
Abstract
We describe a case of congenital esophageal stenosis in which the patient underwent ineffective balloon dilatation twice and eventually required surgery. The case was initially misdiagnosed as achalasia. Pathological findings revealed tracheobronchial remnants (TBRs) in the muscular layer of strictured esophageal tissue. Most TBR strictures are located in the middle and lower thirds of the esophagus. Esophagography is the main examination method for esophageal stricture, and the appearance of the “rat tail sign” is a key diagnostic indicator. Endoscopic ultrasonography can reveal hypoechoic cartilaginous structures. The gold standards for TBR treatment include esophageal stricture resection, end-to-end esophageal anastomosis, and the construction of structures to prevent reflux. At present, endoscopic longitudinal resection and transverse anastomosis of the anterior esophageal wall with partial cartilage resection without pyloroplasty are novel and practical TBR procedures. To avoid further complications, patients with congenital esophageal stenosis should be promptly treated surgically if balloon dilatation is ineffective.
Keywords
Introduction
Congenital esophageal stenosis (CES) attributable to tracheobronchial remnants (TBRs) is a rare malformation, and diagnosing this condition can be difficult. TBRs are characterized by the abnormal presence of congenital tissue of tracheal origin in the esophageal wall, and these remnants are responsible for narrowing of the esophagus. 1 Surgical resection of esophageal stenosis with the tracheobronchial tissue is the only treatment that can completely correct the stenosis and its consequences. 2 This article reports a patient with TBRs who underwent surgery after failed esophageal dilatation. The presence of tracheobronchial tissue was confirmed using the surgically resected esophageal tissue.
Case report
The reporting of this study conforms to CARE guidelines. 3
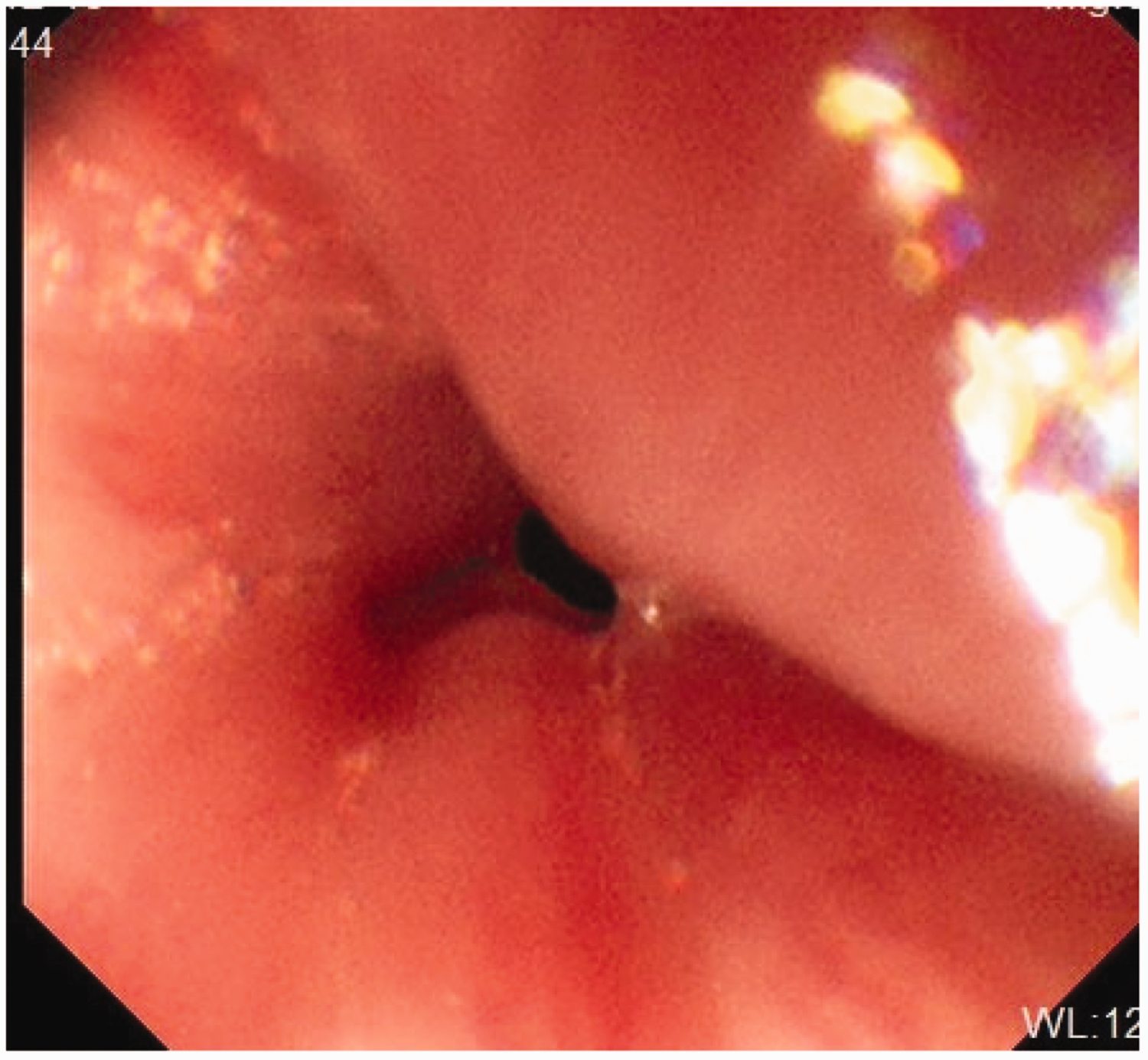
