The aim of this study was to investigate the effects on pulmonary ventilation and oxygen uptake (O2) in athletes with a very high maximal oxygen uptake (O2max) and corresponding high ventilation capacity when using a modern metabolic system with relatively high resistance to breathing (HIGHRES), compared to a traditional system with low resistance to breathing (LOWRES). Four rowers and three cross-country skiers (without asthma), competing at a high international level, performed in experimental conditions with LOWRES and HIGHRES using a rowing ergometer and roller skis on a treadmill. The results showed that O2, blood lactate, heart rate and respiratory exchange ratio were not different between the LOWRES and HIGHRES test conditions during both submaximal and maximal exercise. Also, the athlete’s time to exhaustion (treadmill) and mean power (rowing ergometer) from maximal tests were no different between the two conditions. However, ventilation and expiratory O2 and CO2 concentrations were different for both submaximal and maximal exercise. Thus, the authors have concluded that the differences in resistance to breathing of metabolic systems influence elite endurance athletes E at low to very high workloads, thus affecting the expired gas fractions, but not the submaximal O2, O2max and performance in a laboratory setting at sea level.
Indirect calorimetry is a method that determines whole body metabolic rate via the measurement of pulmonary gas exchange.1 The golden standard for indirect calorimetry is still considered to be the Douglas Bag method, which involves collecting exhaled air in sealed bags, followed by an analysis of the content in terms of volume and gas fractions.2,3 Since the 1960s, automated metabolic systems that aim to facilitate practical measurements and the presentation of data in real time have been introduced to the commercial market. These systems are based on mixing chamber, breath-by-breath or hybrid methodology (through micro-sampling into a miniature mixing chamber) and are available both as stationary systems for the laboratory and portable systems for measurements in the field.1,4–7 Custom-designed portable Douglas bag systems have also been built for measurements in the field.8–10
Automated metabolic systems are commonly used to investigate athletes’ maximal oxygen uptake during sport-specific performance in various exercise activities. However, only a few studies have validated these systems using highly skilled endurance athletes with pulmonary ventilation corresponding to nearly 200 L/min during maximal exercise.5,6,11 Furthermore, because highly trained athletes may ventilate more than 200 L/min during maximal exercise,12 the resulting increased resistance may further limit the accuracy of some systems.11 The capacity for this kind of extreme breathing is likely a challenge for many breath-by-breath systems and even for systems with mixing bag technology. In these cases with very high ventilation, another factor that should be considered is the resistance to breathing (RES) that is attributable to the metabolic system’s hardware. Effects on pulmonary ventilation would be expected due to increased airway resistance caused by the dimensions of the hoses, breathing valves, flow meters and mixing chambers.13
To minimize RES when using a Douglas Bag system, it has been recommended that the hose should be 30 mm or greater in internal diameter (ID), but without stating the hose’s maximum length.14 Saltin and Astrand15 noted that in a Douglas Bag system with a hose ID of 35 mm and length of 0.5 m, the pressure difference (Δp) measured between the ambient air and inside of the system hardware was 1, 3, 6 and 10 cmH2O (98, 294, 588 and 981 Pa) at air flow rates of 100, 200, 300 and 400 L/min, respectively. Gore16 recommended that Δp should be less than 6 cmH2O at flows up to 300 L/min and hoses should be greater than 30 mm in ID and no longer than 1.5 m on either the inspiratory or expiratory side. However, the standard lengths of hoses delivered with common metabolic systems (Jaeger Oxycon Pro, Carefusion Germany 234 GmbH, Hoechberg, Germany; Moxus Modular Metabolic System, AEI Technologies Inc., Pittsburgh, USA; and AMIS 2001, Innovision A/S, Odense, Denmark) are often 1.7–2.7 m (Hans Rudolph Inc., Shawne, USA and Flexible ducting U62, Senior Aerospace BWT, Adlington, UK).
A recent study13 investigated the RES in three commonly used automated metabolic systems and the results showed that the RES was much higher than in previous recommendations. Significant differences were found between the systems and their individual breathing valves, hoses, flow meters and mixing chambers that were included as parts. Interestingly, the lowest resistance was found with a custom-made Douglas Bag system, which had about half the resistance of the automatic metabolic systems. Another interesting observation is that Δp for two of the tested breathing valves was found to be higher than in the information on the manufacturer’s website (Hans Rudolph Inc.).
However, a difference in Δp can be expected, depending on the circumstances in which it is measured. For instance, manufacturers usually measure the Δp in their two-way non-rebreathing valves during a static (constant) one-direction flow, while human pulmonary ventilation entails a dynamic intermittent flow. In the study by Ainegren et al.,13 the Δp was measured in the breathing valve mouthpiece adapter and the inspiratory and expiratory flow were obtained by a metabolic simulator. The metabolic simulator provides a dynamic intermittent flow, similar to human breathing, allowing for more relevant conditions when measuring Δp compared to a constant flow condition. The alternating flow between the breathing valve’s inspiratory and expiratory ports must pass both in and out through the mouthpiece and adapter; in practice, this is a prolongation of the upper airways and, together with the valve volume, there is an increase in anatomical dead space, which accelerates the flow back and forth through the mouthpiece and valve. This intermittent flow produces twice the mean flow rate (during the flow) and a much higher peak flow than in a constant flow. The accelerations and higher flow rates lead to more turbulence and a higher overall mean Δp than for a constant flow at the same ventilation: both manufacturers and researchers present an exponential increase in Δp for a linear increase in flow rate. Furthermore, the opening-closing procedure of the breathing valve’s inspiratory and expiratory ports may also result in different Δp compared to when they are continuously open to a flow. The air density also varies; therefore, Δp may not be normalized against a standard pressure. However, the extent of a likely difference in Δp due to different measurement circumstances is so far unknown.
The oxygen cost of the respiratory muscles’ work of breathing and the effects of different RES have been studied using a proportional assist ventilator and installing obstacles that increase RES in the hardware that distributes the air flow.17–22 The results show that the oxygen cost for the work of breathing constitutes a significant part of measured whole body (10%–15%) and the large differences in RES have a great influence on physiological and performance measures: for example, submaximal exercise follows a change in RES, while ventilation changes in the opposite direction. During maximal exercise, ventilation is still changed, as is the subject’s performance level, while any effect on seems more unclear.
