
Abstract
The incidence of pancreatitis induced by anastomotic stricture following pancreaticodigestive tract anastomosis as a late-onset adverse event has been reported to be 3% or lower, but some cases repeatedly relapse and are difficult to treat. Endoscopic identification and treatment of the anastomotic site are considered to be difficult, and only a small number of cases have been reported. We present three cases with recurrent pancreatitis induced by anastomotic stricture following pancreaticojejunostomy applied after pancreaticoduodenectomy. We successfully identified the anastomotic site and performed endoscopic dilatation of the anastomotic stricture, and pancreatitis has not recurred. We characterized endoscopic features of the anastomotic site, understanding of which is essential to identify the site, and investigated useful techniques to identify the site and perform cannulation for pancreatography. Furthermore, we showed the safety and usefulness of endoscopic dilatation for anastomotic stricture following pancreaticojejunostomy according to our three cases and a review of the literature.
Keywords
Introduction
Endoscopic identification and treatment of anastomotic stricture following pancreaticojejunostomy are considered to be difficult, and only a small number of cases have been reported [Ishizawa et al. 2011; Menon and Sanaka, 2010; Ikeda et al. 2013; Yane et al. 2014; Park et al. 2013; Shimatani et al. 2015]. We encountered three consecutive cases with recurrent pancreatitis induced by the anastomotic stricture following pancreaticojejunostomy applied after pancreaticoduodenectomy. We identified the anastomotic site and successfully performed pancreatography and endoscopic dilatation of the site in these cases. Many points remain unclear with regard to the endoscopic treatment of the anastomotic stricture following pancreaticojejunostomy applied after pancreaticoduodenectomy. To address this, we examined our three cases and reviewed the literature in order to investigate endoscopic characteristics, useful techniques to identify and perform cannulation of the anastomotic site, and the safety and usefulness of endoscopic dilatation for the anastomotic stricture.
Endoscopic dilatation of anastomotic stricture following pancreaticojejunostomy
A tip attachment was applied to an endoscope (GIF-H290, GIF-2TQ260M, and PCF-PQ260I, Olympus Medical Systems, Tokyo, Japan). When the anastomotic site could be identified, pancreatography was performed using a cannula for contrast imaging (TandemXL, Boston Scientific Japan, Tokyo, Japan, Start Tip V cannula PR-109Q-1 and PR-110Q-1, Olympus Medical Systems, Tokyo, Japan, MTW ERCP-Catheter, MTW Endoscopie Manufaktur, Wesel, Germany). After pancreatography, a guidewire (0.025-inch VisiGlide, 0.025-inch angle VisiGlide2, Olympus Medical Systems, Tokyo, Japan, 0.018-inch Roadrunner, Cook, Wilston-Salem, NC, United States) was placed in the pancreatic duct. When pancreatography could not be directly applied, the wire-guided technique was concomitantly employed. After placing the guidewire in the pancreatic duct, the anastomotic site was dilated using a balloon dilator (MaxPass, Olympus Medical Systems, Tokyo, Japan). When pancreatic calculi were present, they were removed using a crusher catheter (Xemex Lithotripsy Basket, Zeon Medical, Tokyo, Japan). Finally, a 5Fr or 7Fr pancreatic stent (Geenen Pancreatic Stent, Cook, Wilston-Salem, NC, United States) was placed.
