
Abstract
Gastroduodenal intussusception is a relatively rare condition in adults and is typically caused by mobile pedunculated submucosal tumors arising from the stomach. Its clinical presentation often includes nonspecific signs of gastric outlet obstruction, such as nausea, vomiting, abdominal pain, epigastric fullness, or abdominal distention. We report a case of gastroduodenal intussusception in a 38-year-old woman who presented with severe anemia but no symptoms of gastric outlet obstruction. The preoperative diagnosis was established through esophagogastroduodenoscopy and computed tomography of the abdomen, and it was confirmed during surgery. Postoperative pathology and immunohistochemistry identified the tumor as a gastric leiomyoma.
Keywords
Introduction
Although intussusception is a common abdominal emergency in children, it is rare in adults, with a reported pediatric:adult ratio exceeding 20:1. 1 Based on the anatomic location, intussusception can be categorized as enteroenteric, colocolic, gastroduodenal, ileocolic, or ileocecal. Gastroduodenal intussusception is the rarest type in adults, with an incidence of approximately 10%, 2 and only a few cases have been reported in children. 3 Like other forms of adult intussusception, gastroduodenal intussusception is typically caused by a definable structural lesion, often pathological, with clinical manifestations that vary depending on the degree of gastric outlet obstruction. Additionally, a few reports have noted that gastroduodenal intussusception can rarely occur after bariatric surgery, particularly gastric plication. 4 This article presents a case of nonobstructive gastroduodenal intussusception caused by a leiomyoma in the gastric antrum, presenting with severe anemia. Open gastric wedge resection was performed as treatment, and complete diagnostic data were available, including computed tomography (CT) findings, gastroscopy, intraoperative photographs, and postoperative pathology.
Case presentation
Written informed consent was obtained from the patient for both treatment and publication of this case. All patient details have been de-identified, and the reporting of this study adheres to the CARE guidelines. 5
A 38-year-old woman weighing 62 kg (body mass index, 23.3 kg/m2) presented to the emergency department with a >10-day history of dizziness, palpitations, and fatigue accompanied by inappetence, black stools, and tenesmus. She denied weight loss in recent months. Three days earlier, gastroduodenoscopy at a local hospital had revealed gastric mucosal ischemia and spherical lesions in the duodenum. The patient had been otherwise well until the onset of symptoms and had no history of surgery. On arrival, she reported no abdominal pain, flatulence, or fever and was hemodynamically stable, with a temperature of 36.8°C, pulse of 88 beats/minute, blood pressure of 110/70 mmHg, respiration rate of 18 breaths/minute, and oxygen saturation of 100% on room air. Despite black stools, physical examination findings were notable only for anemia, while abdominal and digital rectal examinations were unremarkable. Laboratory studies revealed hypoalbuminemia, hypocalcemia, fecal occult blood, and microcytic hypochromic anemia (Table 1). She was admitted to the gastroenterology department for rehydration and blood transfusion to investigate the etiology further and underwent abdominal CT, which showed a heterogeneous, nonobstructing mass in the stomach extending into the second and third parts of the duodenum (Figure 1). Gastroscopy was repeated to assess the feasibility of endoscopic treatment and determine the tumor’s origin and nature, revealing a large polypoid mass originating from the anterior wall of the gastric antrum and protruding past the pylorus into the second part of the duodenum (Figure 2). The lesion’s surface was red but lacked mucosal ulcerations or stigmata of recent bleeding. Endoscopic reduction and tumor resection were deemed infeasible because of the lesion’s large size. Random biopsies showed mild acute and chronic inflammation with significant proliferation of blood vessels and fibroblasts. An exploratory laparotomy was performed under general anesthesia through a midline upper abdominal incision. During the procedure, the gastroduodenal intussusception was observed extending to the junction of the second and third parts of the duodenum and was gradually reduced with traction. An anterior gastrotomy revealed a 4.8- × 3.5- × 2.2-cm solid, well-defined, pedunculated intracavitary tumor near the greater curvature of the anterior wall of the gastric antrum. Wedge resection of the gastric tumor with a 2-cm margin was performed (Figure 3). The postoperative period was uneventful, and the patient was discharged on the ninth postoperative day. Histopathology and immunohistochemistry confirmed the diagnosis of gastric leiomyoma (Figure 4). During a 56-month follow-up, the patient remained well with no recurrence of gastric leiomyoma or gastroduodenal intussusception.
