
Abstract
Introduction:
The quality of the bowel preparation directly influences colonoscopy effectiveness. Quality indicators are widely employed to monitor operator performance and to gauge colonoscopy effectiveness. Some have suggested that the enumeration of the mean number of adenomas per colonoscopy (MNA) may be a more useful measure of bowel preparation quality, but evidence of the utility of this metric is limited. The relationship between bowel preparation quality and MNA was assessed.
Methods:
Records of adult patients, aged 50–74 years, who had undergone a screening colonoscopy in a 6 month period at a hospital-based endoscopy suite in New York City were examined. Excluded were those who were symptomatic or having a colonoscopy for surveillance. Patient and procedural characteristics and clinical findings were abstracted from the endoscopy database. Bowel preparation quality was recorded as excellent, good, fair and poor. Histology and size of polyps removed were gathered from pathology reports. MNA was calculated and incident rate ratios assessing the relationship between bowel preparation quality, MNA, and covariates was calculated using Poisson regression.
Results:
A total of 2422 colonoscopies were identified; 815 (33.6%) were screening colonoscopies among average risk individuals, 50–74 years; 203 (24.9%) had ≥1 adenomas; and 666 (81.7%) had excellent/good preparation quality. Overall MNA was 0.34 [standard deviation (SD) 0.68] and MNA was greater among those >60 years [incident rate ratio (IRR) 1.89, 95% confidence interval (CI) 1.48–2.42), males (IRR 1.60, 95%CI 1.26–2.04) and those with good bowel preparation (IRR 2.54, 95%CI 1.04–6.16). Among those with ≥1 adenomas, MNA was 1.48 (SD 1.05) for excellent and 1.00 (SD 0.00) for poor quality preparation (p = 0.55).
Conclusions:
We found that MNA is sensitive to changes in bowel preparation with higher MNA among those with good bowel preparation compared with those with poor preparation. Our evidence suggests MNA was particularly sensitive when restricted to only those in whom adenomas were seen.
Introduction
The incidence and mortality due to colorectal cancer, the third most commonly diagnosed cancer in the United States, has been steadily declining over the past several decades due in large part to increased uptake of screening, particularly with colonoscopy [Edwards et al. 2010; American Cancer Society, 2013]. Colonoscopy reduces colorectal cancer risk and mortality by allowing for the identification and removal of precancerous adenomas [Winawer et al. 1993].
Background
Adenomas are the premalignant lesions that precede the majority of colorectal cancers and, while every adenoma has the capacity to become cancer, few actually do [Risio, 2010]. Nonetheless, any adenoma detected, easily recognizable by their size, architectural growth, type, grade and dysplasia [Risio, 2010] is regarded as a potential colorectal cancer threat and removed during colonoscopy. The most consistent of predictors of the prevalence of adenomas are older age and male gender [Rex, 1995; Imperiale et al. 2000; Lieberman et al. 2000; Rex et al. 2002; Heitman et al. 2009; Corley et al. 2013], but the risk of adenomas is also increased among those with a personal history of cigarette smoking [Anderson et al. 2003; Reid et al. 2003] and a family history of colorectal cancer [Rex et al. 1993; Lynch et al. 2003].
The endoscopist’s ability to visualize the colonic mucosa is critically important to the effectiveness of colonoscopy. Operator skill, experience and diligence in examining the full length of the colon, as well as the use of imaging adjuncts enhances visualization, but equally essential is the quality of the bowel preparation [Rex et al. 2006]. Bowel preparation quality is, in turn, contingent upon various patient-related factors (age and gender for example), the tolerability and efficacy of the purgative regimen, and aspects the procedure itself such as having a morning versus afternoon procedure [Ness et al. 2001; Sanaka et al. 2006; Wexner et al. 2006; Belsey et al. 2007; Siddiqui et al. 2009]. That there is an association between bowel preparation quality and the detection of adenomas exists has been noted by others. Froehlich and colleagues in the European Panel of Appropriateness of Gastrointestinal Endoscopy European Multicenter Study examined the impact of cleansing quality on colonoscopy diagnostic yield for more than 5800 colonoscopies and found that polyps were more likely detected among those with high-quality cleansing compared with low-quality [odds ratio (OR 1.46, 95% confidence interval (CI) 1.11–1.93) [Froehlich et al. 2005]. In a review of 113,272 colonoscopies in the Clinical Outcomes Research Initiative (CORI) database, Harewood and colleagues demonstrated that adequate preparation (excellent or good) was associated with the detection of colonic lesions (OR 1.21, 95% CI 1.16–1.25) compared with inadequate preparation (fair or poor) [Harewood et al. 2003].