Case series
The first case was a 44-year-old woman with branch duct-type intraductal papillary mucinous neoplasm (IPMN) localized at the pancreatic head who underwent pancreaticoduodenectomy with Cattell’s reconstruction. Pathological evaluation demonstrated adenoma. At 1 year postoperatively, she complained of abdominal pain with elevated pancreatic enzymes repeatedly. A computerized tomography (CT) scan and a magnetic resonance cholangiopancreatography (MRCP) revealed swelling of the residual pancreas with dilation of the main pancreatic duct, but no recurrence of IPMN, suggesting that pancreatitis was caused by an anastomotic stricture following pancreaticojejunostomy. We decided to apply dilatation of the anastomotic site. We could identify the anastomotic site narrowing in a pinhole-like opening in the mucosal region with scar and convergence of intestinal folds observed at the front of the endoscope (Figure 1(a)). Pancreatography showed no pancreatic calculus or feature of recurrent IPMN in the duct (Figure 1(b)). A guidewire was placed through the anastomotic site, and the site was dilated to 3 mm at 6 atm with a 4 × 40 mm balloon dilator in one-session (Figure 1(c)), followed by insertion of a 5 Fr pancreatic stent (Figure 1(d)). No adverse event developed. As of 13 months after treatment, the stent has naturally fallen off, but pancreatitis has not recurred.

(a) Pinhole-like opening in the mucosal region with scar and convergence of intestinal folds observed at the front of the endoscope. (b) No pancreatic calculi or recurrence of intraductal papillary mucinous neoplasm was noted. (c) The anastomotic site was dilated to 3 mm at 6 atm using a 4 mm balloon dilator. (d) A 5 Fr pancreatic stent was inserted.
The second case was a 45-year-old man with a main pancreatic duct-type IPMN localized at the pancreatic head who underwent pancreaticoduodenectomy with modified Child’s reconstruction. Pathological evaluation demonstrated carcinoma in situ with cancer-free margins. At 5 years postoperatively, he complained of abdominal pain with elevated pancreatic enzymes repeatedly. A CT scan and a MRCP revealed a swelling of the residual pancreas with dilation of the main pancreatic duct and pancreatic calculi, but no recurrence of IPMN, suggesting that pancreatitis was caused by anastomotic stricture following pancreaticojejunostomy. We decided to apply dilatation of the anastomotic site and removal of pancreatic calculi. We could identify the anastomotic site narrowing in a slit-like opening in intestinal folds (Figure 2). Pancreatography showed calculi scattered in the duct. A guidewire was placed through the anastomotic site, and the site was dilated to 3.3 mm at 6 atm with an 8 × 30 mm balloon dilator in one-session. Pancreatic calculi were removed using a crusher catheter, and a 7 Fr pancreatic stent was inserted. No adverse event developed. As of 14 months after treatment, the stent has naturally fallen off, but pancreatitis has not recurred.

The anastomosed site was a pinhole-like opening buried in intestinal folds in the tangential direction of the endoscope.
The third case was a 59-year-old man with main pancreatic duct-type IPMN localized at the pancreatic head who underwent pancreaticoduodenectomy with modified Child’s reconstruction. Pathological evaluation demonstrated adenoma. At 1 year postoperatively, he complained of abdominal pain with elevated pancreatic enzymes repeatedly. A CT scan and a MRCP revealed a swelling of the residual pancreas with dilation of the main pancreatic duct, but no recurrence of IPMN, suggesting that pancreatitis was caused by anastomotic stricture following pancreaticojejunostomy. We decided to apply dilatation of the anastomotic site. We could identify the anastomotic site narrowing in a small twitching concavity observed in the tangential direction of the endoscope, and difficult to recognize as an opening (Figure 3(a)). Moreover, the region was sensed as being fixed by lining with the pancreas. To confirm that this was the anastomotic site, the region was examined by endoscopic ultrasonography (EUS) using a 20-MHz small-diameter probe (UMQ240, Olympus Medical Systems, Tokyo, Japan) employing the deaerated water filling method. The dilated main pancreatic duct was successfully visualized, confirming the anastomotic site (Figure 3(b)). Pancreatography showed no pancreatic calculus or feature of recurrent IPMN in the duct. A guidewire was placed through the anastomotic site, and the site was dilated to 4 mm at 6 atm with a 4 × 20 mm balloon dilator in one-session, followed by insertion of a 5 Fr pancreatic stent. No adverse event developed. As of 1 month after treatment, the stent has naturally fallen off, but pancreatitis has not recurred.

