
Abstract
Background:
There is little data on the role of balloon enteroscopy and small bowel strictures. We aim to characterize the diagnostic role of double balloon enteroscopy (DBE) in small bowel strictures and document the outcomes of dilatation.
Methods:
This is a retrospective review from a single tertiary referral centre DBE database from July 2004 to September 2012. All patients with suspected strictures in the small bowel undergoing DBE were included. The position of the small bowel strictures considered for dilatation was determined by diagnostic imaging, i.e. CT enterography, MR enterography or capsule endoscopy in the workup before DBE. Endpoints included stricture description, dilatation parameters and response to treatment. Main outcome measurements were the safety and efficacy of DBE and dilatation.
Results:
From our DBE database of 594 patients, a total of 32 patients underwent 44 DBE procedures for suspected or known strictures. Stricture aetiology included Crohn’s disease (CD), nonsteroidal anti-inflammatory drugs (NSAIDs), surgical, Beçhets disease and one unknown. A total of 17 patients did not undergo dilatation as the strictures were ulcerated, nonobstructing or of uncertain aetiology. From the total of 25 dilatations in 15 patients that were attempted, 8/15 (53%) patients had 1 dilatation, 5 patients had 2 dilatations, 1 had 3 dilatations and 1 had 4 dilatations. The mean dilatation diameter was 14 mm. Three patients underwent surgery post-dilatation (2 for perforation). Mean follow up was 16 months.
Conclusion:
DBE is a useful method in determining the need for dilatation by assessing for active ulceration. Dilatation is effective in the 10–18 mm range, however perforation does occur.
Introduction
Small bowel strictures are uncommon but when they occur can be an important cause of morbidity especially in patients with Crohn’s disease (CD). The causes of small bowel strictures include CD, nonsteroidal anti-inflammatory drugs (NSAIDs), neoplastic, post-surgical and idiopathic amongst others. Clinical dilemmas often arise in determining whether a stricture is present, what the degree or severity is and the nature of that stricture. In addition, the anatomical location being the small bowel makes providing treatment to resolve obstructive symptoms difficult.
Until recently, surgery was the mainstay of treatment for obstruction. However, this has potential of serious complications particularly in cases of CD, with serious complications occurring in up to 20% of cases in one recent study [Gardiner and Dasari, 2007]. Surgical morbidity also includes intra-abdominal adhesions [Parker et al. 2005], short bowel syndrome [Lee and Papaioannou, 1982], and restricturing. First introduced in 2001, balloon-assisted enteroscopy (BAE) and the development of the double balloon enteroscopy (DBE) system allowed for the opportunity to perform therapeutics in the small bowel [Yamamoto et al. 2001]. There have been limited publications of DBE and endoscopic dilatation in small bowel strictures [Despott et al. 2009; Karstensen et al. 2012]. This limited data is positive with a good safety profile and effectiveness; however the data is limited in several ways. First, there are limited patient numbers [Ohmiya et al. 2009]. In addition, the degree of dilatation is only stated in two series and both were in patients with CD [Despott et al. 2009; Karstensen et al. 2012]. Finally, there is no data to recommend a safe and effective approach to dilating small bowel strictures.
We conducted our retrospective study to determine the role of DBE in assessing strictures and the safety and efficacy of dilatation in the small bowel.
Materials and methods
We retrospectively reviewed our DBE database for patients undergoing DBE for known or suspected small bowel strictures. The data was collected between July 2004 and September 2012. Our centre is a tertiary referral university hospital in Sydney, Australia. All patients in our case series were referred to our centre from external gastroenterologists. All but two patients presented with intermittent small bowel obstructive-type symptoms (two had iron deficiency anaemia). Patients with acute and unresolved obstruction were not included. The position of the small bowel strictures considered for dilatation was determined by diagnostic imaging, i.e. computed tomography enterography (CTE), magnetic resonance enterography (MRE) or capsule endoscopy (CE) in the workup before DBE. The route of procedure was determined by the endoscopist and was based on the clinical scenario and imaging findings. Our general approach was to perform an oral approach DBE if we felt that the lesion was in the proximal two-thirds of the small bowel and an anal approach DBE if in the distal third or via a stoma if this was considered the shortest distance to the stricture. This is based upon clinical studies in small bowel overt gastrointestinal bleed (OGIB) [Gay et al. 2006]. All patients undergoing anal approach DBE had bowel preparation.