Quality indicators are widely employed to monitor operator performance and gauge colonoscopy effectiveness. Typically they include assessing cecal intubation using photodocumentation of landmarks during screening procedures among healthy persons (target 95%); individual endoscopist adenoma detection rate (ADR) ≥25% in men and ≥15% in women aged 50 years and older; and when ADR is low, assessment of mean withdrawal time where optimal withdrawal time is 6 minutes or more [Rex et al. 2006]. Of these, ADR is considered the priority indicator and is the most widely used of the quality indicators as it focuses on the primary reason for performing screening colonoscopy – detection and removal of precancerous lesions. Derived by dividing the number of patients in whom any adenoma has been detected by the total number of colonoscopies performed, ADR is a binary measure (0 versus ≥1 adenomas) that provides no information on total adenomas removed. However, some have suggested that enumeration of overall number of adenomas per colonoscopy [Wang et al. 2011; Lee et al. 2012; Rembacken et al. 2012; Denis et al. 2014], calculated by dividing the total number of adenomas detected by the total number of colonoscopies performed, may be a more useful measure of adenoma detection [Rex et al. 2006; Wang et al. 2011; Lee et al. 2012; Rembacken et al. 2012; Kahi et al. 2014]. Evidence regarding the utility of this metric is limited. Only recently has the mean number of adenomas (MNA) per colonoscopy, overall and per positive procedure, been used to assess colonoscopy quality [Lee et al. 2012, 2013, Denis et al. 2014]. In this study we sought to evaluate the relationship between MNA and bowel preparation quality among persons undergoing screening colonoscopy at a large, tertiary care center in New York City.
Materials and methods
The records of outpatients aged 50–74 years who had undergone a colonoscopy in a 6-month period between 1 September 2012 and 28 February 2013 at Columbia University Medical Center were extracted from the electronic endoscopy database. Those with a procedural indication of screening colonoscopy were selected for analysis. Indications such as family history of colorectal cancer or polyps in first degree relative(s), first degree relative(s) before the age of 60 years, multiple second degree relatives, and distant relatives were also included (see Appendix). Excluded were indications of abdominal pain/distress, abnormal computerized tomography (CT) or positron emission tomography (PET) scan of the abdomen, anemia, celiac disease, change in bowel habits, Crohn’s disease, chronic constipation or diarrhea, diverticulitis, hematochezia, heme positive stool, hereditary nonpolyposis colorectal cancer, high risk surveillance, presurgical assessment for organ transplant, personal history of colorectal cancer or polyps, and rectal bleeding. Records of the pathology department were subsequently queried to assemble a list of patients using the above criteria whose pathology reports included a diagnosis of benign neoplasm of the colon and/or benign neoplasm of the rectum. Comparison of the two lists ensured completeness of the data extraction and created a definitive roster of patients diagnosed with adenomas.
The following information was abstracted from the endoscopy database: age; gender; examination date; time of procedure (morning prior to 12:00 versus afternoon); procedural difficulty (not difficult, somewhat difficult, moderately difficult, or difficult); patient’s tolerance of the procedure (tolerated well versus not tolerated well); number of adenomas; and size (<10 mm versus ≥10 mm). Based on the American Society for Gastrointestinal Endoscopy (ASGE) and American College of Gastroenterology (ACG) Taskforce on Quality in Endoscopy recommendations [Rex et al. 2006], bowel preparation quality was assessed as excellent if no or minimal amounts of solid stool were present and suctioning was required for only small amounts of clear liquid; good if no or minimal amounts of solid stool were present and suctioning was required for large amounts of clear liquid; fair if semisolid debris was present that was difficult in removing; and poor if solid or semisolid debris was present that could not be cleared sufficiently.
