
Abstract
Background:
Despite recent emerging literature involving the utility of endoscopic balloon dilation (EBD) of strictures via balloon-assisted endoscopy (BAE), specifically regarding the management of Crohn’s disease (CD), the optimal clinical approach with balloon systems has been largely neglected in academic literature.
Objectives:
This study assesses the intra-procedural success and safety of EBD via BAE for small bowel CD strictures while detailing our clinical approach and technique. Secondarily, we compare the single-balloon endoscope (SBE) and double-balloon endoscope (DBE) systems for EBD-related outcomes.
Design:
Retrospective consecutive patient cohort analysis.
Methods:
We retrospectively assessed a consecutive small bowel CD patient cohort undergoing BAE at the University of Alberta Hospital endoscopy unit from 2013 to 2020. The primary endpoint discerned the safety and immediate success rate of EBD during endoscopy, and comparisons of the dilation parameters and efficacy of SBE versus DBE were assessed as secondary outcomes.
Results:
During the study period, 87 patients (44 male) with a mean age of 56 ± 14.7 years underwent 179 endoscopic procedures (92 DBE and 87 SBE). Of 358 strictures encountered, 320 (89.4%) were successfully dilated and traversed. The mean maximum dilation diameter was 15.76 ± 2.10 mm. There were no perforations or major adverse events.
Conclusion:
EBD via BAE is a safe procedure in small bowel CD with a high intraprocedural success rate. Overall, SBE had a higher success rate in traversing strictures before and after dilation using our technique. This analysis is limited by the retrospective nature of our study and must be balanced against the inherent benefits of the DBE system.
Plain language summary
This study investigated the safety and success of using balloon-assisted endoscopy as a method to dilate small bowel strictures in patients with Crohn’s disease. As a secondary outcome, we compared the overall safety and success between two different types of endoscopic systems: the single- and double-balloon systems.
Background
In stricturing Crohn’s disease (CD), inflammation results in the narrowing of the intestinal lumen.1–4 Occurring in up to 40% of ileal CD patients,5–7 these strictures may cause pain and bowel obstruction and potentially require surgical intervention.8–12 Balloon-assisted endoscopy (BAE), which includes single-balloon endoscopy (SBE) and double-balloon endoscopy (DBE), employs an overtube-and-balloon system to access the small bowel, facilitating direct mucosal assessment and therapeutic intervention. Endoscopic balloon dilation (EBD) via BAE has proven to be a safe, effective treatment for stricturing CD, with the potential to postpone or even eliminate the need for intestinal resection.13–21
While studies have shown the utility and safety of EBD via BAE in CD and recently an excellent set of guidelines was published based on expert Japanese consensus for CD stricture dilation, 22 there is limited explication in the literature detailing the optimal approach to BAE-specific stricture dilations vis-a-vis pre-procedural planning and intra-procedural technique.23–25 Similarly, there is a scant comparison of the therapeutic utility of SBE versus DBE in a large single-center cohort.
Our center integrates BAE (SBE and DBE) into inflammatory bowel disease (IBD) management with a high volume of procedures performed to assess and manage CD strictures. The primary goal of this study is to evaluate the safety and efficacy of EBD performed via BAE for CD strictures while detailing our approach and intra-procedural technique. Secondly, we compared the utility and safety of the two BAE systems – DBE and SBE – as tools in stricturing CD.
Materials and methods
Study design
Patient group
We included all patients who had undergone BAE at our center with a diagnosis of CD and a significant stricture encountered endoscopically. Patients’ diagnosis of CD was determined by clinical, endoscopic, histopathologic, and imaging features; we excluded patients with unclear diagnoses or strictures from non-CD causes (e.g. non-steroidal anti-inflammatory drug (NSAID) use or ischemia).