The significance of RES for various types of face masks has also been studied by manipulating the inspiratory and/or expiratory resistance in the parts used for distribution of the air flow.23–27 The results showed both unchanged and increased and heart rate (HR) and unchanged or decreased ventilation on submaximal exercise due to increased RES. For maximal exercise tests, decreased and performance level were found in those studies where this was measured, while ventilation and HR were either decreased or unchanged due to increased RES. However, these studies had other purposes than to study the effects of the RES of commercial metabolic systems and the subjects were mostly untrained or poorly endurance trained with a low .
In a recently published paper,28 the physiological effects of different RES in two types of two-way non-rebreathing valves were studied using endurance-trained and recreationally active subjects of both genders. The Δp of the complete metabolic systems hardware was unfortunately unknown, while the difference in pressure between the two tested valves was known by the information given by the manufacturers. This study found significantly higher submaximal and energy expenditure for all tested groups with the use of the valve with higher RES, while HR and rated perceived exertion (RPE) remained unchanged. Also, submaximal ventilation was higher for the endurance-trained groups, but not for the recreational groups. Furthermore, on an incremental maximal test, peak oxygen uptake, ventilation, HR and RPE were similar, while time to exhaustion (TTE) was significantly shorter with the use of the valve with higher RES. The reason for the higher submaximal and ventilation and shorter TTE was ascribed to an increase in breathing work and reduced blood flow to the locomotor muscles. However, the subjects’ respiratory exchange ratio (RER) only reached ∼1.00 on the maximal test, a level that is far below the adopted end criterion for a maximal aerobic performance, which means that the validity of the measuring equipment and experiments can be questioned.
To gain knowledge of the energy cost needed for breathing through the hardware of metabolic systems, estimations can be done in the same way as for a fan or a pump that drives a fluid through a pipe system, using equation (1)
where PREQ is the required power (W), Δp is the pressure (Pa) difference measured between the ambient air and the inside of the system hardware, is the volumetric air flow rate (m3/s) and η is the mechanical efficiency, which in this case is the ratio of the obtained power to the athlete’s metabolic rate (a unit analysis for the equation gives: ). The metabolic rate can be calculated from the caloric equivalent (CE), which is based on the RER and is well known for a given (CE: 4.686–5.047 kcal/L of at RER 0.707–1.00), and converted to power (e.g. 1 W = 0.01433 kcal/min). Applying the PREQ equation in the study by Kim et al.,28 using the difference in Δp between the two valves (1.8 cmH2O, 176.5 Pa), a mean of the inspiratory and expiratory volumetric flow in the valve of 0.0067 m3/s (ventilation 200 L/min), a η of 20% and a CE of 5 kcal/L of , gives a PREQ of 5.9 W, 0.08 kcal/min and a of 0.02 L/min. Furthermore, calculating the PREQ from the study on RES in hardware for automated metabolic systems,13 using the same mean flow in the breathing valve as above and a mean Δp of 856.5 Pa (inspiratory and expiratory Δp of 913 and 800 Pa), which was measured for a complete system hardware (Moxus Modular Metabolic System, AEI Technologies Inc.) supplied with the same type of two-way non-rebreathing valve (2700, Hans Rudolph Inc.) as one of the valves used in Kim et al.,28 gives a PREQ of 28.6 W, 0.4 kcal/min and a of 0.08 L/min.
Thus, even if the RES in the hardware of modern automated metabolic systems has been found to be higher than earlier systems and recommendations, it seems unlikely that there are any significant effects on oxygen cost and energy expenditure due to RES in the hardware of present-day automatic metabolic systems. However, with the increased use of automated metabolic systems, instead of Douglas Bag systems with much lower RES,13 and longer hoses for the distribution of inhaled and exhaled air to the measurement system’s sensors, experiments investigating the influence of RES on elite athletes’ ventilation and aerobic energy expenditure have an increasingly greater relevance.
Against this background, the aim of this study was to investigate the effects of a relatively higher RES, typical of some modern metabolic systems on pulmonary ventilation and oxygen uptake in athletes with a very high and correspondingly high ventilation capacity. Based on the present calculations of energy cost needed for breathing through the hardware, the present hypothesis is that the measurement of oxygen uptake is not affected by the RES previously found in modern stationary metabolic systems.
Methods
Measurements of breathing resistance
The resistance to breathing was calculated as the ratio of delta (driving) pressure to the rate of air flow as shown in equation (2)
where RES (Pa/L/s) is the resistance to breathing, Δp (Pa) is the pressure difference measured between the ambient air and the inside of the metabolic systems hardware and (L/s) is the air flow rate.
The Δp was measured (−2500 to 2500 Pa, GMSD25 MR, Swedish Thermo Instrument AB, Täby) at a rate of 100 Hz and filtered at 8 Hz using a Butterworth-filter in Microsoft Excel. For both inspiratory and expiratory flows, the Δp in the systems’ hardware should be greatest near the subject’s mouth. Thus, the Δp was measured in the adapter between the mouthpiece and the breathing valve by replacing the regular adapter with a custom-made adapter manufactured from ABS plastic, using additive manufacturing (Mid Sweden University). The custom-made adapter’s geometry was equivalent to the manufacturer’s original adapter, but supplemented with connections for measuring negative and positive Δp during and , respectively. Since the measured Δp is negative compared to the ambient air during inspiration and positive during expiration, a negative sign is reported before the values for the inspiratory RES (RESI). Furthermore, the RESI and expiratory RES (RESE) were calculated from flows at ambient (ATPS) and body (BTPS) temperature, pressure and water vapour saturation conditions, respectively.
