
Abstract
Background:
When treating achalasia, balloon dilation is often combined with fluoroscopy to allow the lower esophageal sphincter to be visualized as it is being dilated. We sought to evaluate a new balloon dilation technology, EsoFLIP, which allows the shape of the balloon to be visualized in a nonradiographic manner by using impedance planimetry electrodes located within the dilation balloon.
Methods:
Two pigs weighing 35 kg were used. The EsoFLIP balloon dilator was introduced under endoscopic visualization. Successive injections of 50, 60, 70 and 85 mL into the dilation balloon permitted dilations at increasing diameters to be achieved. Following each dilation fluid was withdrawn to leave 30 mL in the balloon and an EsoFLIP image was captured to track progressive dilation of the gastroesophageal junction (GEJ).
Results:
The EsoFLIP catheter was safely deployed in the two pigs and no complications were noted. For pig 1, during dilation, the measured balloon diameter at the waist was 24.1, 28.9, 29.2 and 30.0 mm for balloon dilation volumes of 50, 60, 70 and 85 mL respectively. For pig 2 the corresponding diameter at the waist was 22.8, 27.1, 28.5 and 29.4 mm. The GEJ diameter increased from 12.5 and 12.4 mm to 17.4 and 17.5mm for pigs 1 and 2 respectively. Distensibility of the GEJ in pig 1 increased from 2.3 mm2/mmHg before to 4.4 mm2/mmHg after dilation and in pig 2 from 4.4 to 9.6 mm2/mmHg. The GEJ substantively achieved its final diameter after the dilation using just 50 mL in the balloon.
Conclusions:
We demonstrated technical feasibility and safety of the EsoFLIP dilator in a porcine model. Further studies in humans with achalasia remain to be conducted, which, besides demonstrating technical feasibility, should also evaluate the use of distensibility measurements taken during dilation to predict outcomes.
Introduction
Achalasia is a motility disorder of the esophagus in which the lower esophageal sphincter (LES) fails to relax resulting in functional obstruction of the esophagus. Current treatment of achalasia consists of balloon esophageal dilation or laparoscopic Heller myotomy [Boeckxstaens et al. 2011]. More recently a new endoluminal surgical technique, per oral endoscopic myotomy [Inoue et al. 2010], has been developed to treat the disorder.
EndoFLIP (Crospon Ltd, Galway, Ireland) [Kwiatek et al. 2010] is a new lumen imaging system which employs a balloon catheter containing an array of electrodes to allow dimension and distensibility measurements to be made in the esophagus and stomach. EndoFLIP has been used to assess the dimension and distensibility of the gastroesophageal junction (GEJ) after treatment by each of the three treatment techniques [Perretta et al. 2011a, 2011b; Rieder et al. 2012; de Ruigh et al. 2012a, 2012b; Rohof et al. 2012] and in particular has been shown to offer potential as a predictor of response to achalasia treatment [de Ruigh et al. 2012a, Rohof et al. 2012].
When performing esophageal balloon dilation, the balloon is expanded, using air or a radio-opaque liquid, to disrupt the esophageal muscle and widen the GEJ. This is typically done under endoscopic visualization. However, it is difficult to gauge the degree of dilation when looking axially along the balloon. Therefore, to better assess the degree of dilation, balloon dilation is often combined with fluoroscopy, whereby a radio-opaque fluid in the balloon, for example gastrograffin, will allow the shape of the balloon to be visualized, albeit that an actual GEJ diameter measurement cannot be easily determined. Of necessity, this exposes the patient to radiation. An added disadvantage of performing balloon dilation under fluoroscopic control is that if fluoroscopy is not available in the endoscopy suite, a simple dilation procedure may be held up.
To address the above, a new dilation catheter, EsoFLIP (Crospon), has been developed. This catheter is similar to the current EndoFLIP catheter with one major difference being that a standard high pressure dilation balloon is used on the shaft instead of a very compliant soft balloon. The latter is used when the requirement is simply to measure lumen size, and the balloon is inflated to a pressure of less than 0.1 bar. For achalasia dilation, the balloon must typically be inflated to 1.5 bar pressure, and therefore such catheters use much stiffer balloon materials.
The aim of this study was to evaluate the technical feasibility and safety of the EsoFLIP balloon dilation catheter in pigs.
Materials and methods
Two pigs weighing 35 kg were used. Permission for the study was obtained by the local animal committee.
EsoFLIP prototype dilation balloon
The initial EsoFLIP prototype dilation balloon has a diameter of 30 mm and a dilation length of 8 cm. The balloon is mounted on a 2.8 mm shaft, the tip of which can accommodate a 0.035 inch guidewire. Within the balloon are 16 measurement electrodes, spaced 5 mm apart, which permit simultaneous diameter measurements to be made over the dilation length.
Methods
An overtube was deployed, through which an endoscope was introduced. The location of the GEJ was noted and proximal and retroflexed images of the GEJ were captured. An EndoFLIP EF-325 balloon measurement catheter (Figure 1(a)) was deployed into the GEJ and the profile of the junction was measured with a balloon fill of 50 mL. The EF-325 catheter was then withdrawn and the EsoFLIP balloon dilator (Figure 1(b)) was introduced under endoscopic visualization without a guidewire. Successive injections of 50, 60, 70 and 85 mL into the dilation balloon, using the EndoFLIP fluid delivery system, permitted dilations at increasing diameters to be achieved. Following each dilation fluid was withdrawn to leave 30 mL in the balloon and an EsoFLIP image was captured to track progressive dilation of the GEJ. Upon completion of the dilation, the EsoFLIP catheter was deflated and withdrawn, and the endoscope was reintroduced to capture direct and retroflexed images of the GEJ post dilation. Finally, the EF-325 catheter was reintroduced across the GEJ and profiles of the GEJ were recorded with 50 mL in the balloon.