Data sources and collection
This study was approved by the institutional review board at the University of Alberta Hospital (UAH), examining the safety and outcomes of BAE in IBD patients (Pro 00059254). We reviewed all BAE performed at UAH from 2013 to 2020 via procedural reports and selected procedures that encountered a small bowel stricture. Patient and procedural data were collected from a cohort of prospectively followed patients, including age, sex, disease duration, history of intestinal surgery, medication history, and Montreal classification. Procedure data included the balloon system used (SBE/DBE), route (rectal/oral), and indication for endoscopy (disease assessment, prospective stricture dilation based on prior investigation, obstructive symptoms, query CD), procedural outcomes, and adverse events. We also recorded whether the endoscopy was the patient’s initial procedure or a follow-up to a previous BAE. EBD data included the number of strictures encountered, number of strictures successfully dilated, maximum diameter (mm), change in inflation diameter (mm), type of stricture (de novo/anastomotic), stricture location, complicated/complex stricture (stricture >4 cm, or fistulae/severe ulceration in the stricture), approach to EBD [non-traversable prior to dilation (pre-traversal dilation) versus traversable prior to dilation (post-traversal dilation)], and overall stricture traversability (taking into account both strictures that failed dilation and traversal, and those not deemed amenable/safe for dilation and/or traversal).
The reporting of this study conforms to the STROBE statement. 26
Outcomes
The primary endpoint concluded intraprocedural success and safety of BAE-facilitated-EBD defined as successful stricture dilation and traversal. We further analyzed the procedural outcomes based on whether the procedure was an initial versus a repeat BAE. A secondary analysis of SBE versus DBE outcomes was further conducted.
Statistical analysis
Descriptive statistics were performed to assess patient demographics, procedural data, outcomes, and EBD information. We compared SBE and DBE via proportion analysis. Because there was no a priori reason to believe that the modalities would differ in terms of endoscopic outcomes, our null hypothesis suggested there would be no difference in the proportions of these outcomes. We used a two-tailed proportion analysis at a significance level of α = 0.05 to qualify the rejection of the null hypothesis. As such, p values <0.05 indicate a statistically significant difference between the two modalities.
Procedures
High-volume balloon endoscopists (BH, SZ-G, and CT) performed all procedures at the UAH endoscopy suite with either the Olympus Single Balloon Enteroscope (EVIS EXERA II SIF-Q180) or the Fujifilm Double Balloon Enteroscope (EN450 T5 or EN580T). The choice of endoscopic system was determined by availability and endoscopist preference. The tip balloon was adhered to the scope with standard elastic bands. Carbon dioxide insufflation (CO2) was used in all procedures. The Zutron Medical Enteroscope Stiffening System was employed as required. Through-the-scope controlled radial expansion (CRE) balloon dilation catheters (Boston Scientific) were used for all dilations. The guide wire used, when required to facilitate balloon passage prior to stricture traversal, was the CRE balloon guidewire. No third-party guidewires were used. No procedures employed fluoroscopic guidance for scope movement or stricture assessment/dilation. All BAE at UAH were performed with anesthesiology support; patients with oral procedures underwent orotracheal intubation and rectal procedures varied based on anesthesia preference, procedure length, and patient comorbidity with the majority undergoing conscious sedation with Propofol.
Dilation technique/approach
Our approach to EBD via BAE is summarized in Figure 1. Following the initial assessment, patients underwent cross-sectional imaging to determine the procedural route (oral, rectal, or stoma) and assess for disease complications that would compromise BAE/EBD safety and/or warrant surgical intervention (e.g. severe internal fistula, phlegmon, abscess). Our cross-sectional imaging modality of choice is computed tomography enterography, but MR enterography and non-enterography CT were used in some cases if previously ordered and deemed adequate for assessment. Select cases were discussed at multidisciplinary rounds (involving radiologists, endoscopists, and IBD specialists) to evaluate the endoscopic approach, feasibility, and safety.

Algorithm for stricture assessment in Crohn’s disease.
