
Abstract
The purpose of this study was to investigate the resistance to breathing (RES) in heat and moisture exchanging devices (HME) intended for use during physical activity in the cold. RES was investigated for seventeen HMEs, including different types of filters. In addition, the influence of headwind on RES was tested using four representative HMEs. HMEs were mounted to the face of an artificial head manufactured from ABS plastic. The HMEs were connected to a mechanical lung simulator, which delivered standardised inspiratory and expiratory air flow rates (
Introduction
It is time to intensify preventive measures against the high prevalence of airway morbidity among winter endurance athletes. A pronounced increase in the prevalence of asthma among cross-country skiers was detected in the 1990s. 1 More than two decades later, the situation is unchanged 2 and asthma among winter endurance athletes typically arises during early adolescence. 3 The aetiology is believed to be repeated and prolonged exposure to cold and dry air. 4
During exposure to cold air, thermal mapping of the airways has, as expected, shown that the temperature of inhaled air increases as air moves towards the periphery of the lungs with heat transferred from the airway walls. 5 The temperature at each location in the lung decreases with decreasing ambient air temperature, as well as with increased ventilation. 5 Because cold air holds less water vapour, greater rates of evaporation are necessary during inhalation in cold climates, which leads to greater water loss from the airway mucosa. 6 Since the evaporation process requires energy (enthalpy of vaporisation), this is taken from the heat in the airways, which counteracts the heating to some extent. Upon exhalation, some of the moisture and heat will be returned to the upper airway surfaces as a result of condensation, due to a gradually decreasing temperature and transfer of heat from the lower respiratory tract. However, most of the water vapour and heat is exhaled and the process as a whole causes dehydration and cooling of the airways.
A simple device that could protect the airways from potentially harmful effects of heavy exertion in the cold is the heat and moisture exchanger (HME). 7 The principle of an HME is that its inner surfaces and filters are heated and moistened by exhaled air. The filter also provides a barrier that prevents the mixing of residual exhaled air with ambient air, thus stopping the volume and surface inside the HME from being cooled and dehumidified with ambient air during the short time between exhalation and inhalation. As a result, upon inhalation, cold and dry ambient air will be heated and moistened by the filter and the remaining exhaled volume inside the HME. Differences in HME filter area, mesh density, and remaining expiratory volume should lead to differences in the ability to warm and humidify inhaled air. Some degree of heat impact from the friction between gas molecules and the filter is conceivable, but the impact from this source of heat is likely to be relatively small. The intended functionality of HMEs is thus to provide a pre-station where cold and dry ambient air is partially warmed and humidified before it reaches the airways.
Use of an HME has been shown to attenuate exercise-induced bronchoconstriction during physical activity in cold air among patients with asthma8–11 and even among healthy athletes. 12 In addition to prevention of bronchoconstriction, HME usage may reduce osmotic stress on the airways that could lead to bronchial hyperreactivity. 7
Winter endurance athletes, such as cross-country skiers, are rarely seen using HME during competition, even though it is not banned. Reasons for not using HME may include inconvenience, increased dead space, breathing resistance (RES), and work of breathing (WOB). HME volume has the potential to cause both positive and negative impacts on the user. The impact of increased dead space on inhaled air temperature and humidity causes a decrease in pulmonary O2 and an increase in CO2 concentrations.
It has been suggested that even small increases in dead space could affect minute ventilation at higher exercise intensities. For example, comparisons between mouthpiece plus nose clip versus facemask breathing apparatus, as commonly used in cardiopulmonary exercise testing, have indicated that facemasks, which generally introduce slightly higher dead space volumes (∼50 ml), have minimal effect on respiratory variables, and no effects on exercise economy and test performance.13–15 Marginal differences in dead space aside, the HME filter also has potential to increase RES and thereby WOB compared to a no-HME condition. The effects of different RES on WOB have been studied by using a proportional assist ventilator and installing obstacles that increase RES in the hardware that distributes the air flow.16–21 The results showed that the respiratory muscles’ oxygen cost (
Increased dead space, RES and WOB, combined with other factors, such as comfort and convenience, have the potential to cause concerns among athletes that an HME may negatively affect their performance. Thus, HMEs must present minimal additional dead space, RES and WOB if they are to be adopted by athletes for use during high-intensity training sessions and races.