In 10.3% (21/203) of patients who had adenomas detected, multiple polyps submitted in one fixative jar for histological review were counted conservatively as one adenoma [Lebwohl et al. 2012]. From the pathology reports, polyps histologically classified as adenomas were tabulated and adenomas of the tubulovillous or villous type, tissue with high-grade dysplasia, or adenomas greater than or equal to 10 mm in size were classified as advanced adenomas. All colonoscopy and pathology reports were manually reviewed by a single auditor (G.C.H.). A random 20% sample was re-audited by two gastroenterologists (B.L. and R.M.R.) and Cohen’s Kappa statistic was calculated to demonstrate inter-rater reliability of the recording of bowel preparation quality (K = 0.93) and number of adenomas detected (K = 0.83). Cecal intubation rate was 96.9%. This study was reviewed and approved by the medical center’s institutional review board.
Data analysis
The MNA per colonoscopy was defined as the total number of adenomas detected divided by the number of colonoscopies performed. We examined the relationship between patient demographic and procedure-related characteristics and MNA using Chi square and Student’s t tests. The overall MNA was calculated in addition to MNA stratified by age, gender and preparation quality using analysis of variance (ANOVA). A similar subanalysis among only those in whom ≥1 adenomas were detected was also performed. Using Poisson regression, we calculated incident rate ratios (IRR) to assess the relationship between age, gender and bowel preparation quality, and MNA. Lastly, we performed a secondary analysis to compare ADR, determined by dividing the number of patients with at least one adenoma by the total number of colonoscopies, and MNA. All analyses were conducted using IBM SPSS version 21.
Results
A total of 2442 colonoscopies were performed during the 6-month period. Of these, 232 (9.6%) were inpatients, 606 (25.0%) were less than 50 or greater than 74 years of age, and 769 (31.7%) were for indications other than screening (refer to the Appendix for a complete listing of indications). The remaining 815 screening colonoscopies were performed by 45 providers (38 