All endoscopically significant strictures, as determined by the endoscopist, encountered were included in this analysis. In terms of indication for dilation, this was an operator decision based on an amalgam of symptoms, stricture appearance, and feasibility. Of note, both patients with and without obstructive symptoms were present in this cohort. Aside from symptoms, dilation facilitates scope/overtube traversal and may treat subtle/intermittent obstructive symptoms and/or serve to prevent future episodes. Active obstructive symptoms were not required criteria for dilation. The ability to traverse a stricture did not qualify it as endoscopically insignificant as the scope tip diameter is between 9.2 and 11 mm in BAE systems (Supplemental Table 1), significantly lower than our target dilation range of 15–18 mm. In addition, our scope tip dilation technique allowed traversal of complicated strictures of small diameter prior to dilation, as detailed below. As such, strictures that were traversable prior to dilation were included in this analysis. That said, not all strictures encountered were dilated. Non-dilated strictures were not counted or included in this analysis unless they were not traversable and felt not amenable to dilation/dilation not performed – these were considered a non-traversable stricture. A stricture was considered amenable to EBD based on length (<4 cm), visualization of the bowel passed the stricture, and no severe surrounding inflammation, ulceration, bowel tethering, or fistula(s).
After inspection, initial traversal was attempted via gentle pressure to facilitate post-traversal dilation instead of pre-traversal dilation of a stricture (Figure 2). If the stricture was not initially easily traversed, we attempted to manually dilate or ‘walk’ through the stricture using slow concentric motions of the scope tip (Figure 3). This slow circumduction of the tip facilitated scope passage through some initially ‘non-traversable’ strictures prior to balloon dilation. Post-traversal dilation is preferred because it allows for the assessment of the tissue proximal and distal to the stricture before exerting the shearing forces of dilation (Figure 2-3). It also allows for direct and controlled passage of the CRE balloon rather than blindly through a stricture, effectively decreasing the risk of unintentional bowel damage and perforation. If the stricture could not be traversed, dilation was performed pre-traversal (Figure 2-2).

Pre-traversal versus post-traversal approach to stricture dilation. On passage of the enteroscope and encountering a stricture, (1) the stricture was passed via pressure or with the use of scope tip dilation (see Figure 2). If non-traversable, (2a) the dilation balloon catheter was passed and the stricture dilated (2c) to allow traversal (2d). If traversable, (3a) the upstream bowel can be fully assessed and then subsequent stricture dilation (3b and 3c) can occur prior to further scope passage or withdrawal (3d).

Scope tip stricture dilation or ‘stricture walk’. (1) Non-traversable stricture encountered. (2) Scope tip is impacted into the stricture. (3) The tip is then deflected using the large and small wheels of the scope to maneuver through the stricture while dilating it with gentle circumduction. (4) Once sufficiently dilated, the scope will traverse the stricture and (5) forward passage is possible without the use of a balloon catheter initially.
Once initial traversability was established, EBD was undertaken. To facilitate the passage of the balloon catheter, the working channel of the endoscope was often primed with Lipiodol. With the balloon catheter properly positioned, dilation with a target diameter of 15–18 mm was performed under direct visualization to monitor for mucosal tears or perforation. The balloon was held at target diameters for a minimum of 60 s. Technical success was defined as the ability to successfully dilate and traverse the stricture during the procedure. No fluoroscopy was used in our cohort. We carefully examined the area post-dilation to evaluate for immediate complications such as perforation or bleeding.
Results
Participants
Over the course of the study period, 160 patients underwent BAE; 87 (54.4%) met the inclusion criteria (Figure 4).

PRISMA (Preferred Reporting Items for Systemaic Reviews and Meta-Analyses) flow chart for study inclusion.
Patient demographics
This patient cohort comprised 87 patients (44 males and 43 females) with small bowel CD. Table 1 summarizes patient demographics. The mean age was 53.9 ± 14.7 years and the mean disease duration was 19.2 ± 14.6 years. In all, 55 (63.2%) patients had a previous intestinal resection, and 62 (71.3%) were on biologic therapy for CD.
Demographics for patients with small bowel CD who underwent EBD.

Montreal classification: (1) Age at diagnosis – A1: 16 years or younger, A2: 17–40 years, A3: 40 years or older; (2) disease location – L1: terminal ileum, L2: colon, L3: ileo-colon, L4: upper GI; (3) behavior – B1: non-stricturing/non-penetrating, B2: stricturing, B3: penetrating, p: perianal.
CD, Crohn’s disease; EBD, endoscopic balloon dilation; GI, gastrointestinal.