In November 2020, a 1-year-old girl was referred for recurrent vomiting and progressive dysphagia, which began at the age of 6 months when solid food feeding was started. The child regurgitated two to three times a day without projectile vomiting. The vomitus was gastric content that was free of bile and coffee-colored material, and vomiting was accompanied by hiccups and occasional choking while drinking milk. The child was hospitalized in People’s Hospital of Raoyang County (Hengshui, Hebei Province, China) and treated with antiemetic drugs, but vomiting persisted. The frequency of vomiting increased in the month before admission, eventually exceeding more than 10 times per day with belching. There was no coughing or choking when feeding and drinking. Esophagography revealed an abrupt narrow segment at the lower esophagus with marked proximal dilatation (Figure 1). The esophagoscopy findings included nonyielding lower esophageal stenosis without evidence of esophagitis (Figure 2). Clinical examination identified mild dehydration without malnutrition. On physical examination, the patient was conscious and responsive with slightly poor skin elasticity, and cyanosis on the face and perioral area and depression in the anterior fontanelle and eye socket were not observed. The results of most laboratory indicators, including the serum white blood cell count; red blood cell count; platelet count; hemoglobin, creatinine, cardiac enzyme, procalcitonin, C-reactive protein, immunoglobulin, alanine aminotransferase, and aspartate aminotransferase levels; erythrocyte sedimentation rate; and four coagulation indicators (activated partial thromboplastin time, prothrombin time, prothrombin time, thrombin time, fibrinogen), were within the normal ranges. Conversely, the carbon dioxide level (12.4 mmol/L) and anion gap (26.1) were suggestive of metabolic acidosis. The patient was treated with fluid replacement and acidosis correction. The patient was initially diagnosed with achalasia. Therefore, in December 2020, the patient was treated with balloon dilation at the hospital’s endoscopy center, and the stenosis was slightly dilated (Figure 3).