The data collected included: patient demographics, stricture characteristics, dilatation diameter and success, symptom resolution, need for repeated dilatations, complications and surgery pre procedural imaging, change in management of inflammatory bowel disease (IBD) and follow up. A total of 32 patients (mean age 52.7 ± 15.1 years, 17 female) underwent 44 BAE for suspected or known strictures. Dilatation was performed under direct vision for all but one case, in which insertion was through the stoma and an image intensifier was required. Patient details and baseline characteristics are summarized in Table 1.
Baseline demographic characteristics.

There was no specific approach to dilatation and this was determined by the endoscopists performing the procedure. However, patients with severely ulcerated or inflamed strictures were not dilated due to the high perforation risk. Also patients in whom the scope could traverse the stricture were not dilated, as this would be an unlikely cause of their obstructive symptoms. The diameter of dilatation performed varied according to the stricture size, whether the stricture allowed passage of the scope and the likely nature of the stricture, as NSAID strictures are superficial compared with potentially full thickness CD strictures. Data on the morphology of the stricture was recorded as was the dilatation diameter performed. Only one dilatation per procedure was performed. The goal of dilatation was to allow passage of the scope. All dilatations were performed with the colonic length balloon dilator (Boston Scientific, Boston MA).
Preparation and instrument
The preparation for the procedures included a fasting period of 8 h before the oral procedure and a routine bowel preparation with sodium-picosulfate-based (Picoprep, Pharmatel Fresenius Kabi Pty Ltd, Hornsby, Australia) or sodium-phosphate-based preparations (Fleet, Ferring Pharmaceuticals, Gordon, Australia) with a clear fluid diet the day before the procedure for the anal approach.
The DBEs were performed using the Fujinon therapeutic DBE system with the following components: a EN-450T5/20 video enteroscope (2.8 mm channel, 200 cm working length and 9.3 mm external diameter), a 400 (VP-402, XL 402) processor and a TS-12140 overtube (140 cm length and 12 mm external diameter), 2 latex balloons (1 each at the distal end of the enteroscope and the overtube) and a PB-10 balloon controller (pressure-controlled pump). The technique of performing DBE has been previously described in the literature by Yamamoto and colleagues [Yamamoto et al. 2001]. A controlled radial expansion dilatation balloon (Boston Scientific) was used for stricture dilatation.
All procedures were performed with conscious sedation utilizing a combination of midazolam (Pfizer, Bentley, Australia) or propofol (Fresofol 1%, Pharmatel Fresenius Kabi Pty Ltd, Hornsby, Australia) plus fentanyl citrate (Mayne Pharma Ltd, Mulgrave, Australia) and were administered by the endoscopist or anaesthetist if available.
We received institutional ethics approval to conduct this study.
Results
From our DBE database of 594 patients, a total of 32 patients (mean age 52.7 ± 15.1 years, 17 female) underwent 44 DBE (3 antegrade, 3 stoma, 26 retrograde) for suspected or known strictures. Stricture aetiology included CD in 20, NSAIDs in 7, surgical in 3, Beçhet’s disease in 1 and ischaemic in 1 other.
Out of the 32 patients, 15 had dilatation performed. The reasons to not dilate the strictures in 17 patients included severely ulcerated strictures (n = 8), the stricture was not obstructing (scope passed through easily; n = 6) and miscellaneous reasons (1 uncertain aetiology referred for surgery, 1 sedation failure, 1 extreme angulation). The patient flow is summarized in Figure 1.