Procedural data
Indication
Overall, 179 endoscopic procedures (92 DBE and 87 SBE) were performed (Table 2 summarizes the overall procedural data). The procedural approach was 90.5% via the rectal route. Indications for endoscopy varied as per the table; in 131 procedures (73.2%), the patient had previous obstructive signs or evidence of significant stricturing.
Procedural data for SBE and DBE involving EBD for patients with small bowel CD.

Recorded indications were as follows: stricture dilation with obstructive symptoms, disease assessment (no obstructive symptoms), and patients with no prior diagnosis of CD – query CD.
BAE, balloon-assisted endoscopy; CD, Crohn’s disease; CTE, computed tomography enterography; DBE, double-balloon endoscopy; EBD, endoscopic balloon dilation; SBE, single-balloon endoscopy.
EBD and stricture traversability
During 179 procedures, endoscopists encountered 358 intestinal strictures of which 89.4% (320/358) were successfully dilated and traversed. The mean dilation diameter was 15.76 ± 2.1 mm. The strictures dilated were 76.9% native bowel/de novo. Of the total dilations performed, 194 (60.6%) were done post-stricture traversal (Table 3). One in six (15.4%) strictures encountered were classified as complicated/complex. The success rate for EBD of these lesions was 92.7% compared to 88.8% in the non-complicated group (p = 0.38); there was a significantly lower mean dilation diameter (p = 0.02) and more pre-traversal dilation (p < 0.001) (Table 4). In total, 38 strictures (10.6%) were deemed non-traversable and subcategorized: (1) not-amenable/unsafe due to endoscopic appearance and lack of initial traversability for EBD, 8.7% (31/327), and (2) non-traversable despite EBD, 2.0% (7/327).
Overall Stricture characterization and dilation data. Overall data and Specific Endoscopic system presented.
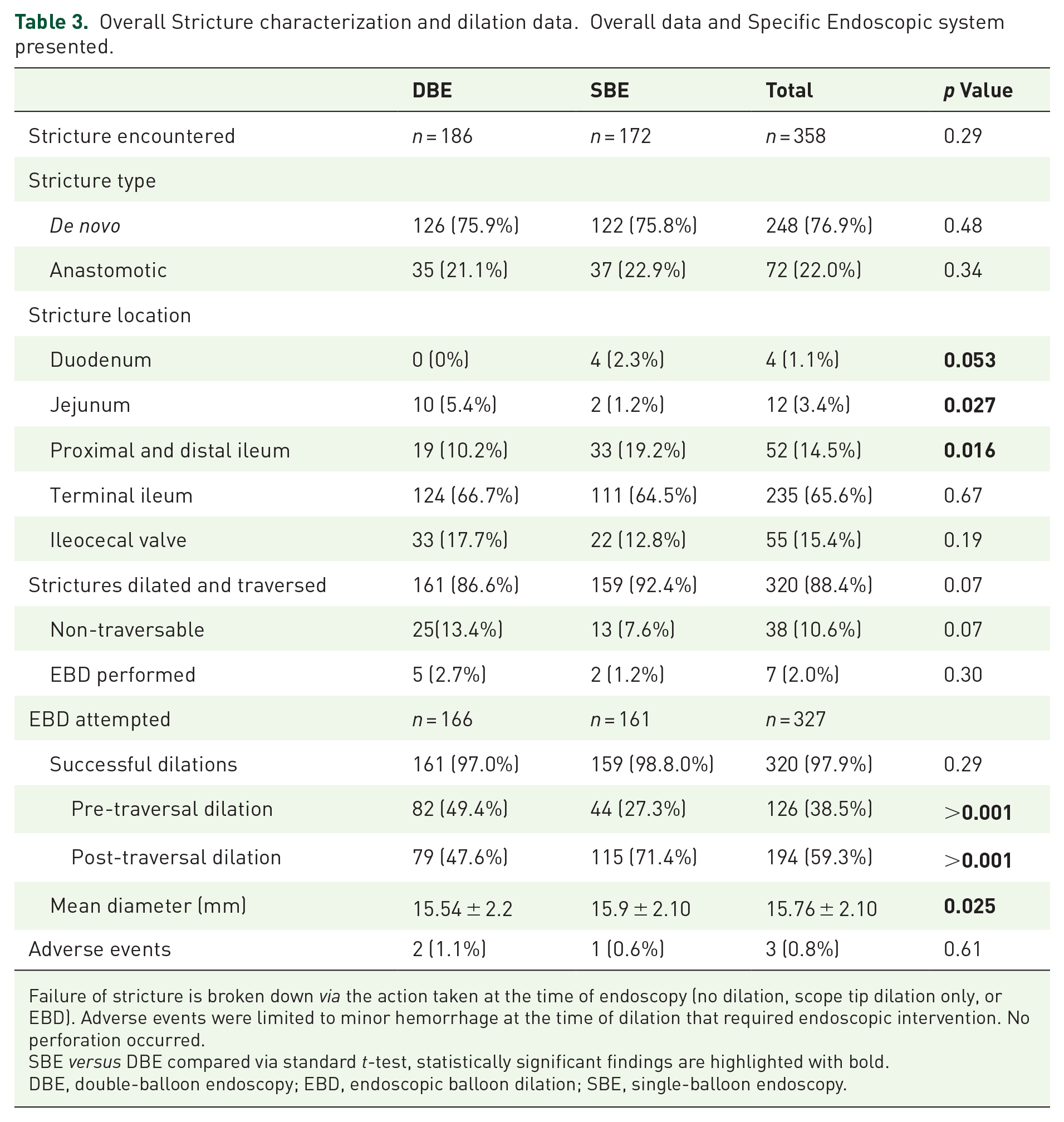
Failure of stricture is broken down via the action taken at the time of endoscopy (no dilation, scope tip dilation only, or EBD). Adverse events were limited to minor hemorrhage at the time of dilation that required endoscopic intervention. No perforation occurred.SBE versus DBE compared via standard t-test, statistically significant findings are highlighted with bold.