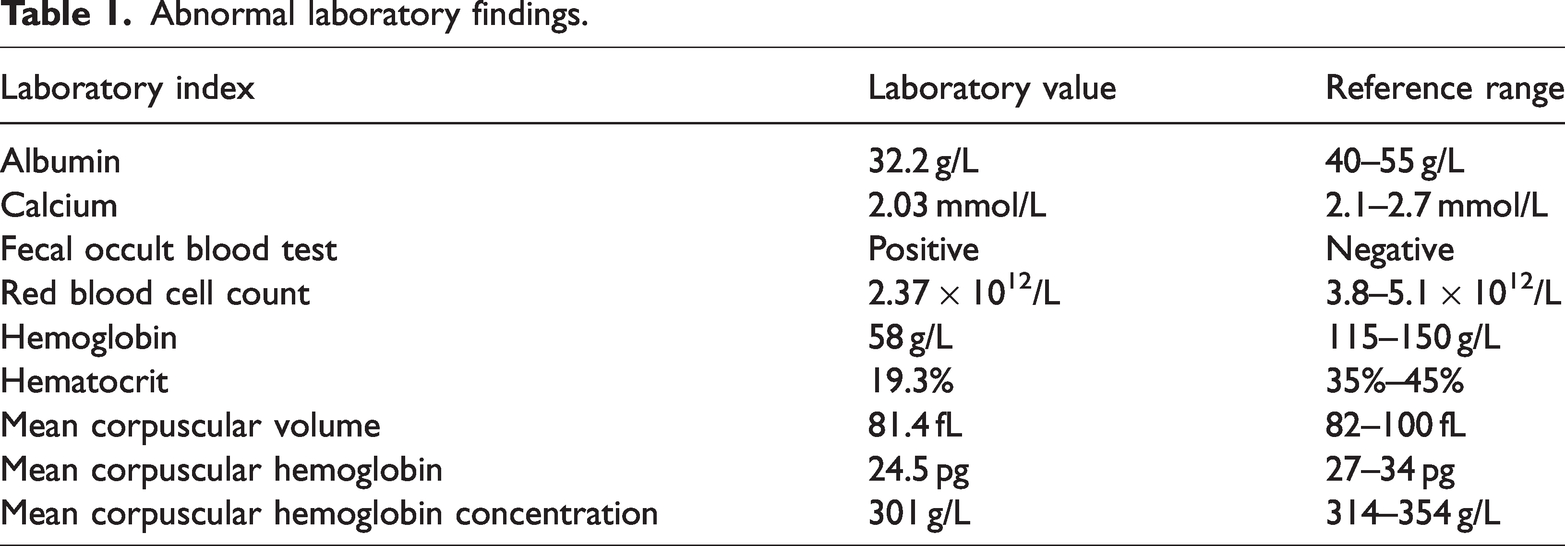
Abnormal laboratory findings.

Preoperative abdominal computed tomography images. (a) Axial scan showing a “target” soft tissue mass in the duodenum. (b) Coronal reformat illustrating the leading point of the intussusception extending to the junction of the second and third parts of the duodenum and (c) Sagittal reconstruction demonstrating intussusception of the gastric wall into the duodenum.
