
Abstract
Background:
Endoscopic balloon dilatation (EBD) is an effective therapy for caustic-induced gastric outlet obstruction (GOO). Gaining access to the stricture site is the most important step. It is sometimes difficult to negotiate a balloon through the stricture with a front-viewing endoscope due to deformed anatomy of stomach. To overcome this technical difficulty, a side-viewing endoscope can be used. There is limited data regarding the use of side-viewing endoscopes in EBD. We here report on the short-term efficacy and safety of EBD in caustic-induced GOO. In technically difficult cases, a side-viewing endoscope was used for EBD and its efficacy and safety were assessed.
Methods:
The study included 25 patients with caustic-induced GOO. Patients underwent EBD using a through-the-scope balloon. Initial balloon dilatation was performed with a front-viewing endoscope. A side-viewing endoscope was used where negotiation across the stricture failed with a front-viewing endoscope. Dilatation was started at 8 mm diameter and was performed at 1-week intervals. The end point of dilatation was 15 mm diameter.
Results:
In 18 patients successful balloon dilatation was possible with a front-viewing endoscope. A side-viewing endoscope was used in six patients as negotiation across the stricture was not possible with a front-viewing endoscope. In all six patients negotiation across the stricture followed by successful dilatation was successful with a side-viewing endoscope. Of the 25 patients included in this study, 24 (96%) achieved procedural success (18 with a front-viewing endoscope and 6 with a side-viewing endoscope) in 3–9 sessions.
Conclusion:
Our results show that EBD is a safe and effective option for caustic-induced GOO and in difficult cases a side-viewing endoscope can be used to achieve technical success.
Introduction
Gastric outlet obstruction (GOO) is a late complication of caustic ingestion due to pyloric stenosis. Both acid and alkali ingestion can cause GOO due to antral and pyloric scarring [Zargar et al. 1989, 1992]. Surgery has been the standard treatment of caustic-induced GOO [Chaudhary et al. 1996]. Endoscopic balloon dilatation (EBD) is an effective therapy for benign GOO [Boylan and Gradzka, 1999; Kochhar et al. 2004, 2009; Solt et al. 2003]. Gaining access to the stricture site is the most important step for successful EBD. Sometimes, it is difficult to negotiate balloon through stricture with conventional front-viewing endoscope in deformed anatomy of stomach. Owing to excessive cicatrization, the plane of antrum comes at a right angle to the body of the stomach due to shortening of lesser curvature. To overcome this technical difficulty, a side-viewing endoscope can be used in these situations. There is limited data regarding the use of a side-viewing endoscope in EBD and none of the previous studies have commented on this issue.
Here we report on the short-term efficacy and safety of EBD in caustic-induced GOO. In technically difficult cases, a side-viewing endoscope was used for balloon dilation and its efficacy and safety were assessed.
Patients and methods
Patients who presented with symptomatic GOO with postprandial vomiting and narrowing on endoscopy and barium studies were included in this study.
The study included patients with caustic-induced GOO from March 2011 to April 2012. The study design is summarized in Figure 1. Patients who were eligible were subjected to EBD by using a through-the-scope (TTS) balloon. Initial balloon dilatation was performed with a front-viewing endoscope (Olympus GIF-1T160). A side-viewing endoscope (Olympus TJF-160R) was used where negotiation of the TTS balloon across the stricture failed with a front-viewing endoscope.
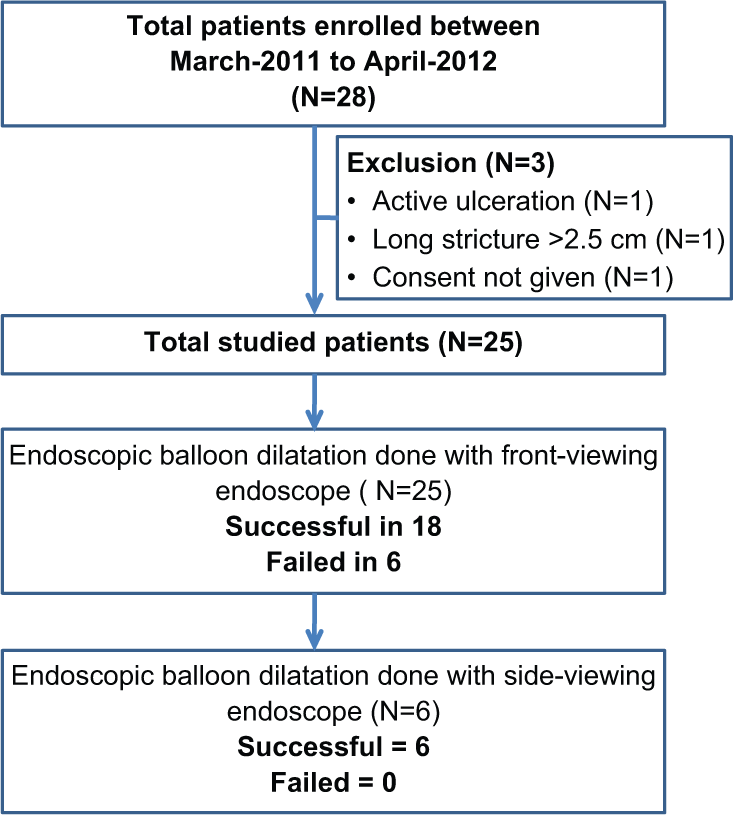
Flow chart summarizing the study design.
Exclusion criteria were: (1) age <14 years; (2) history of caustic ingestion less than 6 weeks previously; (3) active ulceration at the stricture site; (4) >2.5 cm narrowing at the pyloroantral area; and (5) inability to give informed consent.
Informed consent was obtained from each patient at each session, and the study was approved by the Institutional Ethics Committee.
EBD technique
All patients fasted for 12 hour and Ryles’ tube aspiration of gastric contents was performed in every patient. The dilatation was carried out by using a wire-guided TTS controlled radial expansion (CRE) balloon from Boston Scientific Corp, after premedication with 2 ml of intravenous midazolam (1 mg/ml) and 2 ml of n-hyoscine butyl bromide (Buscopan 20 mg/ml).
The balloon was negotiated across the stricture and positioned in the center of the stricture under endoscopic vision. Inflation was performed by using a pressure gun (Alliance inflation device; Boston Scientific) for 60 seconds. After the procedure patients were closely monitored for perforation and bleeding for 24 hours.
Dilatation was performed at 1-week intervals with incremental increase in diameter of the balloon (maximum of three sizes) in each session. Dilatation was started at 8 mm diameter and the end point of dilatation was 15 mm diameter.
Technical success was defined as successful negotiation across the stricture. Procedural success was defined as successful endoscopic dilatation without any major complications and treatment response as relief of obstructive symptoms.
Once the 15 mm end point was achieved, then these patients were further followed up every week for 1 month to record short-term response.
Results
Of the 28 patients with caustic-induced GOO, 25 were subjected to EBD after a period of 7.5 ± 1.7 weeks following caustic ingestion. The details of patients are summarized in Table 1. The mean age of 25 patients was 26 ± 12.8 (range 16–55) years. A total of 22 patients had consumed acid while 3 had consumed alkali.
Patient characteristics.