Consequently, the main aim of the present study was to measure and compare RES in the HMEs available on the Nordic market. Secondary aims were to evaluate whether RES is influenced by different ventilatory rates in harsh wind conditions. Quantification of HME volume and RES enabled calculation of the effect of increased dead space on pulmonary gas concentrations, as well as the oxygen and energy cost to drive airflow through the HME and its filter.
Methods
Heat and moisture exchangers
A total of 17 HMEs, including different types of filters and one neck/face tube, from five manufacturers (Airtrim, Vapro, Produktutveckling AB, Västerås, Sweden; Jonaset, Suomen Jonas Oy, Helsinki, Finland; CT Mask, AirGuard Medical Products Co., USA; Lungplus, Lungplus Info AB, Hörby, Sweden; Craft Sportswear, Borås, Sweden) were tested for RES. The HME model names, abbreviations, weight, filter cross-sectional area and volume (dead space) are presented in Table 1. The volumes are approximate and depend on the individual geometry of the human face. The different models and filters are also illustrated in Figure 1.
Characteristics of the heat and moisture exchangers tested in the study.
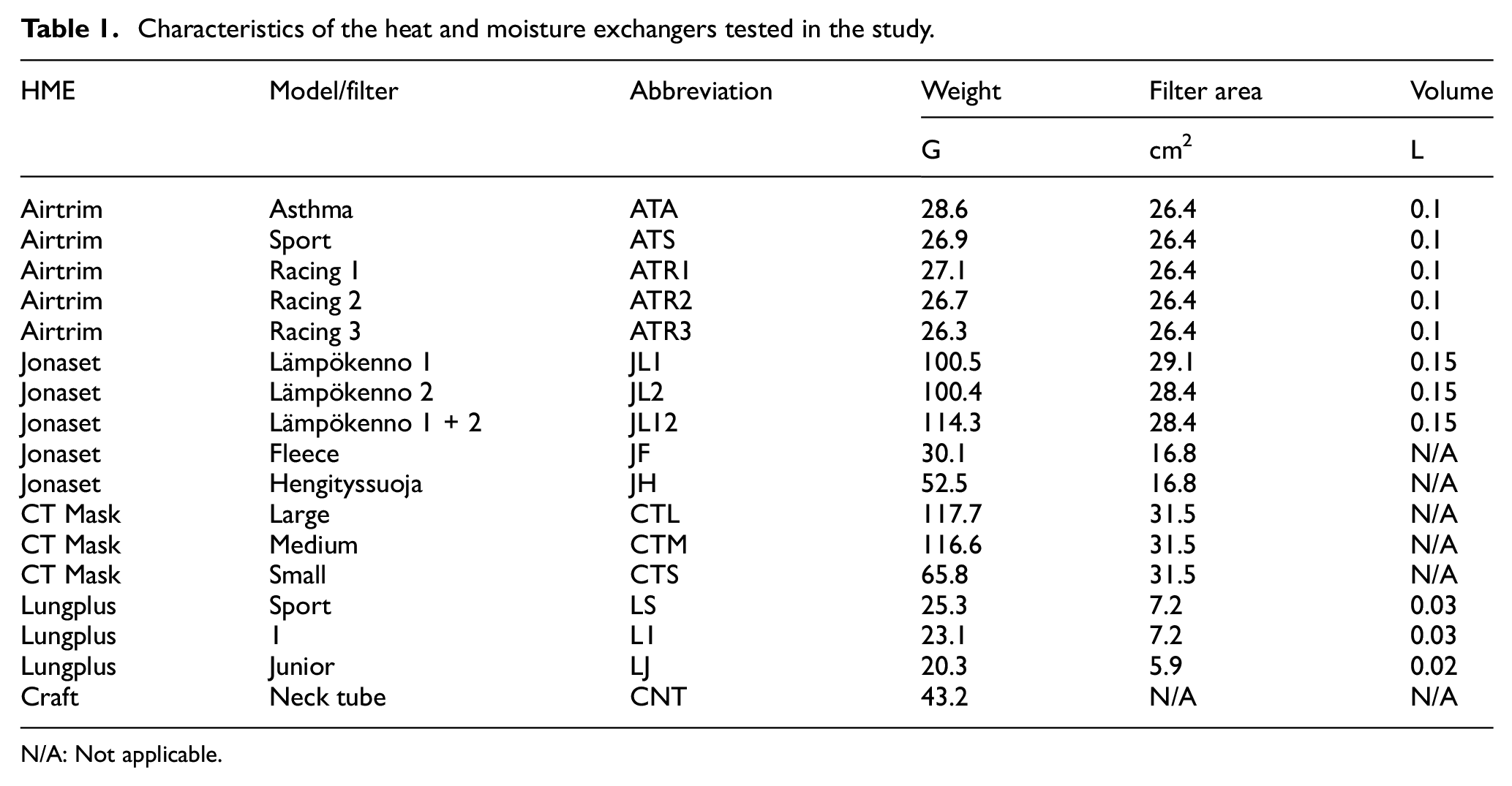
N/A: Not applicable.
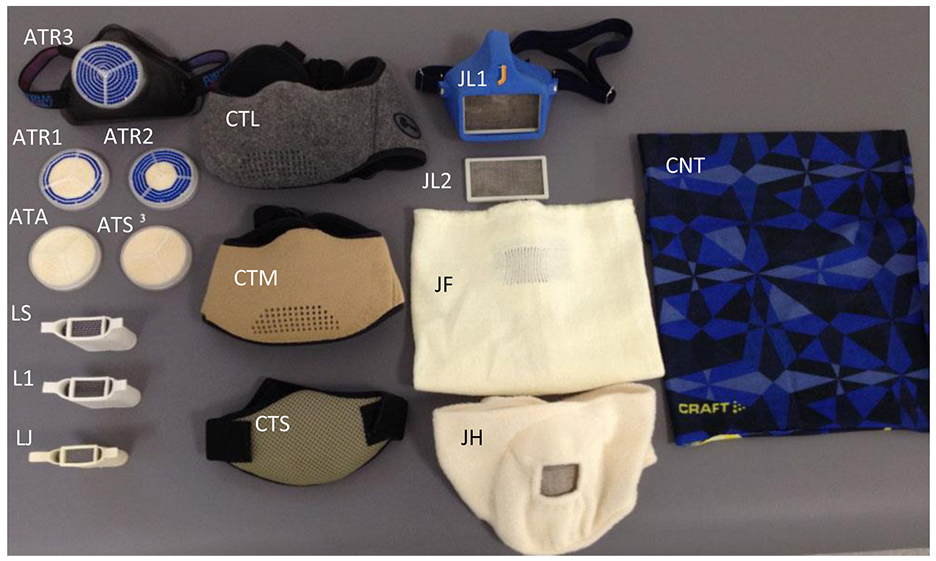
The heat and moisture exchangers with different filters tested for resistance to breathing: Airtrim with five different filters – ATA, ATS, ATR1, ATR2, ATR3; Lungplus in three different variants – LS, L1, LJ; CT Mask in three different sizes – CTL, CTM, CTS; Jonaset with two different filters – JL1, JL2, and two face tubes with filters – JF, JH; Craft, a neck/face tube without any filter – CNT (Table 1).