DBE, double-balloon endoscopy; EBD, endoscopic balloon dilation; SBE, single-balloon endoscopy.
Procedural and endoscopic characteristics for EBD of complicated strictures - heavily ulcerated or fistula present.

No meaningful difference was found between SBE and DBE. There were no major adverse events or perforations.Comparison of complicated to non-complicated strictures made via standard t-test, statistically significant findings highlighted in bold.
CD, Crohn’s disease; DBE, double-balloon endoscopy; EBD, endoscopic balloon dilation; SBE, single-balloon endoscopy.
Initial versus repeat endoscopy
In all, 79 (44%) procedures were performed as initial endoscopic assessments: 49 DBE versus 30 SBE (p = 0.03). In all, 100 procedures were performed as a repeat/follow-up BAE: 57% were SBE (p = 0.047). Successful dilation was higher in the follow-up BAE group (92.2% versus 85.1%, p = 0.034) as were dilation diameter and the amount of post-traversal dilation (Table 5).
Comparison of endoscopic balloon dilation outcomes in SBE and DBE at the initial endoscopic appointment (no prior BAE) and subsequent follow-up appointments for patients with small-bowel Crohn’s disease.

Non-traversable includes strictures that were attempted to be dilated and failed or were not amenable to EBD.
BAE, balloon-assisted endoscopy; DBE, double-balloon endoscopy; EBD, endoscopic balloon dilation; SBE, single-balloon endoscopy.
Single-balloon endoscopy versus double-balloon endoscopy
EBD via SBE had a higher mean maximum dilation diameter (15.9 ± 2.1 versus 15.5 ± 2.2, p = 0.025) and more post-traversal dilations (115 versus 79, p < 0.001). A DBE was initially used in five (2.8%) procedures but replaced intra-procedure with an SBE through the double-balloon overtube. Two of these procedures required switching due to technical problems with the DBE (e.g. scope damage or inability to pass the CRE balloon through the working channel). In the remaining three procedures, the DBE scope could not successfully traverse a stricture despite dilation, whereas the SBE scope was able to safely traverse the strictures in all three cases.