attending gastroenterologists and seven fellows). The majority of patients were younger than 60 years (52.5%) and female (57.4%) (Table 1). Most procedures were performed in the morning before 12:00 (59.1%), had ‘good’ bowel preparation quality (65.9%), and the suite-wide cecal intubation rate was 96.9%. Of these screening colonoscopies, 203 (24.9%) patients had one or more adenomas detected.
Characteristics of outpatients (n = 815) by number of adenomas detected who had undergone screening colonoscopy between 1 September 2012 and 28 February 2013.
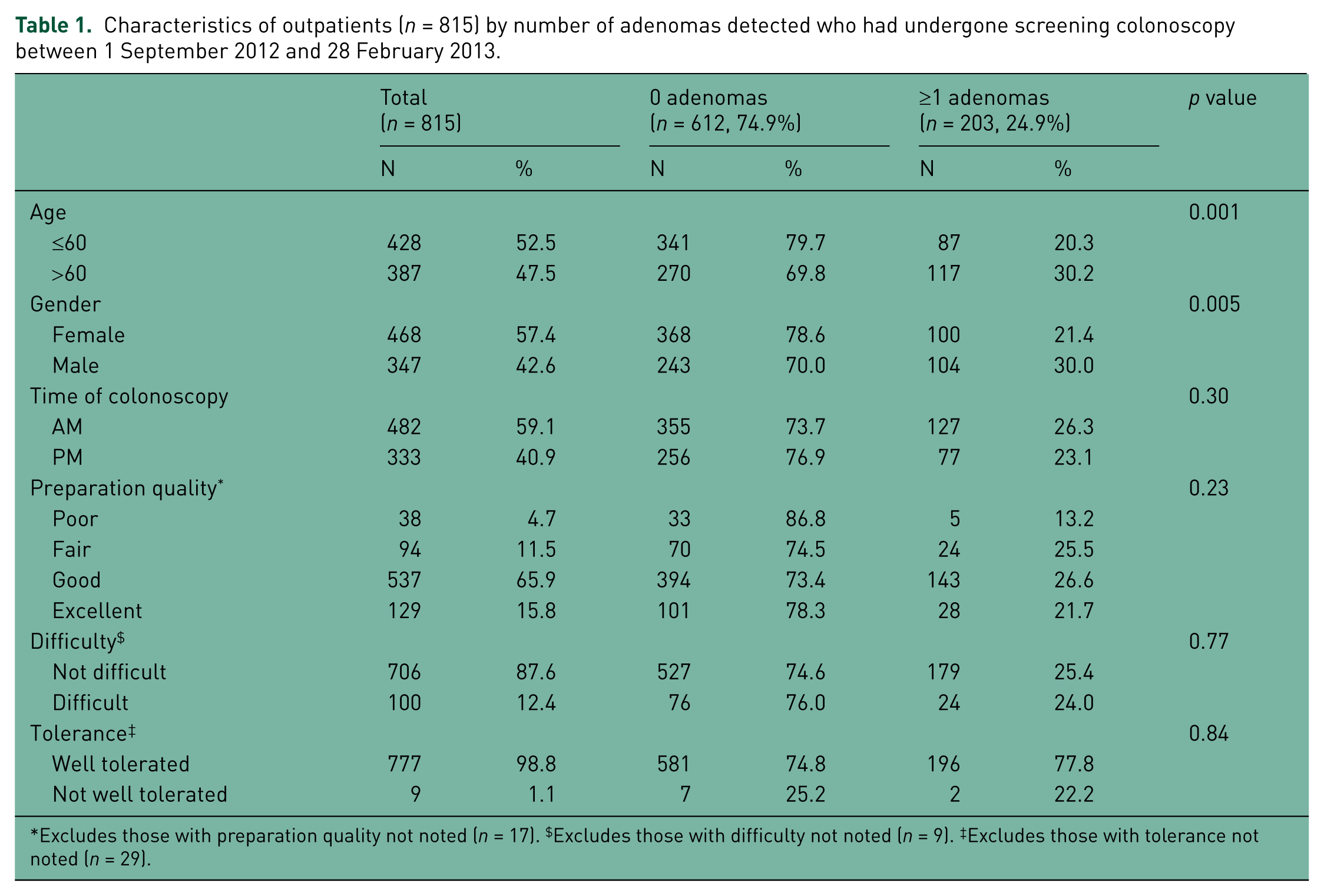
Excludes those with preparation quality not noted (n = 17). $Excludes those with difficulty not noted (n = 9). ‡Excludes those with tolerance not noted (n = 29).
Of patients in whom adenomas were detected, 73.9% had only a single adenoma (Table 2). The majority of the adenomas detected were of the adenomatous/tubular type (88.7%) and were nonadvanced (83.2%). The MNA overall was 0.34 [standard deviation (SD) 0.68] (Table 3). For patients >60 years of age, the MNA was nearly double that found in younger patients [0.44 (SD 0.82) versus 0.24 (SD 0.52), p < 0.001] and by gender; the MNA for males was significantly greater than that of females [0.43 (SD 0.80) versus 0.26 (SD 0.57), p <0.001]. The MNA among those with poor quality bowel preparation was 0.13 compared with 0.31, 0.34 and 0.36 for those with excellent, good or fair preparations, respectively (Table 3) (p = 0.25).
Adenoma characteristics among outpatients (n = 203) in whom adenomas were detected with screening colonoscopy between 1 September 2012 and 28 February 2013.

A total of 274 adenomas were detected among 203 patients. ‡Includes villous and tubulovillous adenomas, adenomas with high grade dysplasia, and adenomas ≥10 mm in size.
Mean number of adenomas per colonoscopy and Poisson regression analysis by select patient characteristics among outpatients (n = 815) who had undergone screening colonoscopy between 1 September 2012 and 28 February 2013.

Excludes those with preparation quality not noted (n = 17). Note: Bolded numbers represent statistically significant associations.
CI, confidence interval; IRR, incident rate ratio.