All HMEs enclose the nose, mouth and adjacent skin surfaces, except the models from Lungplus, which are held firmly in the mouth. The CNT is large enough to cover the face and neck and is marketed to protect surfaces from the cold, rather than an HME for the airways. However, since skiers sometimes cover the mouth and nose with these types of tubes, they were considered relevant to compare with true HMEs.
The five filters belonging to the Airtrim HME have straight channels through which the inhaled and exhaled air will pass, but the size and number of channels vary. The channels are surrounded by thin walls of paper-like material which pass through the filter between its inside and outside. Two of the Airtrim filters (ATA, ATS) design can be seen in Supplemental Appendix B, Figure 4. Lungplus, CT Mask, and Jonaset have filters consisting of a mesh of metal wires through which the air flow will pass. The JL can be used with filter 1 and 2 separately or together: the study tested all three variants. The CT Masks, JH and JF have the filter integrated in a textile that cover large areas of the face and parts of the filter area. The CT Masks have smaller holes in the textile, allowing the air to pass through more easily. However, the holes on the inside are placed a few centimeters higher up, which means that in addition to the navigation around the network of metal wires, the flow must also pass diagonally through the filter to reach the holes on the corresponding side. The filters in the different CT Masks are of the same type, while the masks appear to consist of partly different textiles. Because the flow needs to pass through the filter as well as the textiles, RES needed to be examined in all three variants due to textile differences. The CNT contains no filter, hence the air flow solely passes between the fibers of the relatively thin textile (100% polyester).
Resistance to breathing
Pulmonary ventilation (

To provide selected standardized
The head of a normal-sized human (body height and weight, 170 cm and 78 kg, respectively) was photographed with a 3D camera and manufactured from ABS plastic, using additive manufacturing (Sports Tech Research Centre, Mid Sweden University). The head had a cross sectional area of 336.5 cm2. For connection between the oral cavity and the mechanical simulator, a simple plastic tube with inner diameter of 35 mm was used (Figure 2). The head was designed with an open mouth with a cross-sectional area between the lips of ∼8 cm2. To provide a softer face surface, more similar to human tissue, and avoid leakage to the HME’s surface, a foam sheet was glued to the face. Also, to further prevent leakage, HMEs were taped to the face surface. For HMEs inserted in the mouth (Lungplus), a special adapter was mounted that held the HME between the lips.

Experimental setup of measurements of resistance to breathing: the mechanical lung simulator, a head made from ABS plastic with mounted foam sheet on the face and one type of heat and moisture exchanger tested in the study.
A small connection was inserted under the chin to the front of the oral cavity in order to measure the pressure difference (Δp) between the dynamic air flow inside the HMEs and the ambient static air pressure. Measurements of Δp (−2500 to 2500 Pa, GMSD25 MR, Swedish Thermo Instrument AB, Täby) were made at a rate of 100 Hz. In order to filter out spikes, raw data was filtered at 20 Hz using a Butterworth-filter in Microsoft Excel. Different frequencies were tested to develop a median curve well adapted to raw data. The RES in the HMEs was calculated by the ratio between Δp (Pa) and

Flows were generated using VT of 1, 2 and 3 L and fB of 30, 45 and 60 VT/min to provide the mean
Five additional curves of Δp and
Since sports, such as cross-country skiing, are practiced while moving at different speeds, a dynamic pressure should arise from the air molecules on the HME filter. Thus, in order to study the effect of headwind on RES, measurements were made in a climatic wind tunnel 31 at wind speeds of 0.0, 2.8, 8.3 and 13.9 m/s using four representative HMEs, one from each manufacturer, except Airguard Medical, including ATS, JL1, LS and CNT. The type of filter selected was based on a pilot survey of students at a Swedish high school with national intake towards cross-country skiing, where 17 of 22 students used the ATS, three used the ATR2, one used the ATA and one used the LS. Because the headwind caused turbulence, thus producing more variable flow curves, the results of RESI, RESE and overall mean of RES (RESM) in this part of the study were based on ten flow curves.
