
Abstract
Methods:
Suboptimal bowel preparation, present in over 20% of colonoscopies, can severely compromise the effectiveness of the colonoscopy procedure. We surveyed 93 primarily urban minority men and women who underwent asymptomatic ‘screening’ colonoscopy regarding their precolonoscopy bowel-preparation experience.
Results:
Print materials alone (39.8%) and in-person verbal instructions alone (35.5%) were reportedly the most common modes of instruction from the gastroenterologists. Liquid-containing laxative (70.6%) was the most common laxative agent; a clear liquid diet (69.6%) the most common dietary restriction. Almost half of the participants mentioned ‘getting the laxative down’ as one of the hardest parts of the preparation; 40.9% mentioned dietary restrictions. The 24.7% who mentioned ‘understanding the instructions’ as one of the hardest parts were more likely to be non-US born and to have lower education and income. There was no relationship between difficulty in understanding instructions and mode of instruction or preparation protocol. One quarter suggested that a smaller volume and/or more palatable liquid would have made the preparation easier. Three quarters agreed that it would have been helpful to have someone to guide them through the preparation process.
Conclusions:
These findings suggest a variety of opportunities for both physician- and patient-directed educational interventions to promote higher rates of optimal colonoscopy bowel preparation.
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer-related deaths that affects both men and women in the USA [American Cancer Society, 2013]. Approximately 102,480 cases of colon cancer and 40,340 cases of rectal cancer occurred in 2012 [American Cancer Society, 2013]. CRC screening with colonoscopy provides the opportunity to remove precancerous polyps, thereby reducing mortality [Zauber et al. 2012]. The American College of Gastroenterology advocates colonoscopy as a preferred screening method for CRC [Rex et al. 2009], and the American Cancer Society places colonoscopy along with other tests on the preferred tier of methods [Levin et al. 2008]. A recent report indicated that CRC screening in the USA increased 13% between 2002 and 2010 among 50–75 year olds [CDC, 2011], and that both CRC incidence and mortality have recently declined [CDC, 2011].
While these trends are encouraging, suboptimal bowel preparation seriously compromises the medical value of a colonoscopy [Harewood et al. 2003; Froehlich et al. 2005; Lieberman et al. 2005], and is estimated to be present in over 20% of colonoscopies [Harewood et al. 2003]. In one recent study, nearly 34% of the 133 patients who underwent a repeat colonoscopy due to inadequate preparation were found to have at least one adenoma [Chokshi et al. 2012]. In another study, based on patients who returned for a second procedure due to an initially fair or poor bowel preparation, an adenoma miss rate of 42% was found (number of lesions found on second procedure/total found on both procedures) [Lebwohl et al. 2011a]. Poor bowel preparation also leads to increased cost due to additional procedural time, more procedures, and shorter time intervals between procedures [Ben-Horin et al. 2007; Rex et al. 2002]. Furthermore, evidence suggests that those who are most likely to exhibit inadequate bowel preparation, namely those with lower socio-economic status [Lebwohl et al. 2010], are less likely to receive CRC screening [Richardson et al. 2010], and to be diagnosed at an early stage of disease [Parikh-Patel et al. 2006], when treatment is far more effective.
Despite the importance of adequate bowel preparation to help ensure the medical benefits of colonoscopy screening, we did not identify any published studies describing challenges reported by urban minority patients’ in following bowel preparation instructions. There has recently been increasing ‘navigation’ to help ensure patients attend their scheduled colonoscopy and that they understand the bowel-preparation regimen, but high rates of suboptimal preparation observed in settings that include patient navigators indicate the need for improvement. To facilitate an evidence-based approach to intervention development, we sought to improve understanding about patients’ bowel-preparation experience by interviewing a sample of individuals who had received an asymptomatic ‘screening’ colonoscopy: how instructions were conveyed, which protocols were followed, which aspects of preparation were most difficult to adhere to, what suggestions were offered to improve the experience.
Methods
This cross-sectional study was ancillary to a randomized trial that evaluated alternative interventions to increase CRC screening rates among ‘unscreened’ members (or spouses) of a large healthcare workers union in the New York metropolitan area. The colonoscopy procedure was a fully covered benefit. Individuals between ages 50 years and 75 years were considered ‘unscreened’ if they had not had a colonoscopy within the past 10 years or a three-sample home stool test in the past year. In the course of recruiting ‘unscreened’ individuals, we collected telephone survey data from the first 100 ‘screened’ individuals who agreed to complete a lengthy (approximately 40 min) phone interview. These data were collected in 2010. One individual had been screened by a home stool test and six colonoscopies were not asymptomatic, leaving a sample of n = 93 for this report. This study took place in the New York metropolitan area and was approved by the Institutional Review Boards at William Paterson University, Columbia University Teachers College and Columbia University Medical Center.