(a) A small twitching concavity observed in the tangential direction of the endoscope, and difficult to recognize as an opening. (b) The dilated main pancreatic duct was visualized at the lower left by endoscopic ultrasonography.
Discussion
The incidence of pancreatitis induced by anastomotic stricture following pancreaticodigestive tract anastomosis as a late-onset adverse event has been reported to be 3% or lower, but some cases repeatedly relapse and are difficult to treat [Pannala et al. 2011]. Additional surgery is a candidate treatment, but it tends to be avoided in consideration of difficulty in surgery due to adhesion, postoperative re-stenosis, and physical burden on patients. Thus, endoscopic approaches are investigated. In many studies on endoscopic treatment of anastomotic stricture following pancreaticojejunostomy, EUS-guided pancreaticogastrostomy or endoscopic dilatation of the anastomotic site using rendezvous technique and pancreatic duct drainage were performed [Mallery et al. 2004; Papachristou et al. 2007; Barkay et al. 2010; Itoi et al. 2011; Kikuyama et al. 2011; Kurihara et al. 2013; Takikawa et al. 2013], whereas the anastomotic site could be directly identified using endoscopy in only 13 cases including our cases because identification of the anastomotic site was difficult. The anastomotic site could be directly identified using endoscopy in only 10 cases except for our three cases [Ishizawa et al. 2011; Menon and Sanaka, 2010; Ikeda et al. 2013; Yane et al. 2014; Park et al. 2013; Shimatani et al. 2015]. In previous reports, the rate of success of the anastomotic site identification and treatment by endoscope was 8–33%, suggesting that identification of the anastomotic site was difficult [Chahal et al. 2006; Shimatani et al. 2009]. However, the rate of success was 100% in our hospital, although the number of cases was only three. In order to complete treatment, it is necessary to understand the characteristics of the anastomotic site, the way of identification of the site and treatment by endoscope. It was also reported that the findings of secretin-enhanced magnetic resonance cholangiopancreatography (S-MRCP) were useful for the assessment of the exocrine function of residual pancreas, chronic pancreatitis, identification of anastomotic site by endoscopy, treatment plan, guiding therapy [Munazza and Koenraad, 2013; Czakó et al. 2004]. Therefore, S-MRCP may be useful for the assessment of recurrent pancreatitis induced by the anastomotic stricture following pancreaticojejunostomy.
Regarding the characteristics of the pancreaticojejunostomy-applied site, the site was observed in the front of the endoscope in cases treated with Whipple and Cattell’s reconstruction, and in the tangential direction of the endoscope in cases treated with Child’s reconstruction. In the mucosa, the site was buried in intestinal folds and narrowed showing a pinhole-like, slit-like, or membranous shape. In our three cases, twitching and scarred mucosa, residual thread, and slight- and pinhole-like shapes were noted. The intestinal region in which the anastomotic site was buried in folds was sensed as being fixed by lining with the pancreas, being another accessory finding.
In the pancreaticojejunostomy-applied site identification methods employed, including those for our cases, a tip attachment was used to keep a specific distance, and EUS was performed to confirm the pancreatic duct. For cannulation and pancreatography into the anastomotic site, a tapering cannula and thin guidewire, such as one with a 0.018-inch diameter, were used in combination with the wire-guided technique. The 13 cases including our three cases are summarized in Table 1.
Endoscopic characteristics, identification, cannulation and pancreatography technique of anastomotic sites.