The laboratory air pressure, temperature, relative humidity, and density were 955 hPa, 15.6°C, 20%, and 1.15 kg/m3, respectively, during the testing.
Estimations of energy cost needed for breathing through the HMEs were performed as described in Ainegren et al. 28 using equation (3):

where PREQ is the required power (watts),
The effect of HME-induced dead space on pulmonary gas concentrations was calculated using equations (4) and (5) in Supplemental Appendix A and the results presented in Table 5.
Finally, two HME filters of paper-like material (ATA and ATS) were compared in dry and wet condition to determine if the filter walls were swelled when exposed to humidity, which would increase the resistance to breathing. The procedure is further described, and results presented, in Supplemental Appendix B, Table 6.
Statistics
The statistical analyses were done in SPSS for Windows statistical software release 24.0 (SPSS Inc., Chicago, IL., USA). In the no-wind test condition, the results of RES for the HME variance and
Results
The results of RESI and RESE for the tested HMEs in the no-wind condition are presented as mean ± SD of V 30, 90 and 180 L/min in Figure 3. The largest differences in RES were found between different manufacturers of HME, while there were smaller differences in RES between filters/models from each manufacturer. The highest RES was recorded by the CT Masks, followed by Lungplus, Craft, Jonaset and Airtrim. Because Δp exceeded the equipment measuring range for the CT Masks at higher
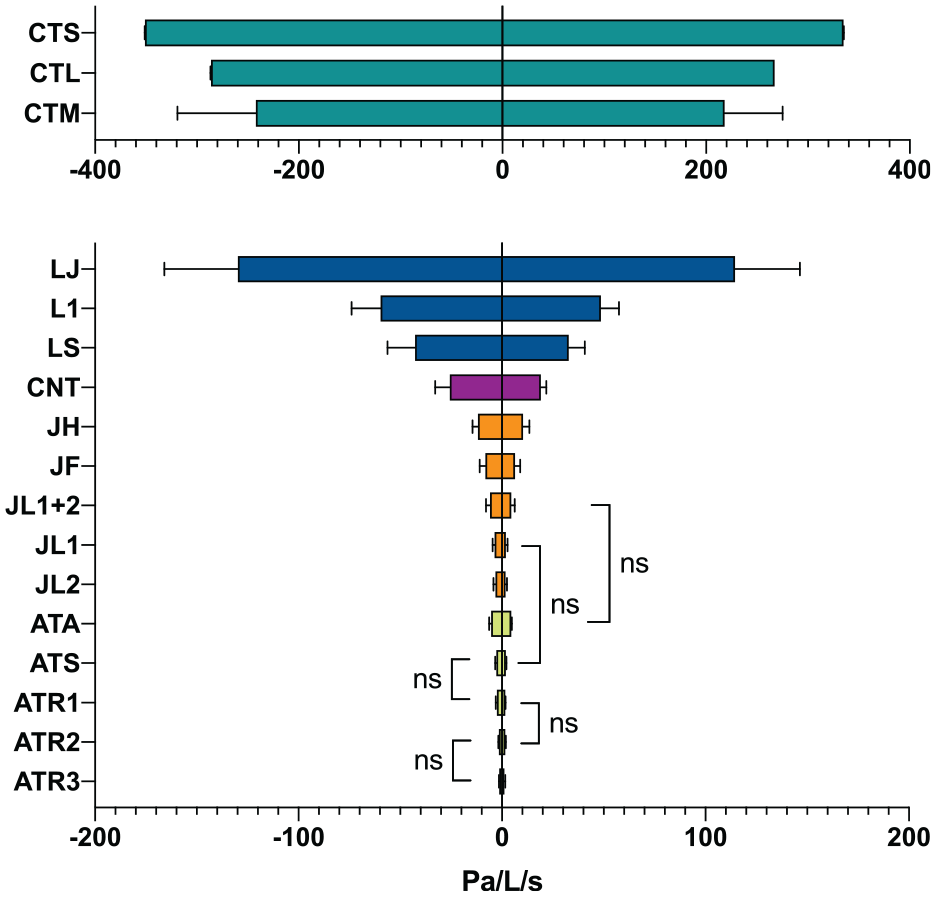
Results (mean ± SD) of inspiratory and expiratory resistance (RESI and RESE) at ventilations 30–180 L/min for seventeen tested heat and moisture exchangers (HME). ATA, ATS, ATR1, ATR2, ATR3: Airtrim with five different filters; JL1, JL2, JL12, JF, JH: Jonaset with two different filters tested separately plus in combination and two face tubes with filters; CNT: Craft, a neck/face tube without any filter; LS, L1, LJ: Lungplus in three different variants; CTL, CTM, CTS: CT masks in three types and sizes (Table 1). All paired comparisons between HME models were significant at p < 0.05, except the paired comparisons indicated by ‘ns’ (not significant (p > 0.05)). p-values for all paired comparisons can be found in Supplemental Appendix C, Tables 7 and 8.