Setup for metabolic measurements
Two different hardware setups were used to achieve experimental conditions with low RES (LOWRES) and high RES (HIGHRES). For the LOWRES, a Douglas Bag system described in an earlier paper13 was used. This system was found to have approximately half the RES of three investigated automated metabolic systems and only one third of the RES of the automated system with the highest RES. This LOWRES hardware setup included the same type of breathing valve and hose as an automated metabolic system (AMIS 2001, Innovision A/S) and a custom-built three-way valve (Håkan Eriksson, Karolinska University Hospital, Stockholm, Sweden) to distribute the expired air, either to the ambient surroundings or for collection to bags (130 L, PU coated fabric, C. Fritze Consulting, Svedala, Sweden). The HIGHRES experiments were carried out using components (and resistance) added to the Douglas Bag system described above. The standard setup was supplemented with the same type of hose on the inspiratory side and a valve mounted on the outer end of the hose. This extra valve was a two-way T-shape breathing valve (2700, Hans Rudolph Inc.) with the opening plugged where the mouth piece is mounted in normal use, which made it a one-way valve with the air flow able to pass straight through the inlet and outlet of the valve. The same type of modified breathing valve was also mounted on the expiratory side between the hose and the inlet to the three-way valve.
In order to acquire knowledge of the resistance in the LOWRES and HIGHRES setups prior to experiments with athletes, a study was carried out using a metabolic simulator (Metabolic Simulator No 17056, Vacumed, Ventura, CA, USA) with the ability to select standardized by mimicking different tidal volumes (VT) and breathing frequencies (fB).13 A VT of 3 L and fB of 15, 30, 45, 60 and 75 VT/min to give the mean of 45–225 L/min, with the corresponding mean and (during flow) of 1.5, 3.0, 4.5, 6.0 and 7.5 L/s, was created using the simulator. Five adjacent curves of Δp and formed the results, which showed that within the range of tested air flows, LOWRES was −46.1 + 7.3 and 53.2 + 12.9 Pa/L/s, while HIGHRES was −155.6 + 13.4 and 154.7 + 15.7 Pa/L/s, for the inspiratory and expiratory sides, respectively. Hence, this result shows a large difference in resistance between LOWRES and HIGHRES experimental conditions, with the HIGHRES similar to that reported for automated metabolic systems.13 Consequently, it was stated that this experimental setup should provide a valid and representative range of RES to study the influence of resistance to breathing.
The validity of the mechanical lung simulator was also checked using both LOWRES and HIGHRES setups and the same as mentioned above. After sampling a number of 43 VT (129 L) into a 130-L Douglas Bag, it was emptied in a water-sealed spirometer (custom made and enlarged copies of a Collins-Tissot). This showed that the volume from the mechanical lung simulator was like the volume determined in the spirometer: 128.1 + 1.5 L (p > 0.05), coefficient of variation = 1.14%. The laboratory air pressure (p), temperature (T), relative humidity (RH) and density (ρ) were 983 hPa, 22.5 °C, 38% and 1.16 kg/m3 during the measurements with the mechanical lung simulator.
The Douglas Bag’s content of expired gas fractions was measured using O2 and CO2 gas analyzers (Skiers: AEI Technologies Inc.; Rowers: Vacumed Gold Edition, and AMIS sport, Innovision A/S), while the bag’s gas volume (BTPS) was measured in the spirometer, which was equipped with a temperature sensor for calculations of STPD gas volume. The gas analyzers were calibrated with the following O2 and CO2 concentrations: AEI Technologies Inc., 16% ± 0.02 rel.% and 4% ± 1%; Vacumed, 15% ± 0.04% and 6% ± 0.1%; AMIS, 15% ± 0.02 rel.% and 5% ± 0.1 rel.%.
Subjects and exercise protocol
A total of seven endurance-trained athletes, including four rowers and three cross-country skiers (age, 26.3 ± 6.3 years; body height, 1.91 ± 0.04 m; body weight, 91.6 ± 9.7 kg), who compete at a high international level volunteered to take part in the study. The study was approved by the Regional Ethical Review Board, reg no. 2016-418-32M. Before the experiments started, the subjects signed their voluntary approval to participate in the study. The subjects reported no known asthmatic problems.
All subjects participated in both experimental conditions, where three of the subjects started with LOWRES and four started with the HIGHRES setup. A rowing ergometer (Concept 2 Inc, Morrisville, USA) was used for the rowers’ experiments while the skiers roller skied on a treadmill (Rodby Innovation AB, Vänge, Sweden) using the classical style diagonal stride technique. The time between the two experimental conditions was 4.5 h for the rowers and 1–2 days for the skiers.
Before the data collection began, there was a 10-min warm-up period on the initial submaximal workload. The exercise protocol included three submaximal workloads (Sub 1, Sub 2 and Sub 3, corresponding to 57 ± 6, 66 ± 4 and 75 ± 3% of ) for 4 min each, with a 1-min break between them, followed by a 10-min break before a maximal test (Max) was performed. The rowing ergometer power (P) of the three submaximal workloads was predetermined at 230, 260 and 290 W, while the maximal test was a 6-min all-out test, where the mean P was registered. The skiers performed the three submaximal workloads on treadmill inclinations and speeds of 4° at 2.5 m/s, 5° at 2.64 m/s and 6° at 2.78 m/s. Max was a ramp test with constant speed (3.06 m/s) and an increase in treadmill inclination by 1° every minute, starting at 3°, until voluntary exhaustion. If the skier performed more than 8 min (completed 10° inclination), the speed was increased by 0.14 m/s every minute until exhaustion. The skier’s TTE was also registered from the maximal tests. The roller skis’ (Swix Classic Roadline C2, Lillehammer, Norway) rolling resistance coefficient (µR) was carefully investigated in another study, conducted during the same period, using special equipment for this purpose.29 This study showed that µR did not change during the period the experiments were carried out (µR = 0.025).
Data collection and analysis
The data collection took place at low altitude (<300 m above sea level) at three different laboratories. The skiers performed tests at Mid Sweden University, Östersund, Sweden30 and the rowers performed tests at the laboratory at Swedish Sports Confederation, Bosön, Sweden or the Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark. The laboratories’p, T, RH and ρ were 990 ± 26 hPa, 18.8 ± 1.0 °C, 45% ± 12% and 1.18 ± 0.03 kg/m3 during the experiments with the athletes.