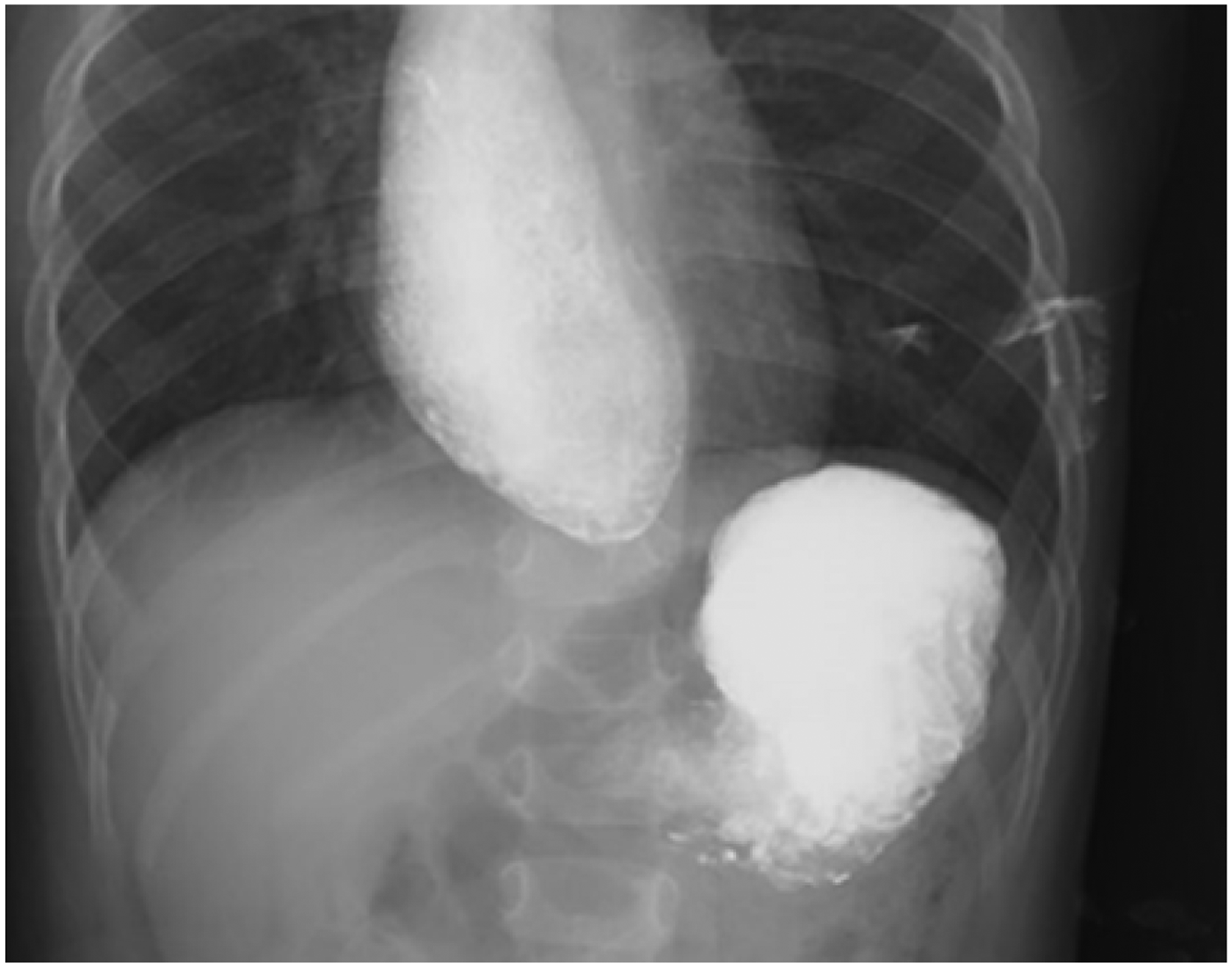
Esophagography revealed an abrupt narrow segment at the lower esophagus with marked proximal dilatation.

Stenosis was observed in the lower esophagus, and the endoscope (outer diameter, 5.8 mm) could not pass through the stenotic orifice, which was approximately 4 mm in diameter.
After balloon dilatation, the stenosis in the lower esophagus was dilated.