(a) EndoFLIP EF-325 catheter. (b) Prototype 30 mm EsoFLIP catheter.
Results
The EsoFLIP catheter safely deployed in the pigs under endoscopic visualization without the use of a guidewire. Between dilation steps, the position of the EsoFLIP catheter was regularly visualized, and if needed, adjusted to maintain the GEJ at the center of the balloon. This was done by reference to the real time image on the EndoFLIP system and endoscopically.
The minimum diameters and distensibility of the GEJ before and after the dilation, as measured by the EndoFLIP EF-325 catheter with 50 mL in the balloon, are shown in Table 1. Distensibility is defined as the minimum cross-sectional area of the GEJ divided by the pressure measured in the balloon. For pig 1, during dilation, the measured balloon diameter at the waist was 24.1, 28.9, 29.2 and 30.0 mm for balloon dilation volumes of 50, 60, 70 and 85 mL respectively. For pig 2, during dilation, the measured balloon diameter at the waist was 22.8, 27.1, 28.5 and 29.4 mm for balloon dilation volumes of 50, 60, 70 and 85 mL respectively.
Gastroesophageal junction (GEJ) diameter and distensibility before and after dilation.

Figure 2 shows an image of the GEJ of pig 2 before and after dilation, as measured with an EndoFLIP EF-325 with 50 mL in the balloon. On account of the wide GEJ opening, we have presented EndoFLIP images with a 50 mL balloon fill versus the 30 mL balloon fill more typically used for EndoFLIP imaging of the GEJ of patients with achalasia in previous studies. This was necessary since we were unable to achieve satisfactory images with 30 mL on account of the balloon not expanding adequately to conform with the shape of the large junction.

(a) EndoFLIP EF-325 image of the gastroesophageal junction (GEJ) of pig 2 before dilation. (b) EndoFLIP EF-325 image of the GEJ of pig 2 after dilation.
Figure 3 shows an image of the GEJ after dilation. There is relatively little disruption of the mucosal surface observed at the GEJ. Figure 4 shows the image of the EsoFLIP dilation balloon at each stage of dilation. Figure 5 shows an example of images of the GEJ of pig 2 at different stages of dilation, as measured by the EsoFLIP balloon with 30 mL in the balloon. It is evident that the GEJ has substantively achieved its final diameter after the dilation using 50 mL in the balloon.

Proximal view of the gastroesophageal junction in pig 2 after dilation.
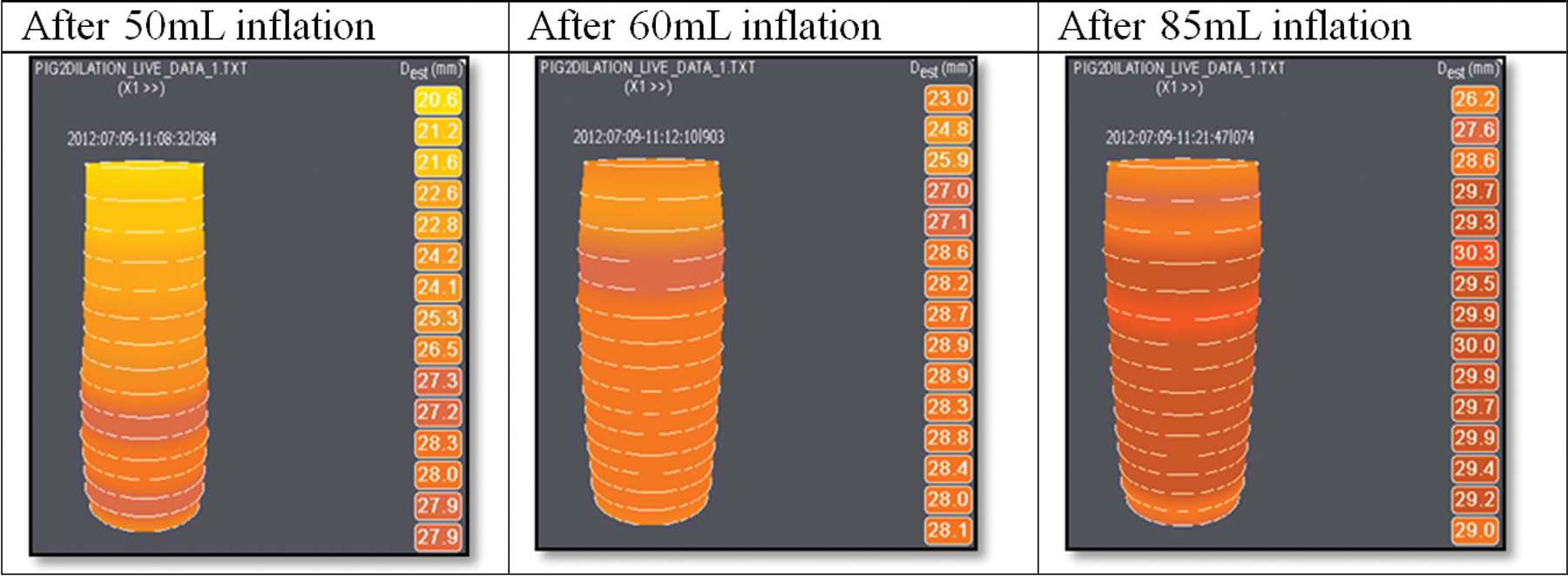
Sample images showing the EsoFLIP dilation balloon with different volumes of fluid during the dilation procedure.