HR (Polar Electro OY, Esbo, Finland) and Δp were recorded during the last minute of each submaximal workload, while a Douglas Bag was filled with expired air. During the maximal test, HR, Δp and Douglas Bags were sampled throughout the test (filling time per bag 30–40 s). Directly after each submaximal workload and the maximal test, the subjects rated their perceived exertion in breathing (RPEB 6–20) and a capillary blood sample was taken from a fingertip to analyse blood lactate (La) (Biosen S-line Lab+, EKF-Diagnostic, Cardiff, UK).
The results of HR, , fB, , ventilatory equivalent , RER, RESI and RESE were calculated as mean and standard deviation (SD) from the last minute for each submaximal workload. From the maximal test, the results were calculated from 30 s of sampling and from the same time during the test as when the highest was obtained. The subjects’fB was determined by counting the number of Δp curves and the VT from the ratio of /fB. The and were calculated at current ATPS and BTPS conditions, respectively, while the and were calculated according to STPD conditions.
Due to the volume of CO2 produced not being the same as the O2 consumed, except when RER is 1.00, and are not exactly the same.31 Since the Douglas Bag method measures the athlete’s only, to calculate RESI, was calculated using equation (3), which is known as the Haldane transformation
where is the fraction (%) of nitrogen in inspired air and is the fraction of nitrogen in expired air computed from the measured gas fractions of expired oxygen and carbon dioxide as shown in equation (4)
Furthermore, the and flow rates (L/s) are also dependent on the relative time (%) between inspiration and expiration, which was calculated for each flow direction (tI and tE) by the number of samples for each flow (SI and SE, respectively) divided by the total sum of samples as shown in equation (5)
Statistics