The patient’s condition was improved compared with that in the preoperative period, and she displayed good tolerance to drinking milk and eating a small amount of supplementary food without vomiting or abdominal distension. The treatment effect was considered satisfactory, and thus, she was discharged. However, 4 months later, her vomiting symptoms reappeared after eating solid food. In April 2021, the patient was readmitted for a second balloon dilation. The child tolerated the second balloon dilation with normal diet feeding, and symptoms such as vomiting and dysphagia were not present within 6 months of follow-up. In February 2022, during home observation at the age of 2 years, the patient was admitted for a third time because of vomiting after eating solid food, and her symptoms of vomiting and dysphagia gradually worsened. Esophagography revealed esophageal stenosis 2 to 3 cm above the cardia and tapered narrowing in the lower segment, similar to the “rat tail” sign (Figure 4). Finally, TBRs were suspected, and surgical exploration was performed on 19 February 2022. During the operation, esophageal stricture was found at the level of the diaphragm (approximately 0.8 cm long), and the upper esophageal lumen was normal. The demarcation between the muscle tissue and the mucosa of the stenotic esophageal segment was unclear, the mucosa was thin, and the mucosa was ruptured during separation. Hard material was present in the esophageal muscle layer, and a whitish cartilage-like material was observed after separation. Severed end-to-end anastomosis was performed after resection of the stenotic segment of the esophagus, followed by a Dor basal fold. The surgical specimen consisted of a 0.8-cm-long esophageal segment with a markedly narrowed lumen and a rigid wall. The postoperative pathological results revealed hypertrophy and disorders of the muscle layer within the examined tissue, and intermuscular tubules lined with ciliated columnar epithelium and surrounded by cartilage and mucus glands were present (Figure 5). The findings of immunohistochemical staining were as follows: CD34 (vascular+), S-100 (+), CR (−), and D2-40 (partial +).

Esophagography revealed a stricture (arrow) at the lower esophagus that was close to the gastroesophageal junction. The proximal portion of the lower esophagus was remarkably dilated.

Histological findings. (a) Squamous epithelium (black triangle) was present in the resected esophagus. Hypertrophic and disordered layers of muscle surrounded by mucous glands (thick arrow) and epithelial tissue were observed. Hematoxylin and eosin, original magnification ×40 and (b) The resected muscular layer contained chondrocytes (thin arrow). Hematoxylin and eosin original magnification ×100.
The subsequent clinical course was uneventful. In this patient, although anastomotic stenosis was found after surgery, she recovered after esophageal dilation was performed twice. The patient has remained asymptomatic after the second post-operative dilation, and she is eating normally. During 6 months of follow-up, no vomiting or dysphagia has been observed. The patient remains under follow-up.
Discussion
CES has been defined as intrinsic narrowing attributable to congenital malformations of the esophageal wall that is not necessarily symptomatic at birth. 4 The etiologies of CES are divided into three histologic entities: 5 (1) TBRs, (2) fibromuscular thickening (FM) or fibromuscular stenosis, and (3) membranous webbing or esophageal membrane. CES owing to TBR is a particularly rare condition. 6 Stenosis of the esophagus caused by a residual tracheobronchus was first reported by Frey and Duschel in 1936, who detected cartilage in the distal esophagus of a 19-year-old girl who had died of achalasia diagnosed from cardia. 7
TBRs are believed to result from the failed separation of the respiratory system from the foregut. 8 The tracheal outgrowth appears in the primitive foregut at the level of the fourth pair of pharyngeal pouches. After the longitudinal separation of the tracheo-esophageal foregut from the tail to the cranium, the trachea and esophagus become separate organs. One explanation is that the trachea extends from the common foregut as the lung buds grow, and another is that both the trachea and esophagus extend from the common foregut.9,10 The exact mechanism for the occurrence of this disorder has not been fully clarified. In addition, muscle hyperplasia and muscle disorders were also observed in our case. Some scholars11,12 believe that TBRs can be classified into the same category as bronchopulmonary foregut malformations. We speculate that some patients with TBRs have related muscle layer disorders. Singaram et al. 11 suggested that the reduction of myoenteric nitrogenous neurons might also be associated with TBRs.