Endoscopic dilatation of the anastomotic stricture following pancreaticojejunostomy was performed in 32 cases including our three cases. The anastomotic site was endoscopically identified and dilated using a dilator or balloon in 10 cases [Ishizawa et al. 2011; Menon and Sanaka, 2010; Ikeda et al. 2013; Yane et al. 2014; Park et al. 2013; Shimatani et al. 2015]. The rate of success of anastomotic site identification and treatment by endoscopy directly was 8–33%. The incidence of adverse events was 4.9%. Most of these adverse events were due to endoscopic insertion [Chahal et al. 2006; Shimatani et al. 2009]. However, no adverse event of anastomotic site dilatation occurred. Endoscopic dilatation of the anastomotic site using EUS rendezvous technique was performed in 19 cases [Mallery et al. 2004; Papachristou et al. 2007; Barkay et al. 2010; Itoi et al. 2011; Kikuyama et al. 2011; Kurihara et al. 2013; Takikawa et al. 2013]. The rate of success of EUS-guided treatment was reported to be about 50%, but the incidence of adverse event was 63.6 % [Mallery et al. 2004; Papachristou et al. 2007; Barkay et al. 2010; Itoi et al. 2011; Kikuyama et al. 2011; Kurihara et al. 2013; Takikawa et al. 2013; Kinney et al. 2009; Farrell et al. 2006; François et al. 2002; Will et al. 2007; Pelaez et al. 2007; Kahaleh et al. 2007; Tessier et al. 2007; Ryou et al. 2010; Binmoeller and Nguyen-Tang, 2011; Bataille and Deprez, 2002]. Postoperative adverse event were mostly pancreatic duct puncture-induced pancreatic juice leakage, acute pancreatitis, and abscess around the pancreas. But no adverse event of anastomotic site dilatation was noted. They were followed for 1 year or longer on average after dilatation, and pancreatitis relapsed in only 3.1 % (1/32cases). This patient was a recurrent pancreatic cancer case. Even if the possibility of recurrent pancreatitis after dilatation of the anastomotic site is low, it may be important to follow the dilation of residual main pancreatic duct by CT or MRCP. In our three cases, recurrent pancreatitis was accompanied with dilation of residual main pancreatic duct. Therefore, the exacerbation of dilation of residual main pancreatic duct may predict the restenosis of anastomotic site with recurrent pancreatitis. The 32 cases are summarized in Table 2.