The statistical analyses were performed in SPSS for Windows statistical software release 24.0 (SPSS Inc., Chicago, IL, USA). Statistical differences (p < 0.05) between LOWRES and HIGHRES test conditions were evaluated for HR, La, RER, RPEB, (L/s), (L/min and L/s), , VT, fB, , , RESI, RESE, TTE and P, using the paired t-test. On Sub 1 for LOWRES, the Δp curve for one of the subjects was unfortunately not satisfactorily registered. Thus, the results for RESI and RESE on Sub 1 are reported for six subjects only.
Results
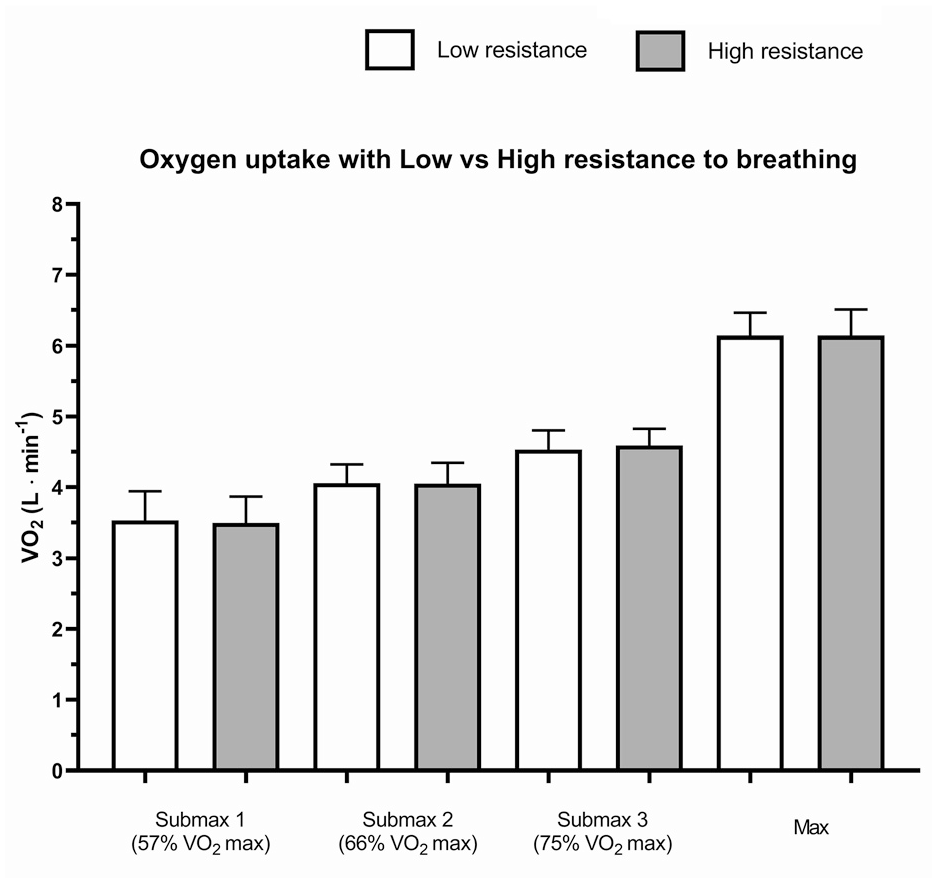
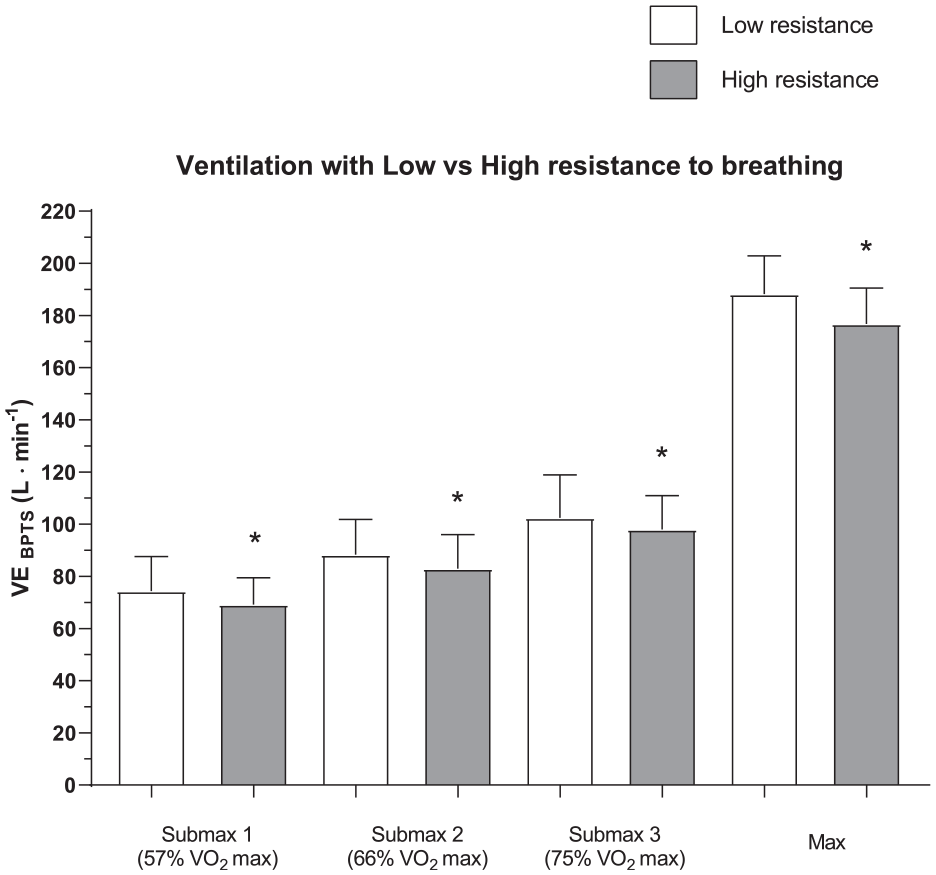
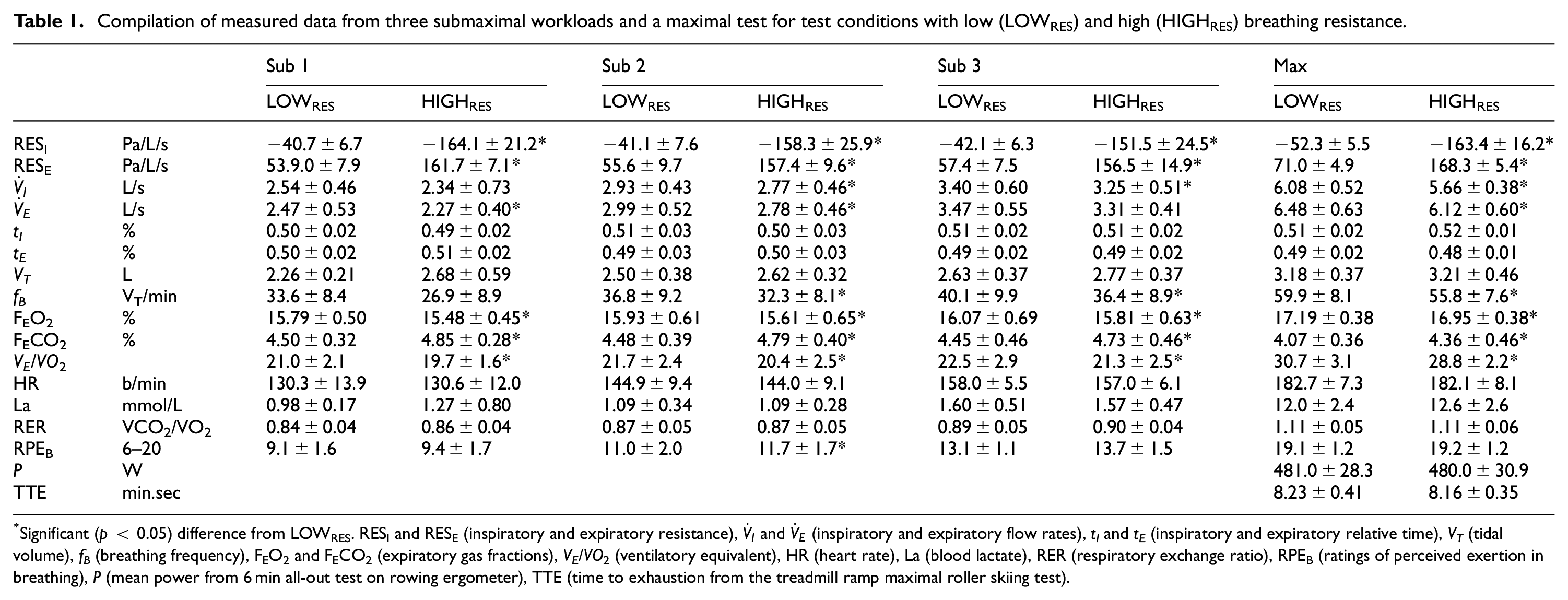
No significant (p > 0.05) difference was found in between the LOWRES and HIGHRES experimental conditions either at Sub 1, Sub 2, Sub 3 or Max (see Figure 1). On the contrary, (L/min) was significantly lower (<0.05) for the HIGHRES test conditions at all workloads (see Figure 2). The lower for HIGHRES was due to a lower fB, while VT was unchanged for all workloads, except the lowest (see Table 1). Also, due to the lower pulmonary ventilation per minute, the , and (L/s) were significantly lower using HIGHRES. Furthermore, the FEO2 and FECO2 were significantly different for all workloads, with lower FEO2 and higher FECO2 for the HIGHRES experiments. Significant differences were also found for both RESI and RESE between the LOWRES and HIGHRES experiments for all workloads (see Table 1). However, no differences were found between conditions with regard to La, HR, RER, tI, tE, TTE, P and RPEB, except for RPEB on Sub 1 (see Table 1).
Oxygen uptake with low (LOWRES) and high (HIGHRES) breathing resistance at submaximal and maximal exercise.
Ventilation with low (LOWRES) and high (HIGHRES) breathing resistance at submaximal and maximal exercise.
Compilation of measured data from three submaximal workloads and a maximal test for test conditions with low (LOWRES) and high (HIGHRES) breathing resistance.