Sample images of the gastroesophageal junction after different stages of dilation, with fluid withdrawn to leave 30 mL in the dilation balloon.
Discussion
We have demonstrated the technical feasibility of dilating the GEJ using a prototype EsoFLIP dilation catheter in a porcine model. This prototype 30 mm diameter dilation catheter provided an image with real time measurements of the GEJ both during and after dilation without the need for fluoroscopy.
When using conventional dilators under endoscopic visualization, a pressure is applied to the balloon to achieve a target diameter in accordance with a manufacturer-provided lookup table. However, the final diameter achieved is a function of the degree of recoil after the balloon is deflated. With the EsoFLIP dilation catheter, a target diameter can be selected and dilation can be stopped when the target diameter is achieved. When the balloon is deflated, the degree of recoil can be assessed, and successive dilations may be performed to achieve the final desired diameter. We noted that at the maximum balloon dilation diameter of 30 mm, the balloon pressure was approximately 1.5 atm. However, as can be seen in Figure 4, the majority of the diameter increase during dilation occurred at a significantly lower balloon volume. When dilation is carried out under endoscopic visualization alone, the balloon is inflated to a target pressure to achieve a target diameter. However, if fluoroscopy is employed, less pressure may be applied to the balloon, since balloon inflation will be stopped once full effacement of the dilator has been achieved, which may, in turn, potentially reduce the risk of perforation due to dilation. The ability to visualize the GEJ diameter during endoscopy may thus reduce the balloon pressures required, mirroring those obtained when fluoroscopy is used. As can be seen in Figure 3, the disruption of the mucosal surface was minimal despite achieving good dilation.
A weakness of the study is that the GEJ of the pig does not represent a good model for achalasia. The initial GEJ opening was significantly larger and the GEJ was more distensible than would be encountered in humans with achalasia. Nevertheless, it was possible to demonstrate a significant therapeutic effect with the GEJ being remodeled to produce a 40% diameter increase and a more than doubling of the junction distensibility (Table 1). Rohof and colleagues recently concluded that an EndoFLIP distensibility measurement may be used as an alternative to a timed barium esophagram to assess the effect of therapy of achalasia, the former offering the advantage of being able to be performed intraoperatively [Rohof et al. 2012]. They concluded that the sensitivity and specificity of GEJ distensibility for treatment failure is 92% and 72% respectively using a distensibility cutoff value of 2.9 mm2/mmHg and measured when inflating the EndoFLIP balloon to 50 mL. As can be seen from Table 1, the distensibility of the junctions after the two dilations was considerably above this distensibility threshold. The integration of EndoFLIP measurement with the dilation apparatus of EsoFLIP thus offers the possibility to potentially assess probable outcome after balloon dilation and may therefore offer guidance as to whether further dilations are required in additional dilation sessions.
In conclusion, we have demonstrated the initial technical feasibility and safe use of the EsoFLIP dilator in a porcine model. Further prospective studies in humans with achalasia remain to be conducted, which besides demonstrating technical feasibility, should also be designed to prospectively evaluate the ability of measurement-based clinical rules [Rohof et al. 2012], applied at the time of dilation, to predict outcomes.
Footnotes
Acknowledgements
The authors acknowledge the technical support for this study provided by Silvana Perretta MD, Department of Gastrointestinal and Endocrine Surgery, IRCAD-EITS, University of Strasbourg, Strasbourg, France.
Funding
This work was supported by Crospon Ltd, Galway, Ireland. J. O’Dea is an employee and stockholder of Crospon Ltd. P.D. Siersema has no financial relationships relevant to this publication to disclose.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.