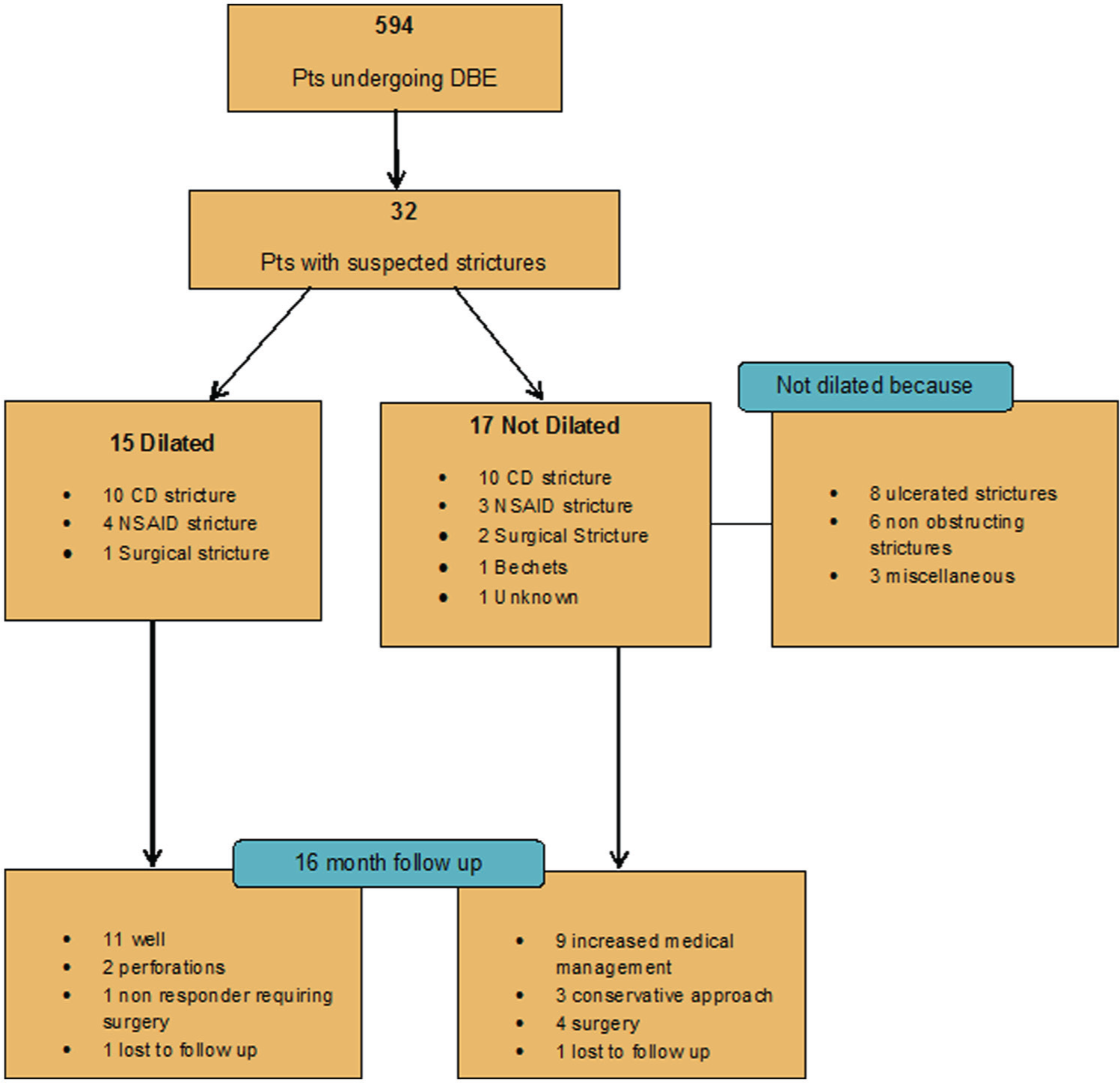
Patient flow diagram. DBE, double balloon enteroscopy; CD, Crohn’s disease; NSAID, nonsteroidal anti-inflammatory drugs.