Significant (p < 0.05) difference from LOWRES. RESI and RESE (inspiratory and expiratory resistance), and (inspiratory and expiratory flow rates), tI and tE (inspiratory and expiratory relative time), VT (tidal volume), fB (breathing frequency), FEO2 and FECO2 (expiratory gas fractions), VE/VO2 (ventilatory equivalent), HR (heart rate), La (blood lactate), RER (respiratory exchange ratio), RPEB (ratings of perceived exertion in breathing), P (mean power from 6 min all-out test on rowing ergometer), TTE (time to exhaustion from the treadmill ramp maximal roller skiing test).
Discussion
To the best of the authors’ knowledge, this is the first study to evaluate the influence of different RES in metabolic systems on pulmonary ventilation and oxygen uptake in elite athletes with very high aerobic power.
The authors hypothesized that in athletes with a very high aerobic power and ventilation capacity, the high resistance against breathing, which has previously been estimated in modern stationary metabolic systems, would not affect the measurement of when compared to the minor breathing resistance that exists in the traditional Douglas Bag method. Results showed that the measured variables , La, HR and RER were unchanged between the LOWRES and HIGHRES experimental conditions during both submaximal and maximal exercise. Also, there were no differences in TTE and P between the two test conditions. However, breathing frequency and pulmonary ventilation were affected during both submaximal and maximal exercise.
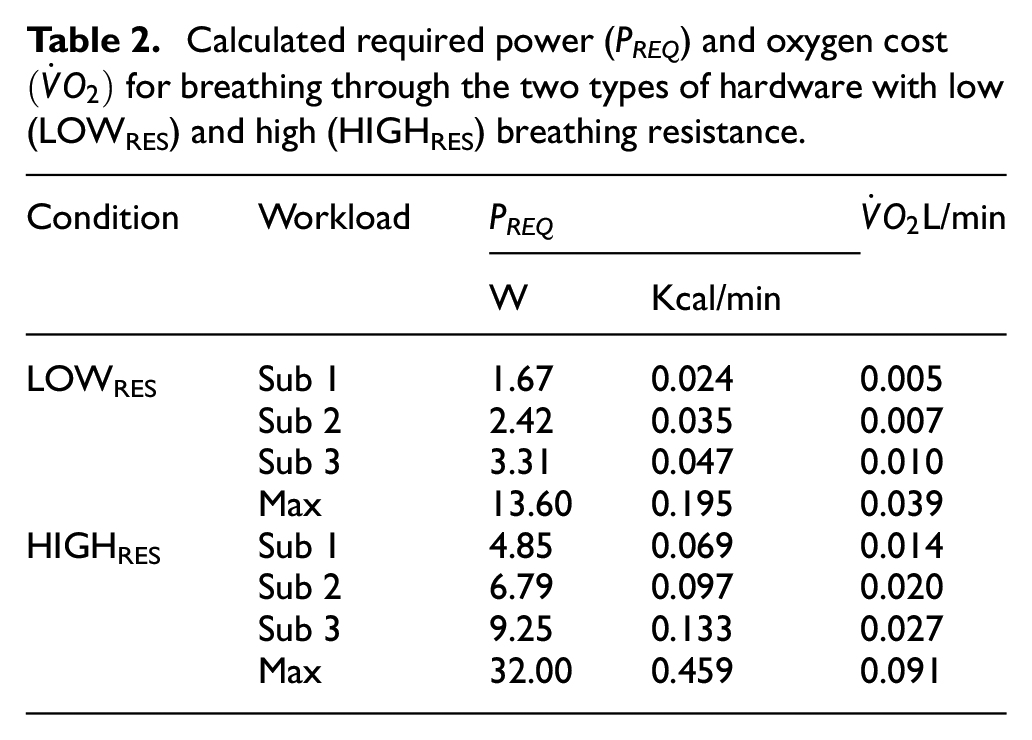
Calculations of the PREQ and oxygen cost, based on the measured Δp and volumetric flow of the seven subjects for the LOWRES and HIGHRES testing conditions, are presented in Table 2. Mechanical efficiency (η = 17.9% ± 0.7%) was established from the three submaximal workloads using the ratio of the power of the rowing machine and the rower’s metabolic rate calculated from their RER, CE and . The calculated result assumes that the gas flow is not compressed: the relatively small Δp between the inside of the hardware and the ambient air (0.2%–2%) shows that the air is likely to be minimally compressed. Furthermore, mechanical efficiency can vary by a few percent between individuals, different types of sports and activity levels and may also be different for the respiratory muscles in comparison to the muscles used for locomotion. However, these possible causes of error are not likely to dramatically change the calculated results of PREQ and oxygen cost.
Calculated required power (PREQ) and oxygen cost for breathing through the two types of hardware with low (LOWRES) and high (HIGHRES) breathing resistance.
Condition
Workload
PREQ
L/min
W
Kcal/min
LOWRES
Sub 1
1.67
0.024
0.005
Sub 2
2.42
0.035
0.007
Sub 3
3.31
0.047
0.010
Max
13.60
0.195
0.039
HIGHRES
Sub 1
4.85
0.069
0.014
Sub 2
6.79
0.097
0.020
Sub 3
9.25
0.133
0.027
Max
32.00
0.459
0.091
As can be seen in Table 2, the PREQ and oxygen cost is very small. Even at maximal exercise at the HIGHRES test condition, the calculated cost for breathing through the hardware is less than 1.5% of the measured energy expenditure and oxygen uptake. This should be less than any day-to-day variation measured with metabolic systems, including the Douglas Bag method. Even though the difference in hardware resistance between LOWRES and HIGHRES is both large, valid and representative for today’s metabolic systems, the calculated energy cost appears to be too small and therefore would not be expected to have a significant influence on the results of . Thus, it is not surprising that the actual measurements of the athletes’ were not significantly different between the LOWRES and HIGHRES conditions.
As a comparison, Wetter et al.20 calculated the oxygen cost for the respiratory muscles’ work of breathing using an equation by Aaron et al.17 at 0.18, 0.30 and 0.61 L/min for exercises of 50%, 75% and , and the oxygen cost of a large difference in RES (<10 cmH2O/L/s (981 Pa/L/s)) to 0.11, 0.20 and 0.54 L/min, which was verified in their experiments on 50% and 75% of . However, this study used a proportional-assist ventilator to reduce work on the inspiratory muscles during unloading and added mesh screens during loading with many times larger RES than in this study.