In 18 patients successful balloon dilatation was performed with a front-viewing endoscope. In the remaining six patients there was deformed anatomy of the stomach and the antrum was at a right angle to the body of the stomach due to excessive cicatrization. We therefore were unable to negotiate the stricture with a front-viewing endoscope, so a side-viewing endoscope was used in these six patients. In all six patients we were able to negotiate the balloon across the stricture followed by successful dilatation with a side-viewing endoscope. All of the patients tolerated the procedure well.
The results of procedure are summarized in Table 2. Of the 25 patients, 24 (96%) achieved procedural success (18 with front-viewing endoscope and 6 with a side-viewing endoscope) in 3–9 (mean 5.2 ± 1.6) sessions.
Results of endoscopic balloon dilatation (N = 25).

A significant complication in the form of a perforation was seen in 1 patient (4%) who underwent urgent surgery. The patient had an uneventful postoperative recovery. Minor complications in the form of self-limiting abdominal pain in 8 patients and minor bleeding in 4 patients were seen. These results are summarized in Table 3.
Complications during endoscopic balloon dilation (N = 13).

All of the patients resumed normal diet and gained weight following a successful procedure. The 24 patients who achieved procedural success were followed up for 1 month to check for recurrence. They all were well at 1 month with no recurrence of their symptoms.
Discussion
Previous studies have shown that EBD is a safe and effective option for caustic-induced GOO [Boylan and Gradzka, 1999; Kochhar et al. 2004, 2009; Solt et al. 2003], however, data regarding this procedure are not very robust.
Our study evaluated the outcome of 25 patients with caustic-induced GOO whose mean age of patient was 26.6 ± 12.8 years. Previous studies had shown that EBD was successful in most patients with corrosive GOO [Kochhar et al. 2009, 2010]. In the study by Kochhar and colleagues [Kochhar et al. 2009] EBD was effective in 39/41 (95.1%) of patients. In our study, successful dilatation was achieved in 24/25 (96%) patients.
In previous studies successful dilatation was achieved in all patients [Kochhar et al. 2009, 2010; Solt et al. 2003]. In our study, despite repeated efforts, we were not able to negotiate the balloon across the stricture in six of our patients when using a front-viewing endoscope. Gastric anatomy was deformed with reduced capacity in all six patients and the level of fibrosis was so extensive that the antrum was at right angle to the body of the stomach. In these difficult cases a side- viewing endoscope was used and we were able to negotiate the balloon across the stricture in all six patients.
The main advantage of the side-viewing endoscope is its large working channel (4.2 mm) and the presence of an elevator which allows adjustments of the balloon position. Our study has shown that balloon dilation with a side-viewing scope is as equally effective and safe as that performed with a front-viewing endoscope. It is important to note that one of the perforations that occurred in our study was made with a front-viewing endoscope. Some patients with corrosive GOO may have associated esophageal stricture. In these patients the risk of perforation with a side-viewing endoscope could be avoided by using a front-viewing endoscope followed by a side-viewing endoscope.
Previous studies have also shown that caustic-induced GOO is more difficult to treat and requires a greater number of sessions as compared with peptic stricture. In our study, the mean number of dilations required to achieve the 15 mm diameter end point was 5.2 ± 1.6, was similar to that observed in the study from Kochhar and colleagues [Kochhar et al. 2009]. The complication rate was also similar to previously reported studies [Kochhar et al. 2004, 2009].
Although long-term follow up was not performed after achieving the end point, patients were followed for up to 1 month. All patients were asymptomatic after this period and none experienced a relapse of symptoms.
In conclusion, our results show that EBD is a safe and effective option for caustic-induced GOO and that in difficult cases a side-viewing endoscope can be used to achieve technical success.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have not conflicts of interest to declare.