At initial assessment with BAE, SBE had a higher rate of successful dilation and traversal (93.7% SBE versus 77.9% DBE, p = 0.003), although this did not reach statistical significance in the overall group (92.4% SBE versus 88.6% DBE, p = 0.07) (Table 5). In the repeat BAE group, successful dilation was similar when comparing BAE systems (p = 0.78). Maximum dilation diameter (15.7 versus 16.2 mm, p = 0.042) and the ability to traverse the stricture prior to dilation (55.4% versus 77.8%, p = 0.008) were again more significant with SBE.
Adverse events
There were no major adverse events (e.g. perforation, postoperative pancreatitis, hospitalization, or death) in all 156 procedures. Three (0.8%) minor intraprocedural post-endoscopic hemorrhaging requiring endoscopic interventions were reported. There was no statistical difference in reported adverse events requiring intervention between the two modalities.
Discussion
As the largest single-center cohort of BAE-assisted CD stricture dilations in the published medical literature outside of Japan, 27 our data demonstrate that EBD is safe and effective. Considering the study participants under investigation were primarily complicated CD patients (63% having prior intestinal resections) coupled with a large mean dilation diameter (15.8 mm), the findings of this study further support the safety of EBD for stricturing CD patients. Our high success rate (89.4%) for overall dilation and traversal corresponds with rates reported by other EBD studies.28–30 Of note, this counted all strictures that could not be traversed regardless of whether dilation was performed or not. If one looked strictly at the success rate of dilations performed, it was 97.9% (Table 3). The failure to dilate and traverse strictures occurred more frequently during DBE compared to SBE, especially at a patient’s initial enteroscopy (p = 0.009). That said, there were significantly more DBE performed as the initial endoscopic technique, which means this may suggest DBE was used for more complicated/difficult procedures. Our data further suggest that SBE may have advantages over DBE for traversing CD stricture using our technique, facilitating more post-traversal dilation and achieving a higher mean dilation diameter, although this was not a controlled comparison of the two systems.
Most strictures (78%) encountered were de novo, highlighting the utility of EBD in stricturing CD patients without previous intestinal resection. Initial EBD studies focused on treating anastomotic strictures, yet increasing literature demonstrates the utility of native stricturing.31–33 A recent systematic review with meta-analysis, to which we contributed significant patient data, indicated short-term clinical effectiveness in 82.3% of patients and a surgery-free rate of 72.6%. 34
As noted in the Section ‘Materials and methods’, the need for dilation was made based on endoscopic appearance and was performed in symptomatic and asymptomatic individuals as well as in strictures that were traversable via the enteroscope. Our approach is that these both facilitate scope and overtube passage, as well as treat the present and future risks of obstructions. It is also very difficult to tell how fibrous a stricture is without dilation, as a response to the balloon dilation can be key in its classification (i.e. visible fibrous stretch through the balloon, mucosal disruption, and hemorrhage post-dilation). Furthermore, a BAE procedure and access to the small bowel are laborious and resource-intensive, so we try to apply maximum therapeutic benefit at the time of endoscopy. In our experience, there is very little risk of complication with EBD as noted in our results. However, this approach needs to be balanced against perforation and patient harm. Also of note, in our cohort, 38 strictures overall were not attempted to be dilated at the time of enteroscopy, as per the criteria in our methods, and likely increases the safety of this approach.
The safety profile of BAE EBD was excellent with no perforations or significant adverse events, lower than reported in other studies.20,21,35 This is likely due to several factors: experienced endoscopist performing all procedures, our pre- and intra-procedural approach to dilation (Figure 1), and our emphasis on initial stricture traversability pre-dilation (Figure 2) – facilitated by scope tip dilation (Figure 3) at the time of stricture assessment. We also schedule all procedures with anesthesia support, enhancing patient safety and overall procedural success.
The structure of the BAE scope is ideal for IBD assessment and stricture dilation, regardless of whether deep enteroscopy is required. The BAE has a narrower diameter (Supplemental Table 1), increased flexibility, and greater stability afforded by the overtube and balloon system; thus, increasing the likelihood of reaching and traversing disease segments, whether colonic, distal ileal, or in the midgut.33,36 This is also why traversable strictures were dilated; a goal of 15–18 mm is our targeted diameter for stricture dilation, which is much larger than the SBE or DBE scope diameter (Supplemental Table 1).