Adverse events and relapse of pancreatitis after endoscopic dilatation of the anastomotic site.
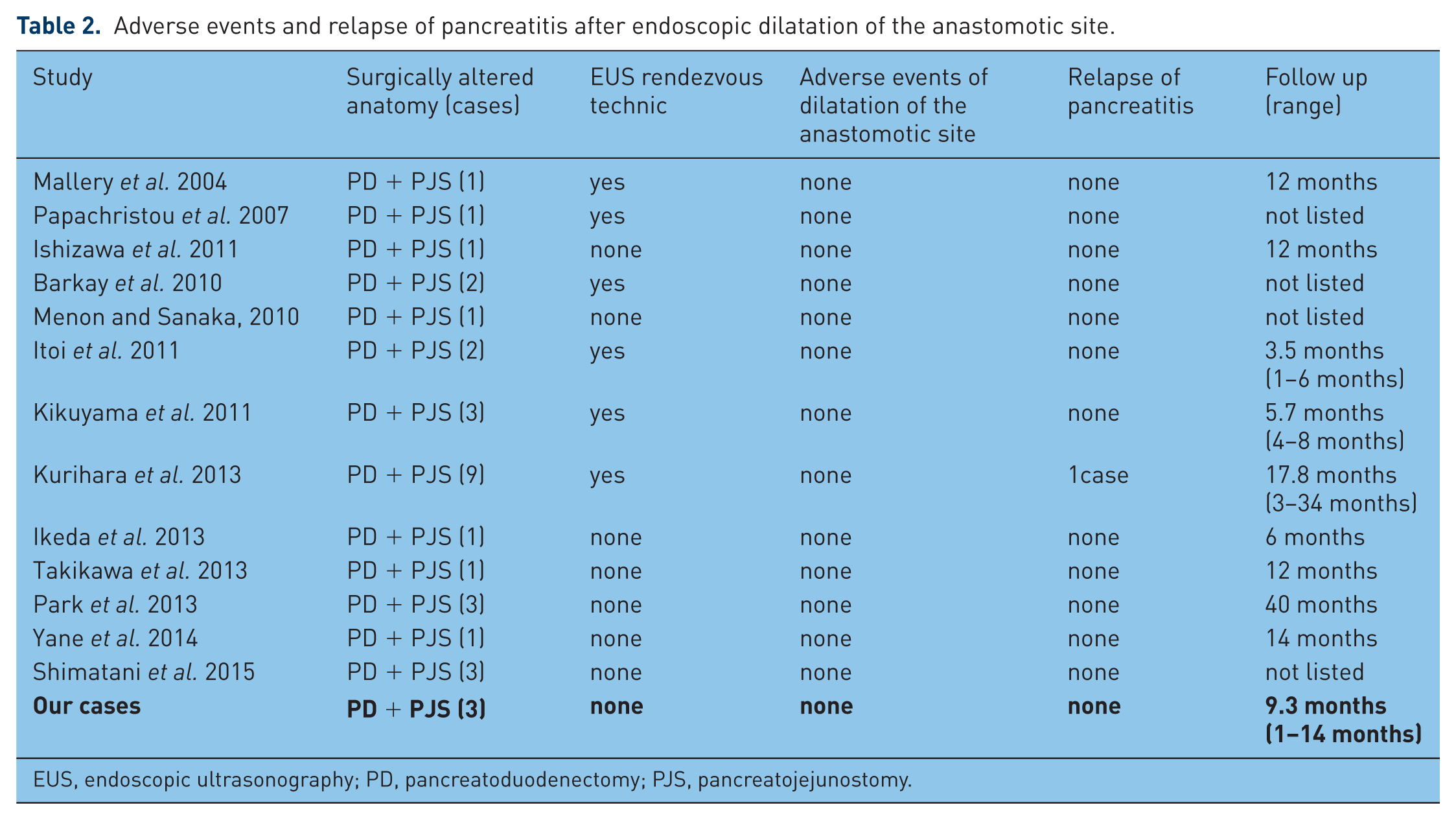
EUS, endoscopic ultrasonography; PD, pancreatoduodenectomy; PJS, pancreatojejunostomy.
Regarding safety, no adverse event of dilatation of the anastomotic site occurred. The adverse event of greatest concern is perforation of the anastomotic site, but it was not reported in any study [Mallery et al. 2004; Papachristou et al. 2007; Barkay et al. 2010; Menon and Sanaka, 2010; Ishizawa et al. 2011; Itoi et al. 2011; Kikuyama et al. 2011; Kurihara et al. 2013; Takikawa et al. 2013; Ikeda et al. 2013; Park et al. 2013; Yane et al. 2014; Shimatani et al. 2015]. The anastomotic site is lined with the pancreas parenchyma, which may be the reason for the absence of perforation. Transient edema may develop after dilatation at the anastomotic site, but dilatation may be safely performed by concomitantly applying pancreatic duct drainage with 5~10Fr pancreatic stent. Regarding the usefulness, excluding one patient with recurrent pancreatic cancer, pancreatitis has not relapsed for 1 year or longer, suggesting high usefulness [Mallery et al. 2004; Papachristou et al. 2007; Barkay et al. 2010; Menon and Sanaka, 2010; Ishizawa et al. 2011; Itoi et al. 2011; Kikuyama et al. 2011; Kurihara et al. 2013; Takikawa et al. 2013; Ikeda et al. 2013; Park et al. 2013; Yane et al. 2014; Shimatani et al. 2015].
From the above, although EUS-guided procedures are more successful than direct endoscopy procedures, the incidence of adverse event of EUS-guided access to the pancreatic duct is very high. According to our three cases and a review of the literature, if the anastomotic site is found and the guidewire could be advanced into the pancreatic duct, endoscopic dilatation of the anastomotic site is safe and very effective in prevention of relapses of pancreatitis.
Conclusion
We characterized endoscopic features of the anastomotic site, the understanding of which is essential to identify the site, and investigated useful techniques to identify the site and perform cannulation for pancreatography. Furthermore, we showed the safety and usefulness of endoscopic dilatation for anastomotic stricture following pancreaticojejunostomy according to our three cases and a review of the literature.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.