In our subanalysis among only patients who had one or more adenomas detected, a linear association between MNA and age was observed with 1.11 (SD 0.37) adenomas detected in the youngest age group (50–55 years) rising to 1.62 (SD 0.94) for the 71–75 year-old group (p = 0.019) (Figure 1). MNA was highest among procedures with excellent quality preparations [1.48 (SD 1.05)], was lower but equivalent for good and fair preparations [1.34 (SD 0.68) and 1.33 (SD 0.48), respectively], and still lower for poor preparation quality [1.00 (SD 0.00), p = 0.55]. When examining the relationship between bowel preparation quality and mean number of proximal adenomas [excellent: 1.20 (SD 0.63); good: 1.26 (SD 0.55); fair: 1.28 (SD 0.47); poor: 1.00 (SD 0.00), p = 0.78], and between preparation quality and mean number of distal adenomas [excellent: 1.00 (SD 0.00); good: 1.13 (SD 0.43)]; fair: 1.14 ([SD 0.38); poor: n = 0, p = 0.61], no trend was observed. Secondary analysis showed the ADR was higher in older patients (30.2% 60 years or older versus 20.3% younger than 60 years, p = 0.001) and male patients (30.0% versus females 21.4%, p = 0.005). The overall ADR was 25.0%; the ADR for males was 28.8% and 22.2% for females. ADR increased with age with 17.5% for 50–55 year-olds and 31.9% for 71–75 year-olds (p = 0.007). Stratified by level of bowel preparation quality, the ADR was 21.7% for excellent preparation, 26.6% for good, 25.5% for fair and 13.1% for poor preparations. In the regression analysis, adjusted for age and gender, there was no statistically significant association between ADR and bowel preparation quality.
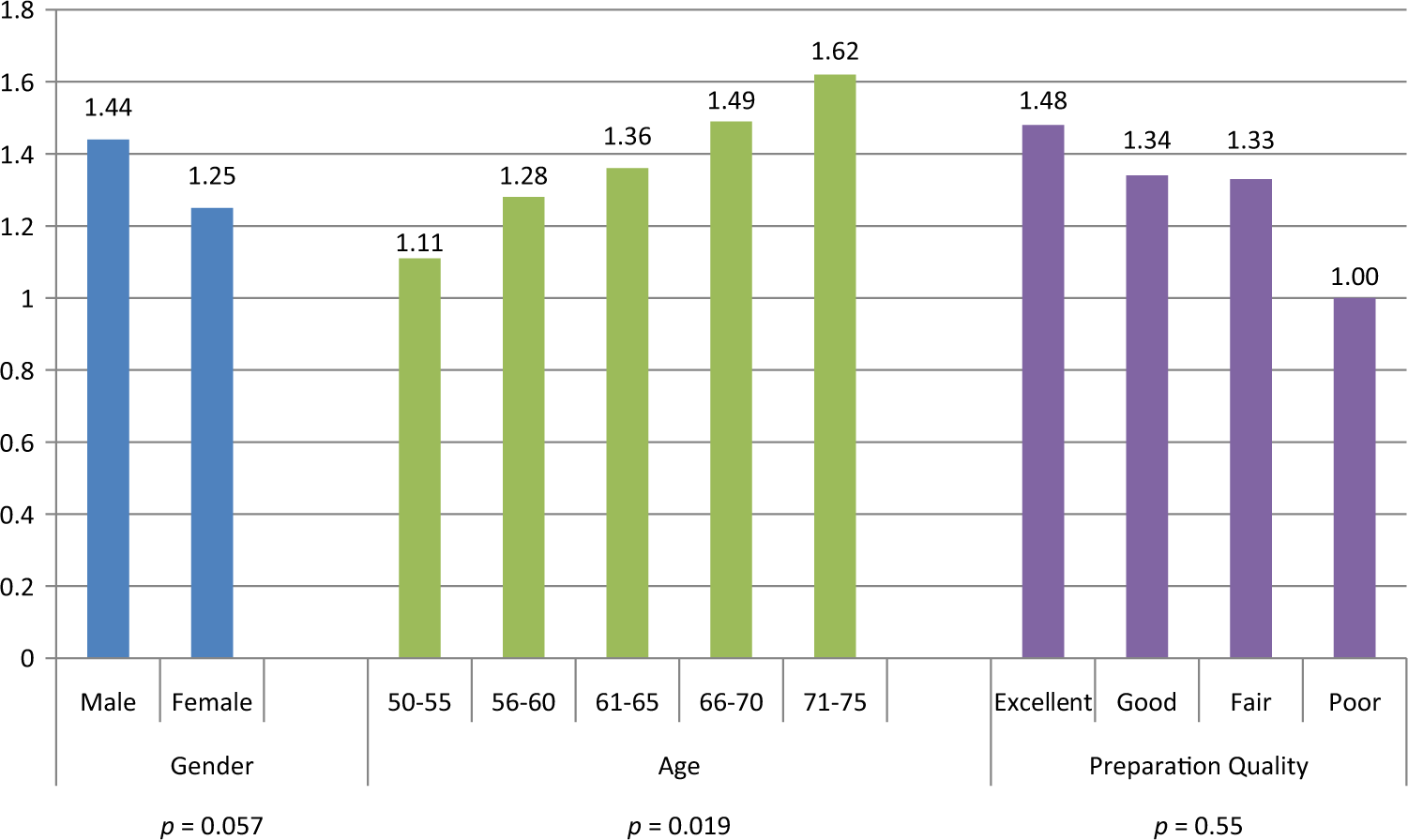
Mean number of adenomas (n = 276) by select patient characteristics among only patients in whom adenomas were detected (n = 203).
Discussion
Our findings demonstrate that the MNA is significantly greater for those with ‘good’ bowel preparation compared with those with ‘poor’ preparation. We also found that increasing age (>60 years old) and male gender were associated with greater numbers of per patient adenomas, which coincides with reports of higher adenoma detection noted in the literature [Rex, 1995; Imperiale et al. 2000; Lieberman et al. 2000; Rex et al. 2002; Heitman et al. 2009; Corley et al. 2013], among older individuals (>60 years) and for males. Our results suggest that the MNA may be sensitive to fine gradations in preparation quality, particularly among those in whom adenomas were seen, and may prove to be a useful measure of the effectiveness of colonoscopy as proposed by others [Rex et al. 2006; Wang et al. 2011; Lee et al. 2012; Rembacken et al. 2012].