Nevertheless, the difference in RES between the two experimental conditions clearly affected the athletes’ pulmonary ventilation, even at relatively low flow rates. Increasing the RES from low to a high RES similar to that of hardware used by manufacturers of automated metabolic systems significantly reduced the by 5.9% ± 1.1% (see Figure 2). The reduction was due to decreased fB, while the VT was unchanged, although there was a trend to a larger VT for the HIGHRES test condition. Thus, it might be that a possible increase in submaximal oxygen and energy consumption and a decrease in TTE and P, due to increased RES, was cancelled out due to the decreased fB and , resulting in similar work of breathing and . However, the difference in RES and was not perceived by the athletes, which is shown by similar ratings of perceived exertion for breathing between the two test conditions.
Despite the very high (5.8–6.8 L/min) for the athletes taking part in this study, the ventilation at (<206 L/min) was not as high as that reported in some other studies.12 The tests were carried out on low land (less than 300 m above sea level), even though the air density was lower than at standard sea level conditions. With an even lower air density, the ventilation and can be expected to be higher than in this study. Even though the viscosity and friction against the hardware inner surfaces will be a little lower with decreased density, resistance to breathing in the hardware of a metabolic system being used at high altitude should be addressed.
There were also differences in the measured FEO2 and FECO2 between the LOWRES and HIGHRES test conditions, where the former decreased and the latter increased in the HIGHRES test condition. This is well in line with the decrease in breathing frequency and pulmonary ventilation found for HIGHRES. When the breathing frequency changes, the duration for each breath in the lungs also changes. Thus, with an increased duration, the time for the diffusion of gases to proceed between the pulmonary capillaries and alveoli is extended. This should be the reason why a greater difference occurred for HIGHRES between the inspiratory and expiratory gas fractions for O2 and CO2. A changed VT also entails changed expired gas fractions, since the gas volumes in the lower respiratory tract are changed proportionally to a changed VT (while anatomical dead space remains relatively constant). However, the athlete’s VT was not different between the two experimental conditions.
One important concern of this finding is that researchers and manufacturers should be aware that breathing resistance differences between an automated metabolic system and the reference method being used to validate the system can imply changes in that are somehow compensated for by changes in FEO2 and FECO2, resulting in the same , as shown by Jensen et al.7 In addition, during progressive submaximal work, and are often used to determine the so-called ventilatory thresholds. These provisions could thus depend on whether a system with high or low RES is used. Prior to the study’s implementation, the option of using a representative automated metabolic system for the HIGHRES setup was discussed, but this option was rejected due to possible validity problems with the comparative flow measurements. If an automated system had been used for the HIGHRES, speculation would have arisen at this stage about whether the established difference in ventilation was due to a validity problem with the automated system flow sensor or the difference in breathing resistance.
The was lower for HIGHRES due to the lower pulmonary ventilation and similar oxygen uptake compared to LOWRES. The increased from Sub 1 to Max from 21.0 to 30.7 and 19.7 to 28.8 for LOWRES and HIGHRES, respectively. Increasing the and thereby the oxygen cost of breathing when hyperventilating is significant.17 Forsberg and Saltin32 and Dempsey and colleagues33,34 discuss how a reduction in the oxygen saturation of the arterial blood (SaO2) that occurs in highly trained athletes might be a cost benefit between lowering the energy demands needed for the increased hyperventilation at the expense of a small reduction in SaO2. In this study, the for the submaximal workloads was within the lower range of the critical level (20–25) indicated by Saltin and above this level for the maximal tests, but lower than that seen in some other studies for maximal exercise (30–40).35,36 Another aspect contributing to lowering would be that increases less proportional (M0.55) with body weight (M) than max (M0.73), which would limit maximal ventilation more in relatively heavy athletes (as in this case).12 However, the and oxygen partial pressure gradient between the alveoli and pulmonary capillaries were all apparently still sufficient to cause an effective gas exchange and similar oxygen carrying capacity in the blood, which is indicated by the changes in FEO2 and FECO2 that are discussed above and similar metabolic and performance measures for the test with high breathing resistance in comparison to the test with low resistance.
The results of , , and TTE in this study exhibit both similarities and deviations from the results of other studies investigating the influence of breathing resistance (see section ‘Introduction’). The reason for this may consist of several factors, such as the participant’s different ventilation, aerobic and performance capacity, protocols, equipment and of course the differences in RES of the hardware being studied. In many of the other studies, the RES was much higher than in this study and large differences in inspiratory versus expiratory RES were also common.
The results of this study should be most useful for researchers, clinicians and test leaders who work with studies of healthy endurance-trained athletes who are active at a very high performance level. Also, both users and manufacturers should consider resistance differences between systems in the validation processes, which may result in differences in , but not necessarily in . Even though the athletes’ performances and oxygen uptake were unaffected by the difference in RES in the hardware being used, the authors recommend being vigilant with metabolic systems with a high RES. A conscious choice of hardware and its components can make a great difference to RES. Also, if extremely long hoses are necessary, for example, for tests on a very large treadmill, there should be consideration about using a Douglas Bag system with very low RES instead of an automated system with higher RES due to the system sensors and mixing chambers.
Conclusion
The results of this study show that the differences in RES of metabolic systems influence elite endurance athletes’ at low to very high workloads and this affects the expired gas fractions, but not the submaximal , and performance in a laboratory setting at sea level.
Footnotes
Acknowledgements
Many thanks go to Glenn Björklund, Tobias Elgh and Thomas Lindberg (the Swedish Sports Confederation, Bosön, Sweden) for great assistance with the physiological measurements carried out on the rowers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD
Mats Ainegren
References
1.
ShephardRJAoyagiY. Measurement of human energy expenditure, with particular reference to field studies: an historical perspective. Eur J Appl Physiol2012; 112: 2785–2815.
2.
DouglasCG. A method for determining the total respiratory exchange in man. J Physiol1911; 42: 17–18.
3.
ShephardRJ. Open-circuit respirometry: a brief historical review of the use of Douglas bags and chemical analyzers. Eur J Appl Physiol2017; 117: 381–387.