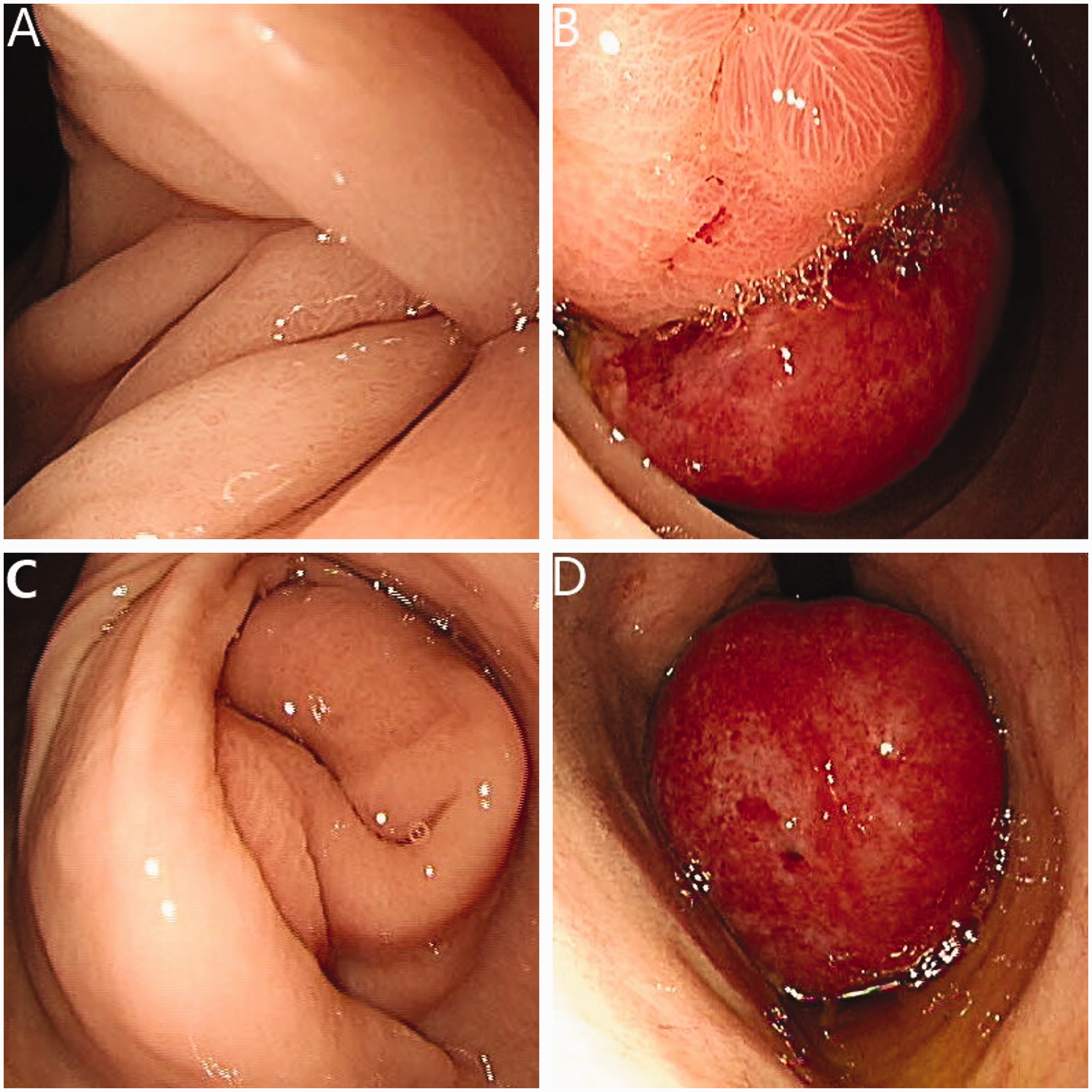
Endoscopic findings. (a) Image showing invagination of the gastric antrum into the duodenum. (b) The submucosal polypoid mass, along with the gastric wall, passing through the pylorus into the second part of the duodenum. (c) Image of endoscopic partial reduction of the antrum wall and (d) Retrograde distal view after endoscopic partial reduction.