Several studies have utilized MNA as an indicator of the quality of colonoscopy and support the efficacy of MNA as a sensitive metric to evaluate bowel preparation quality, but these studies have been conducted almost exclusively in the context of stool-based colorectal cancer screening programs [Lee et al. 2012, 2013; Denis et al. 2014]. Since the risk of adenoma detection on colonoscopy following a positive fecal-based colorectal cancer screening test is substantially greater [UK Colorectal Cancer Screening Pilot Group, 2004] than that associated with a screening colonoscopy of an average risk individual, these studies generally yielded a higher MNA than those found in our study, overall and among only those with adenomas detected. Lee and colleagues in a study measuring the quality of colonoscopy following a positive fecal occult blood test, reported the mean number of adenomas per procedure (MAP) was 0.91 overall and the mean number of adenomas per positive procedure (MAP+) was 1.94 compared with our findings of 0.34 and 1.34, respectively [Lee et al. 2012]. Similarly, Denis and colleagues [Denis et al. 2014] used the MNA to establish benchmark rates for colonoscopy quality in a French stool-based colorectal cancer screening program. The range of MNA per colonoscopy varied widely (between 0.36 and 0.98) in this study which the authors attributed to interoperator differences, an observation supported by Wang and colleagues [Wang et al. 2011] who found that adenomas under the curve (AUC) varied based on the setting of the endoscopic practice (academic versus community-based) with AUC of 1.94 in academic settings compared with 1.65 among community-based practices (p < 0.001). Only one study utilized MNA to evaluate a specific colonoscopy procedural aspect as we did. In this study, MAP was used to demonstrate the impact of increased colonoscopy withdrawal time (CWT) and found that MAP increased from 0.77 to 0.94 as CWT increased from 7 to 11 minutes [Lee et al. 2013].