Scope tip dilation
Our novel technique of scope tip dilation (Figure 3) enhances initial stricture traversal allowing for upstream visualization and post-traversal dilation (Figure 2). This obviates the need for fluoroscopy, which is cumbersome and a source of radiation, instead allowing the endoscopist to evaluate the bowel completely before undertaking dilation (discussed below). When applying this technique, the endoscopist must be mindful of the tension on the scope to avoid damaging the internal angulation wires.
A higher stricture traversal rate (both pre-dilation and overall) has a meaningful impact on the management of CD. A non-traversable stricture prevents other strictures from being accessed, decreasing the efficacy of the procedure from a dilation perspective, and potentially necessitating surgery that could have been delayed or avoided. Regardless of dilation, initial stricture traversal allows for a complete assessment of disease extent, severity, and associated complications. It also facilitates post-traversal dilation, decreasing the risk of mucosal trauma or perforation caused by blindly passing the balloon catheter into a diseased or sharply angulated section of the bowel. The proper pre-dilation assessment also minimizes the risk of dilating fistula tracts or blind loops of the bowel in side-to-side anastomosis, which can be challenging to assess intraluminally. Furthermore, dilating multiple strictures at the time of scope withdrawal decreases the need for repeated re-insertions of the dilation catheter (i.e. upon scope withdrawal, the catheter remains advanced and is simply inflated once dragged into place) reducing procedure time and the likelihood of catheter rupture/damage.
Of note, we do not use scope caps or distal attachment devices when undertaking BAE; however, this may be of utility in stricture assessment, traversal, and dilation. A recent publication from Oguro et al. 37 discusses a novel calibrated transparent hood, which not only aids in initial stricture measurement but also due to its conical shape, likely provides increased ease of pre-dilation traversal. Our center currently does not have access to this tool.
Single-balloon endoscopy versus double-balloon endoscopy
Comparing SBE and DBE outcomes was a secondary outcome in this retrospective study. While both performed well, SBE had a higher rate of stricture traversal (on initial BAE) and post-traversal dilation, and larger mean diameter dilation. Although this is a retrospective study that cannot assess superiority, SBE may have some performance advantages over DBE when a stricture is encountered endoscopically.
The SBE design likely accounts for the differences in our data namely the absence of the balloon on the scope tip; although the balloon does not add diameter to the scope tip, the rubber bands that secure it add both surface area and a sharper, shouldered edge to the scope tip (Supplemental Table 1). In sub-analysis based on whether the procedure was an initial or a follow-up BAE (Table 5), SBE performed better by all parameters. In the initial BAE group, SBE was more successful in stricture dilation and traversal. In the follow-up group, the success rates between systems were not statistically different, but there was more post-traversal dilation and a higher mean maximum dilation diameter in the SBE group. In both groups, SBE outperformed DBE in stricture traversal. Anecdotally, we noted three cases where CD strictures were not traversable via DBE but were successfully traversed by first withdrawing the DBE scope, leaving the overtube in place, and inserting the SBE scope to perform EBD. This supports the notion that, for complex strictures reachable by either system, the SBE scope may provide procedural advantages. Such precedents should be balanced against the improved depth of insertion and stability offered by the second balloon in the DBE system, which is a major advantage of DBE. To truly compare efficacy, selection must be randomized and assessed prospectively. Finally, if the balloons are adhered to by another method such as with vinyl tape (personal communication with Dr H. Yamamoto), the DBE would likely perform similarly and still provide deeper enteroscopy, stability, etc. There are also potential benefits from using the tip balloon to inflate and perform fluoroscopic contrast studies with the double-balloon scope to delineate stricture and bowel anatomy by preventing backflow of contrast. As stated, our experience is non-fluoroscopic, so this is not a technique we employ at our center. Of final note, the overtube balloon on the SBE is silicon and thicker than the latex found on the DBE. This may hamper overall scope passage through strictures. There is a benefit if patients have documented latex allergy, and use of the DBE would be contra-indicated.