Results
The sample had a mean age of 59.8 years, range = 50–74. Most were female (80.6%), self-identified as African-American (64.5%) and non-US born (83.9%) (> 65% were from the Caribbean). Around 61% reported education of high school or less; 69.9% reported an annual household income of US$50,000 or less.
Print materials alone (39.8%) and in-person verbal instructions alone (35.5%) were reportedly the most common modes of instruction for precolonoscopy bowel preparation from the gastroenterologists’ office; 14.0% reportedly received both print and verbal instruction. Other modes of communicating instructions were less common (Table 1). Most participants (84.8%) required a prescription for their preparation. Liquid laxative (46.7%) was the most common laxative agent, followed by a liquid and pill combination (23.9%), and concentrated liquid requiring dilution (18.5%). A clear liquid diet (69.6%) was by far the most common dietary restriction. Nine participants (9.8%) mentioned no dietary restrictions. About 45% mentioned ‘getting the laxative down’ as one of the most difficult aspects of the preparation (Table 2). There were no significant differences in laxative agent between those who did so and those who did not. About 41% mentioned dietary restrictions, and those who did so were more likely than those who did not to report a dietary regimen stipulating clear liquids (94.7% versus 69.1%, chi square test = 7.58, p = .006). There were no significant relationships between difficulty in getting the laxative down or with dietary restrictions and age, gender, being US born, education, or income.
Colonoscopy bowel-preparation protocols reported by n = 93 primarily urban minority males and females.
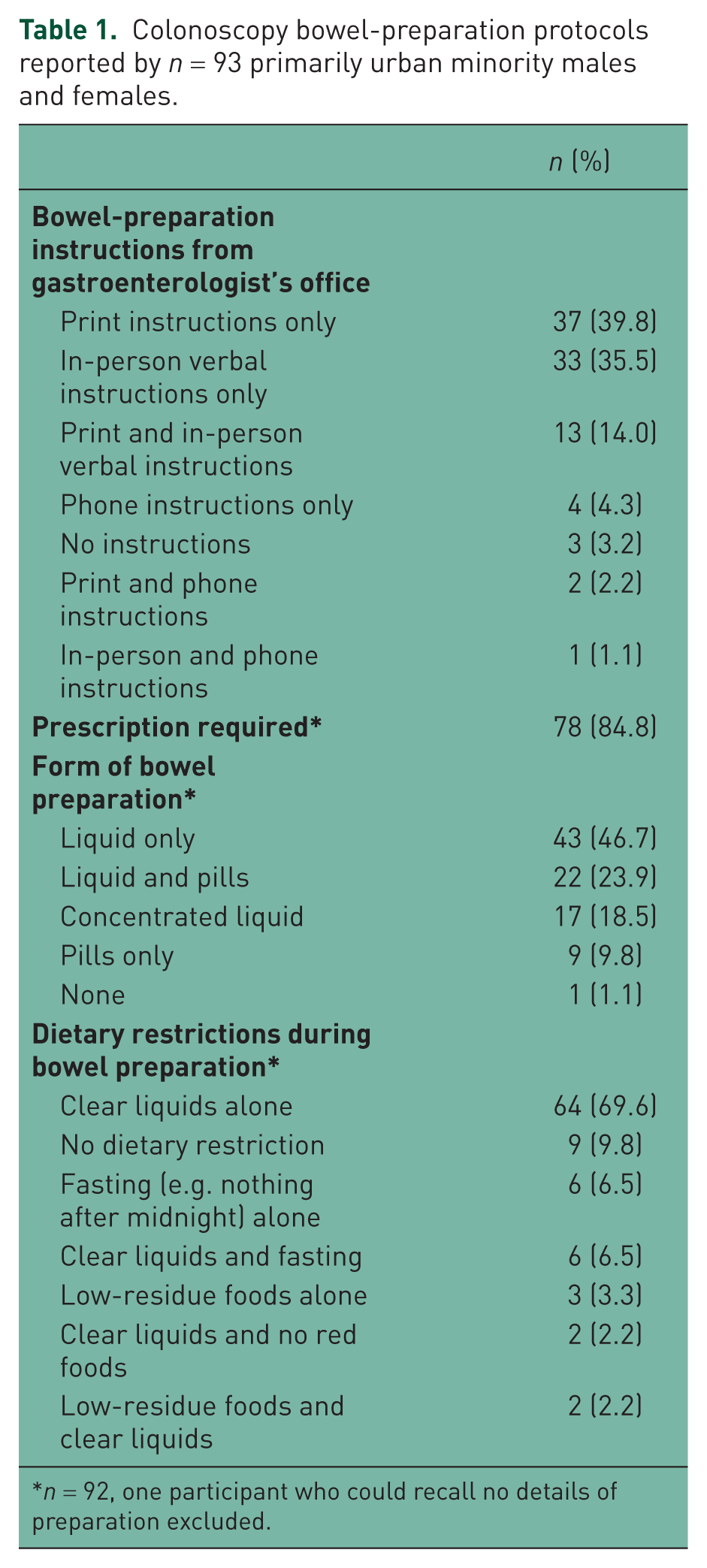
n = 92, one participant who could recall no details of preparation excluded.