In 15 patients that underwent dilatation, 10 had CD strictures, 4 NSAID strictures, and 1 surgical stricture. All but one was for obstructive symptoms (two patients had a retained capsule) and one for a retained capsule alone (Figure 2). From the total of 25 dilatations that were attempted, 8/15 (53%) patients had 1 dilatation, 5 patients had 2 dilatations, 1 had 3 dilatations and 1 had 4 dilatations. The mean dilatation diameter was 14 mm (range 10–18mm). Intervention details and location of strictures summarized in Table 2.
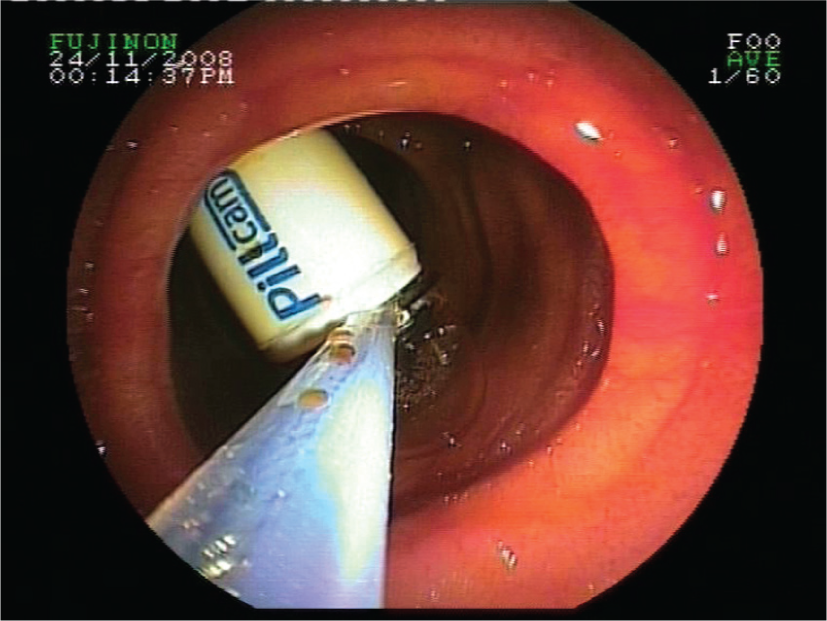
Dilation of stricture and retrieval of a retained capsule.
Intervention details and location.

sx, surgery; mx, management; CE, capsule endoscopy; CD, Crohn’s disease; CT, computed tomography; MRE, magnetic resonant enterography; NSAID, nonsteroidal anti-inflammatory drug.
Outcomes
Clinical benefit
Two patients were lost to follow up and in the remaining 30 patients the mean follow up was 16 (3–60) months. A total of 12 of the 15 patients dilated (80%) had clinical improvement. Of the 14 patients with obstructive symptoms, 11 (78.6%) had resolution of these symptoms with dilatation (1 failed to improve and 2 perforated). Of the three cases with retained capsules all three were retrieved successfully. Two of these three cases also had obstructive symptoms and these resolved post-dilatation. In the three patients who did not benefit, one patient with CD strictures had two dilatations with very short-lived benefit and then opted for surgery. Perforation occurred in two patients with CD and both required surgery.
Complication rates
The only reported complication was perforation. The complication rate was 2/15 (13.3%) per patient or 2/25 (8%) per dilatation. As both perforations occurred in patients with CD the risk in these patients was 2/10 (20%). Both patients had mild associated ulceration (Figure 3) and were dilated to 15 mm. One of these two cases had the nonobstructing jejunal stricture with a retained capsule. The other patient had a distal ileal stricture that was obstructing and had previously responded to 15 mm dilatation.

Mildly ulcerated small bowel stricture.