The comparison of SBE to DBE is limited in that it only looks at strictures that were encountered, not accounting for overall stricture access. It may be that DBE can access more strictures overall due to the depth of insertion and facilitate a more complete exam of a patient’s disease. Our finding here simply assesses the technical aspects of intra-procedural dilation, not the other aspects of the endoscopic assessment. Furthermore, DBE was potentially selected for more complicated cases, with strictures that required deeper insertion and were more technically challenging.
Contemporary literature suggests that EBD via BAE is a safe procedure for treating small bowel CD,30–32,34 which our results corroborate with an overall minor event rate of 3.8%. When comparing modalities, Wadhwa et al. 35 noted equivalent adverse event rates after endoscopic investigation (0.6% SBE and 1.1% DBE), and similar studies have shown no difference in complication rate.38–43 Our study found that SBE had a slightly lower rate of adverse events (0.6%) versus DBE (1.1%; p = 0.61) but no significant SAE with either system. Again, as a retrospective study, these findings are simply observational.
Limitations
Data were collected and analyzed retrospectively, limiting the study. Future studies should be prospective, ideally as randomized controlled trials, while collecting intraprocedural and post-procedural dilation outcomes (e.g. immediate success, complications, surgery-free rates, pre/post-operative obstructive symptoms, and pain scores to gauge long-term clinical efficacy). Some of our outcome data were recently published as part of a systematic review and meta-analysis. 34 Our complete clinical outcome data are being collected and compiled as part of a more extensive study on the clinical impact of BAE in CD. The data are primarily a single-operator experience (Dr BPH) for >85% of the cases, possibly limiting the generalizability of the results, but the findings are consistent with current literature.
Conclusion
EBD via BAE is a safe therapeutic procedure in small bowel CD with a high intra-procedural success rate. Both SBE and DBE were highly effective tools for this indication and SBE had a higher rate of stricture traversability in our secondary analysis, in patients undergoing initial enteroscopy. This was not a study designed to assess superiority, and this finding would need prospective, controlled studies to be further investigated. We hope this data and the description of our dilation approach and technique provide technical guidance in performing these procedures and support an increasing role for BAE in CD management.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241230904 – Supplemental material for Stricture dilation via balloon-assisted endoscopy in Crohn’s disease: approach and intraprocedural outcomes with the single-balloon and double-balloon systems
Supplemental material, sj-docx-1-tag-10.1177_17562848241230904 for Stricture dilation via balloon-assisted endoscopy in Crohn’s disease: approach and intraprocedural outcomes with the single-balloon and double-balloon systems by Brendan P. Halloran, Matthew Reeson, Christopher Teshima, Karen Kroeker, Vivian Huang, Levinus Dieleman, Peter Holmes, Daniel C. Baumgart, Karen Wong, Frank Hoentjen, Farhad Peerani and Sergio Zepeda-Gomez in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848241230904 – Supplemental material for Stricture dilation via balloon-assisted endoscopy in Crohn’s disease: approach and intraprocedural outcomes with the single-balloon and double-balloon systems
Supplemental material, sj-docx-2-tag-10.1177_17562848241230904 for Stricture dilation via balloon-assisted endoscopy in Crohn’s disease: approach and intraprocedural outcomes with the single-balloon and double-balloon systems by Brendan P. Halloran, Matthew Reeson, Christopher Teshima, Karen Kroeker, Vivian Huang, Levinus Dieleman, Peter Holmes, Daniel C. Baumgart, Karen Wong, Frank Hoentjen, Farhad Peerani and Sergio Zepeda-Gomez in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to acknowlege the Inflammtory Bowel Disease Unit, and all its affiliated personel, at the Zeidler Ledcor Centre and the Universtity of Alberta Hopsital Al Owens Endoscopy Suite, and all the affiliated personel; Both have been intrinsically important to the management of these patients and the generation of this data. Thank you to Maura Halloran and Sylvia Mellott for writing assistance. Finally, we would like to acknowledge Dr. Richard Fedorak for his support, mentorship and belief in the small bowel program at the University of Alberta hospital. His vision made all of this possible.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.