We found that, after adjusting for age and gender, ADR was not associated with level of bowel preparation quality. Results from other studies regarding this association vary. For example, the relationship between ADR and bowel preparation quality was examined in the UK Flexible Sigmoidoscopy Screening Trial in 2006. In this study, ADR was higher in flexible sigmoidoscopy examinations with excellent or good bowel preparations compared with poor (p = 0.02) [Thomas-Gibson et al. 2006]. Another study, also conducted in the UK, evaluated the impact of poor bowel preparation on colonoscopy quality indicators including polyp detection rate (no distinction between neoplastic and non-neoplastic polyps) [Butt et al. 2012]. For good, satisfactory and poor bowel preparation, the polyp detection rate was 20%, 20%, and 16%, respectively, compared with our ADR findings of 26.6%, 25.5% and 13.1% for good, fair and poor quality, respectively, demonstrating that ADR appears to be diminished by a poor preparation, but does not vary significantly among preparations deemed superior to the lowest quality.
This study has several limitations. This study was conducted at a single site, thus limiting the generalizability of our findings to other sites and population groups. Our sample size was relatively small with only 38 patients having poor bowel preparation, which may have limited our ability to detect significant associations between MNA and excellent and fair bowel preparation. Our finding that only good preparation was associated with higher MNA likely reflects that large number of patients with good preparation compared with those with better or worse preparation quality. Intra-observer agreement in rating the bowel preparation quality was not assessed, which may have resulted in misclassification bias. The fact that MNA tends to improve among the highest preparation quality rating suggests that these gradations of quality reflect actual differences, rather than varying subjective impressions of bowel cleanliness. We did not evaluate the impact of gastrointestinal (GI) fellows performing procedures on a subset of our cohort, which may have resulted in higher adenoma detection among select patients [Rogart et al. 2008]. Non-intubation of the cecum is a confounder of the relationship between bowel preparation quality and MNA, as failure to reach the cecum is associated with both the exposure and the outcome. In our study, the cecum was not intubated in only 25 patients (3%). Due to the small number in whom the cecum was not intubated, it is likely that nonintubation had little effect upon our results. This study was also limited in that information regarding the type of purgative prescribed was not available, which may have provided additional insight to the relationship between bowel preparation quality and MNA. Lastly, we conservatively counted multiple adenomas submitted in one fixative jar as a single adenoma. This practice may have resulted in an underestimation of MNA. Strengths of this study include a large sample size and that all adenoma results were histologically confirmed.
To date, no other study has evaluated whether this metric, MNA, is affected by bowel preparation quality. Future studies should test this hypothesis among larger cohorts of gastroenterologists in which the determination of bowel preparation has been standardized [Lai et al. 2009], examine the mean number of right-sided adenomas, evaluate mean number of flat/serrated adenomas and determine the influence of bowel preparation strategies upon MNA. If confirmed, our findings may demonstrate that the mean adenoma count per colonoscopy is an important quality assessment outcome and a potentially useful outcome when testing interventions to improve preparation quality.
Footnotes
Appendix
| Inclusion | Exclusion | |
|---|---|---|
| Indication |
- Colon cancer screening, increased risk - Family history of colorectal cancer or colon polyps in first degree relative, multiple first degree relatives, multiple second degree relatives - Family history of cancer other than colorectal cancer - Personal history of malignant neoplasm other than colorectal cancer - Screening for colon cancer - Screening for malignant neoplasm in colon or rectum - Screening in patient at increased risk |
- Abdominal pain, distress, mass or lump - Abnormal computerized tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET) scan - Anemia - Celiac disease - Chronic diarrhea, change in bowel habits - Colitis - Colon mass - Constipation - Crohn’s disease - Diverticulitis - Follow up of other conditions - Hematochezia - Heme positive stool - High risk colorectal cancer surveillance - History of malignant neoplasm of colon or rectum - Hereditary nonpolyposis colorectal cancer (HNPCC) - Inflammatory bowel disease - Personal history of adenomatous polyps - Pre-operative assessment - Pre-organ transplant evaluation - Surveillance - Therapy of adenomatous polyps in rectum or colon - Weight loss |

Funding
This study was supported in part by a National Institute of Health grant 1U24 CA171524 to G.C.H.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.