In this case, because of the lack of awareness of TBRs, the patient was misdiagnosed with achalasia, and she underwent balloon dilation twice without benefit before a diagnosis of TBRs was given. The onset of TBR symptoms usually starts in infancy, generally after the introduction of semisolid or solid foods around 6 months of age. Regurgitation of food without gastric fluid and bile is the leading clinical manifestation. Zhao et al. 13 noted a time lag of 2 to 2.5 years between patient onset and final treatment, with final treatment occurring at an average of 2.6 to 3 years of age. In our case, the time from onset to final treatment was shorter than previously reported. However, our case featured a time lag of 14 months between the onset of symptoms and diagnosis of TBRs. The preoperative diagnosis of TBRs is extremely difficult. Early diagnostic differentiation is extremely important because of the need for definitive appropriate treatment. In terms of the location of onset, TBRs mainly arise in the lower third of the esophagus (within 1 cm of the gastroesophageal junction), EM affects the upper or middle third of the esophagus, and FM affects the middle or lower third of the esophagus. 2 Esophagography has been the main diagnostic tool, and the results in this study revealed a typical narrow stricture at the lower esophagus with proximal dilatation. Zhao et al. 13 divided TBRs into three types based on the findings of esophagography: type I, distal esophageal stenosis with either tapered or abrupt narrowing; type II, flask-shape shadow; and type III, type I or II together with the linear projection of barium at the level of stenosis. In our case, the presentation on esophagography was consistent with type I. Computed tomography might not always demonstrate the presence of the cartilage. 14 Esophagoscopy revealed dilation of the esophagus, and the folds of the esophageal mucosa gathered to form strictures. Esophagoscopy can identify reflux esophagitis. Recently, endoscopic ultrasonography has proven useful for the diagnosis of TBR by highlighting the presence of cartilage, 15 and the cartilage in the esophageal wall is visualized as a low or high echoic area.16–18 More than one radiological method is required because barium swallow can be misdiagnosed, and thus, additional tests should be performed if clinically suspected. 19
Whether CES is classified as TBRs is important for determining the therapeutic strategy. Unnecessary or overenthusiastic repetition of dilation can lead to deleterious complications. Fortunately, in our case, balloon dilation was only performed twice without complications. Wu et al. 12 suggested that surgical intervention should be considered if the first dilation failed to achieve expected results. For patients with TBRs, most scholars20–26 believe that resection of the esophageal stenotic segment followed by end-to-end anastomosis is the best treatment of choice.
It is extremely important to remember the possibility of a TBR diagnosis when first examining an infant with repeated vomiting. Every case suspicious of TBRs should be analyzed at a specialized center. The diagnosis of TBRs should be considered when an infant experiences repeated vomiting or dysphagia or features a failure to thrive. Unlike achalasia, balloon dilation is usually unsuccessful and dangerous in the treatment of TBRs. Our experience suggests that precise and complete resection of stenosis segment is a reliable treatment for TBRs.
Supplemental Material
sj-jpg-1-imr-10.1177_03000605221132704 - Supplemental material for Congenital esophageal stenosis caused by tracheobronchial remnants: a case report
Supplemental material, sj-jpg-1-imr-10.1177_03000605221132704 for Congenital esophageal stenosis caused by tracheobronchial remnants: a case report by Zhihong Gao, Lingyan Wang, Huaijun Liu and Xia Zhang in Journal of International Medical Research
Footnotes
Acknowledgements
This study was supported by the Second Hospital of Hebei Medical University and Hebei Children’s Hospital. We thank all of our colleagues in the Pediatric Surgery Department, Hebei Children’s Hospital.
Authors’ contributions
ZG and LW contributed to data collection and patient evaluation. LH revised the paper and provided practice consultation. XZ designed the study and drafted the paper. All authors read and approved the final manuscript.
Availability of data and materials
All data related to this case report are stored in the Pediatric Surgery and Radiology Department of Hebei Children’s Hospital, and data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that they have no conflict of interest.
Ethics statement
This study was approved by the Medical Research Ethics Review Committee of Hebei Children’s Hospital (approval number: 202225; approval date: 8 May 2022). Written consent was obtained from the patient’s parents throughout treatment and for the publication of this report.
Funding
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.