4.
MacfarlaneDJWongP. Validity, reliability and stability of the portable Cortex Metamax 3B gas analysis system. Eur J Appl Physiol2012; 112: 2539–2547.
5.
RosdahlHGullstrandLSalier-ErikssonJ, et al. Evaluation of the Oxycon Mobile metabolic system against the Douglas bag method. Eur J Appl Physiol2010; 109: 159–171.
6.
RosdahlHLindbergTEdinF, et al. The Moxus Modular metabolic system evaluated with two sensors for ventilation against the Douglas bag method. Eur J Appl Physiol2013; 113: 1353–1367.
7.
JensenKJörgensenSJohansenL. A metabolic cart for measurement of oxygen uptake during human exercise using inspiratory flow rate. Eur J Appl Physiol2002; 87: 202–206.
8.
AnderssonFSkoglundPViktorssonJ, et al. A portable Douglas bag system. In: LinnamoVLindingerSSmithG (eds) 3rd international congress on science and Nordic skiing (ICSNS) 2015. Vuokatti: University of Jyväskyla University of Salzburg, 2015, p.59.
9.
de GrootGSchreursWAvan Ingen SchenauGJ. A portable lightweight Douglas Bag instrument for use during various types of exercise. Int J Sports Med1983; 4: 132–134.
BeltramiFGFroydCMamenA, et al. The validity of the Moxus Modular metabolic system during incremental exercise tests: impacts on detection of small changes in oxygen consumption. Eur J Appl Physiol2014; 114: 941–950.
12.
JensenKJohansenLSecherNH. Influence of body mass on maximal oxygen uptake: effect of sample size. Eur J Appl Physiol2001; 84: 201–205.
13.
AinegrenMJensenKRosdahlH. Breathing resistance in automated metabolic systems is high in comparison with the Douglas Bag method and previous recommendations. J Sports Eng Tech. Epub ahead of print 30 June 2017. DOI: 10.1177/1754337117715946.
14.
ÅstrandPORodahlK. Textbook of work physiology. 3rd ed.New York: McGraw-Hill, 1986, pp.299–304.
GoreCJ (ed.). Determination of maximal oxygen consumption. 2nd ed.Champaign, IL: Human Kinetics, 2013.
17.
AaronEASeowKCJohnsonBD, et al. Oxygen cost of exercise hyperpnea: implications for performance. J Appl Physiol1992; 72: 1818–1825.
18.
BabcockMAPegelowDFHarmsCA, et al. Effects of respiratory muscle unloading on exercise-induced diaphragm fatigue. J Appl Physiol2002; 93: 201–206.
19.
RomerLMLoveringATHaverkampHC, et al. Effect of inspiratory muscle work on peripheral fatigue of locomotor muscles in healthy humans. J Physiol2006; 571: 425–439.
20.
WetterTJHarmsCANelsonWB, et al. Influence of respiratory muscle work on VO2 and leg blood flow during submaximal exercise. J Appl Physiol1999; 87: 643–651.
21.
HarmsCAWetterTJMcClaranSR, et al. Effects of respiratory muscle work on cardiac output and its distribution during maximal exercise. J Appl Physiol1998; 85: 609–618.
22.
HarmsCAWetterTJSt CroixCM, et al. Effects of respiratory muscle work on exercise performance. J Appl Physiol2000; 89: 131–138.
23.
CarettiDMWhitleyJA. Exercise performance during inspiratory resistance breathing under exhaustive constant load work. Ergonomics1998; 41: 501–511.
24.
CerretelliPSikandRSFarhiLE. Effect of increased airway resistance on ventilation and gas exchange during exercise. J Appl Physiol1969; 27: 597–600.
25.
DressendorferRHWadeCEBernauerEM. Combined effects of breathing resistance and hyperoxia on aerobic work tolerance. J Appl Physiol Respir Environ Exerc Physiol1977; 42: 444–448.
26.
HeusRden HartogEAKistemakerLJA, et al. Influence of inspiratory resistance on performance during graded exercise tests on a cycle ergometer. Appl Ergon2004; 35: 583–590.
27.
HermansenLVokacZLereimP. Respiratory and circulatory response to added air flow resistance during exercise. Ergonomics1972; 15: 15–24.
28.
KimSHomesteadEPByrnesWC. Breathing valve resistance alters physiological responses during a graded exercise test. Eur J Appl Physiol2018; 118: 1921–1929.
29.
AinegrenMCarlssonPTinnstenM. A portable rolling resistance measurement system. In: SubicAFussPCliftonP, et al. (eds) The impact of technology on sport V. Hong Kong: Elsevier, 2013, pp.79–83.
30.
AinegrenMTuplinSCarlssonP, et al. Design and development of a climatic wind tunnel for physiological sports experimentation. Proc IMechE, Part P: J Sports Engineering and Technology. Epub ahead of print 4 October 2018. DOI: 10.1177/1754337118801729.
31.
McArdleWDKatchFIKatchVL. Exercise physiology: energy, nutrition, and human performance. 7th ed.Philadelphia, PA: Lippincott Williams & Wilkins, 2010.
32.
ForsbergASaltinB. Konditionsträning i teori och praktik. In: Forsberg A and Saltin B (eds) Aerob arbetsförmåga syrets väg till och förbrukning I Arbetande muskulatur. Idrottens Forskningsråd. Sveriges Riksidrottsförbund. Uddevalla: Bohuslänningens Boktryckeri AB, 1988, pp.22–37.
33.
DempseyJHansonPPegelowD, et al. Limitations to exercise capacity and endurance: pulmonary system. Can J Appl Sport Sci1982; 7: 4–13.
34.
DempseyJA. J.B. Wolffe memorial lecture. Is the lung built for exercise?Med Sci Sports Exerc1986; 18: 143–155.
35.
EkblomBBerglundB. Effect of erythropoietin administration on mammal aerobic power. Scandinav J Med Sci Sports1991; 1: 88–93.
36.
TannerDADukeJWStagerJM. Ventilatory patterns differ between maximal running and cycling. Respirat Physiol Neurobiol2014; 191: 9–16.