Discussion
The role of DBE is dual providing a diagnosis and therapy. In our hands dilatation was deemed unnecessary or inappropriate in 17 cases (53%). As less than half had dilatation attempted, the dominant role for DBE in our practice is diagnostic. DBE as a diagnostic tool has been previously established with Oshitani and colleagues reporting in their study of patients with established CD undergoing DBE for evaluation of active disease that DBE was superior to radiologic evaluation for the detection of aphthae, erosions and small ulcers in the ileum [Oshitani et al. 2006]. A study by Mensink and colleagues showed that in patients with active small bowel CD up to 75% of this cohort had an escalation in medical management with excellent outcomes in their follow up [Mensink et al. 2009] indicating this as an appropriate therapeutic algorithm as an alternative to endoscopic dilatation. This is in keeping with our experience where strictures due to disease activity were only determined at DBE despite previous cross-sectional imaging. However, an international consensus statement on the role of small bowel endoscopy in the management of IBD concluded that there is not enough data to recommend DBE, unless conventional diagnostic modalities have been inconclusive and histological diagnosis would alter disease management. This was primarily due to a paucity of data available about the application of this novel endoscopic modality in IBD patients. Nonetheless, DBE and other device-assisted enteroscopy techniques were endorsed as valid modalities for the diagnosis of CD because histological corroboration is available [Bourreille et al. 2009].
When endoscopic dilatation was indicated we had good technical success with 80% having clinical improvement. This is in keeping with previous studies on DBE dilatation of small bowel strictures. Furthermore, our experience is similar to other published work with regards to the need for multiple treatments particularly in CD [Mueller et al. 2010; Thienpont et al. 2010]. In a Dutch study 74% required repeat dilatation [Karstensen et al. 2012]. Dilatation with DBE can be repeated if strictures recur, this does not mean that the primary dilatation was a failure, especially when taken in context that repeat surgery after stricturoplasty may be as high as 25% over a follow up of 30 months [Tichansky et al. 2000].
The optimal algorithm for dilating strictures remains uncertain. This is especially the case with CD. In our series two perforations occurred, making the risk at around 20% in this group of patients. Studies in ileo-colonic dilatation have reported perforation rates as high as 20% [Couckuyt et al. 1995; Singh et al. 2005]. The reasons remain unclear. Both cases had a small amount of inflammation associated with the stricture and during DBE was not considered significant or severe. Also, both were dilated to 15 mm diameter. Hence, we would recommend that dilatation of a stricture that has any degree of associated inflammation should be restricted to less than 15 mm and probably no more that 12 mm which appeared to be safe in our experience.
Our series also suggests that NSAID-related strictures are most commonly found in the distal small bowel whereas CD strictures can occur anywhere in the small bowel. Hayashi and colleagues postulated that the NSAID-induced mucosal injuries in the ileum tend to become more severe than those in the jejunum because of the differences in the bacterial flora and immune system between jejunum and ileum [Hayashi et al. 2009]. The diaphragm-like stricture is thought to be pathognomonic of NSAID injury (Figure 4), which is likely a scarring reaction secondary to ulcerative injury during long-term NSAIDs use [Kelly et al. 2005; Matsuhashi et al. 1992]. We should suspect diaphragm disease when we see a patient with both obstructive symptoms and chronic NSAID use. Diaphragm disease is now regularly visualized on capsule endoscopy. In our series we had patients with entrapment of the capsules. Intestinal resection was formerly the only option for patients with diaphragm disease in the small bowel. Recently, DBE enabled us to treat diaphragm disease in the small bowel [Mehdizadeh and Lo, 2006]. Most stricturing disease is not numerically excessive and can be managed endoscopically [Despott et al. 2009; Ohmiya et al. 2009; Pasha and Leighton, 2009].

Diaphragm stricture secondary to NSAIDs.
In conclusion, our study shows that the technique of DBE assisted small-bowel stricture dilatation for selected patients is of significant benefit and should be considered when possible as a useful and effective alternative to surgical resection or stricturoplasty. Care should be taken to limit the diameter of dilatation if any degree of inflammation is present at the stricture site.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.