Intraoperative findings and resection. (a) The gastric wall and palpable mass at the greater curvature of the gastric antrum invaginating through the pylorus into the duodenum. (b) Anterior gastrostomy exposing the mass for safe wedge resection and (c) Wedge resection of the tumor with secure margins.

Pathological findings. (a) Hematoxylin and eosin section showing a spindle cell neoplasm (×200) and (b) representative immunohistochemistry for CD117, CD34, DOG1, SMA, and desmin (×200).
Discussion
Gastroduodenal intussusception occurs when mobilized gastric mucosa or a tumor prolapses into the duodenum, pulling the adjacent gastric wall into a depression. It is an extremely rare condition, accounting for less than 10% of documented intussusceptions in adults.2,6 According to the literature, the lesions that cause gastroduodenal intussusception are typically mobile pedunculated submucosal tumors, such as lipomas, gastrointestinal stromal tumors, leiomyomas, Menetrier’s disease, polyps, and polypoid gastric adenocarcinomas.7–11 Additionally, gastroduodenal intussusception has been reported, though rarely, following bariatric surgery, particularly gastric plication. Increased gastric mobility due to division of the gastrosplenic and gastrocolic ligaments is suggested to be a prerequisite for this complication. 4 Although the leading point of the intussusception can arise from any part of the stomach, the incidence decreases from the antrum to the fundus. Gastric leiomyomas originate from smooth muscle cells, most commonly in the cardia and rarely in the antrum.12,13 This may explain the rare occurrence of gastric leiomyomas causing intussusception. The initial clinical manifestations of gastroduodenal intussusception vary depending on the degree of gastric outlet obstruction. Symptoms can range from chronic, intermittent signs such as epigastric fullness, mild abdominal pain, and melena to acute symptoms such as emesis, cramping abdominal pain, and hemorrhagic shock. 7 Differential diagnoses include rare conditions such as superior mesenteric artery syndrome in younger individuals and gallstone-induced Bouveret syndrome in older patients. 14 In our case, the patient did not exhibit symptoms of gastric outlet obstruction but presented solely with anemia-related manifestations, including dizziness, palpitations, and fatigue. Cases presenting only with anemia-related symptoms are limited in the medical literature, making this case relatively rare. 7 The most valuable preoperative diagnostic tools for gastroduodenal intussusception are esophagogastroduodenoscopy and abdominal CT. These modalities not only assess the degree of intussusception but also provide preliminary information about the lesion’s nature, offering significant guidance for treatment decisions.
The choice of therapeutic approach for gastroduodenal intussusception depends on the anatomical location, size, and nature of the lesion, as well as whether the intussusception is easily reducible. For small benign lesions, endoscopic reduction and resection is feasible. 15 By contrast, surgery is preferred for large lesions with undetermined preoperative benign or malignant characteristics, irreducible intussusceptions, or when endoscopic management is not viable. If the surgeon is experienced in minimally invasive techniques, laparoscopic resection is favored over open surgery. 9
Conclusion
Cases of gastroduodenal intussusception caused by gastric leiomyoma are rare. Clinicians should remain vigilant for gastroduodenal intussusception, particularly in young individuals presenting with signs of gastric outlet obstruction. The leading point of gastroduodenal intussusception is often a highly mobile pedunculated lesion in the stomach. Clinical manifestations vary depending on the degree of obstruction. Surgical methods should adhere to appropriate oncologic principles, with the location, size, and pathological characteristics of the underlying lesion serving as key evaluation criteria.
Footnotes
Author contributions
Benlei Zhu conceived the study, analyzed the data, and wrote the manuscript. Jingwei Fu selected the clinical case and supervised the study. Congming Wang analyzed the data and generated the figures. All authors read and approved the final manuscript.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Ethics statement
The present study was approved by the ethics committee of Jining No. 1 People’s Hospital (approval number: 2024-IIT-051) and conducted in accordance with local legislation and institutional requirements. Written informed consent was obtained from the patient for the publication of this case report.