the gold standard of endoscopy, and would effectively direct management to emergent, urgent, or elective endoscopy.
While all UGIB patients should undergo endoscopy within 24 hours [Barkun et al. 2003], the need for, and the timing of, more urgent endoscopy has until now been a subjective decision. Predicting risk in real time with a live view image would result in a superior risk assessment with potential benefit in outcome for patients presenting with UGIB. If our results are validated in larger studies, Pillcam ESO® could become the risk stratification tool of the future.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Sang H. Kim, MD is a consultant for Boston Scientific and Gilead Sciences. Moshe Rubin, MD is a consultant for Given Imaging and is a speaker for Abbott Laboratories. The remaining authors have no conflicts of interest to declare.