Hardest parts of colonoscopy-bowel preparation and suggestions for improvement among n = 93 primarily urban minority males and females.

Open-ended question; more than one response possible. Columns do not sum to 100%.
One quarter mentioned ‘understanding the instructions’ as one of the hardest parts of the preparation experience, and those who did so were more likely to be non-US born (100% versus 78.6%, chi square test = 4.40, p = .036), to have high school or less education (82.6% versus 55.9%, chi square test = 4.17, p = .041), and to have an annual family income of less than US$50,000 (100% versus 72.1%, chi square test = 5.79, p = .016). There were no significant relationships between difficulty in understanding instructions and age, gender, mode of instruction, or preparation protocol.
The most common suggestions for improvement in the colonoscopy-preparation experience were a smaller volume of liquid or more palatable liquid (26.9%), and more food (19.4%) (Table 2). Over three quarters (76.3%) agreed that it would have been helpful to have someone to talk with to guide them through the preparation. All but one of these 71 individuals reported that they had difficulty understanding instructions.
Discussion
Our findings suggest a variety of opportunities for both physician and patient-directed educational interventions. Respondents reported that the most difficult aspects of bowel preparation were ‘getting the laxative down’ and that a smaller volume, or more palatable liquid, would have made the experience easier. Dividing the large volume of electrolyte lavage solution (PEG) into two doses may enhance patient tolerance [Kilgore et al. 2011]. Unflavored lavage solutions can be coupled with flavoring such as lemonade or iced tea-flavored Crystal Light mix to increase palatability. Low-volume PEG with bisacodyl (e.g. HalfLytely) may be equally effective as and better tolerated than standard 4-L PEG regimens [Adams et al. 1994; Sharma et al. 1997]. Pills alone as a laxative agent was uncommon in this sample (9.8%). The extent to which gastroenterologists tailor their prescribed regimens to both patient comorbidities and to stated preferences may facilitate more optimal bowel preparation. Patients, for their part, should be aware that they have options.
One quarter of respondents reported having difficulty understanding the bowel-preparation instructions, and these respondents were more likely to be non-US born and to have lower income and education. Since most gastroenterologists’ offices are distributing print materials (the most common source of bowel instruction in this sample) it is important that these materials be deliberately tailored to the population served. Over three quarters of respondents agreed that it would have been helpful to have someone to talk with to guide them through the bowel preparation. Patient–directed interventions, such as patient navigators [Lebwohl et al. 2011b; Christie et al. 2008; Chen et al. 2008], and tailored telephone education [Basch et al. 2006], have been used with some success in helping patients overcome many barriers to CRC screening (e.g. financial, cultural, emotional), and warrant testing to assess their value for improving bowel preparation. We only identified two studies in the published literature that evaluated an intervention to assist patients in understanding and adhering to the prescribed bowel-preparation protocol [Spiegel et al. 2011; Liu et al. 2013].
Poor bowel preparation compromises the population-wide, public-health benefits of CRC screening. As CRC-screening colonoscopy rates rise, increased emphasis is needed to help ensure the quality of these procedures, and improved bowel preparation is an important element that has been overlooked. This is particularly needed among those with a lower level of income and education.
Despite its importance for helping to ensure the quality of colonoscopy procedures, there is a paucity of research on the patient’s perspective on bowel preparation. This study begins to address that gap, but the findings must be interpreted in light of the limitations. We collected data in one geographic area from a small sample, the design was cross sectional, receipt of colonoscopy was self-reported, and participants had to rely on memory to recall their experience. Nevertheless, our findings begin to identify patients’ challenges in adhering to bowel preparation and to suggest strategies for addressing these challenges.
Footnotes
Funding
This work was supported by the American Cancer Society (grant number RSGT-09-012-01-CPPB), and the ART fund at William Paterson University.
Conflict of interest statement
The authors report no conflicts of interest in preparing this article.