Due to very high reproducibility of the equipment that generated the flow and pressure measurements, the SD for RES was very small. Therefore, even small differences in mean values between different HMEs and flows resulted in significant differences in RES (Figure 3).
Thus, there were significant differences in RESI between the following HMEs and versus all other tested HMEs: ATA, CTL, CTM, CTS, JL12, JF, JH, LS, L1, LJ and CNT (p < 0.001). Significant differences were also established between the following: ATS versus JL2 (p < 0.05) and ATS versus all other HMEs (p < 0.001), except ATR1; JL2 versus ATS (p < 0.05) and JL2 versus all other HMEs (p < 0.001); ATR1 versus all HMEs (p < 0.001), except ATS; ATR2 and ATR3 versus all HMEs (p < 0.001), but not between themselves; JL1 versus JL2 (p < 0.01) and JL1 versus all other HMEs (p < 0.001).
Further, significant differences in RESE were found between the following HMEs and versus all other HMEs: ATR3, CTL, CTM, CTS, JF, JH, LS, L1, LJ and CNT (p < 0.001); ATA was also different versus all HMEs (p < 0.001), except ATA versus JL12; JL12 was different versus all HMEs (p < 0.05), except JL12 versus ATA. ATS was different versus JL2 (p < 0.01) and all other HMEs (p < 0.001), except ATS versus JL1; JL2 was different versus JL1 (p < 0.05), ATS (p < 0.01) and all other HMEs (p < 0.001); JL1 was different versus JL2 (p < 0.05) and all HMEs (p < 0.001), except JL1 versus ATS; ATR1 and ATR2 were different versus all HMEs (p < 0.001), but not between themselves.
In other terms, no differences were found between ATS versus ATR1 and ATR2 versus ATR3 for RESI and ATR1 versus ATR2, ATA versus JL12 and ATS versus JL1 for RESE (Figure 3).
Significant differences (p < 0.001) were also noted in RES between the three
There were also significant differences in RESI and RESE between different headwind conditions, except between the two lowest wind speeds, 0.0 versus 2.8 m/s, where RESI decreased and RESE increased systematically with increased headwind (Table 2): RESI: 0 versus 8.3 (p < 0.05) and 13.9 m/s (p < 0.001); 2.8 versus 8.3 and 13.9 m/s (p < 0.05); 8.3 versus 13.9 m/s (p < 0.01); RESE: 0 versus 8.3 (p < 0.05) and 13.9 m/s (p < 0.01); 2.8 versus 8.3 (p < 0.05) and 13.9 m/s (p < 0.01); 8.3 versus 13.9 m/s (p < 0.001).
Inspiratory (RESI), expiratory (RESE) and mean (RESM) resistance to breathing for four HMEs at headwind conditions 0, 2.8, 8.3 and 13.9 m/s. Mean ± SD across a range of ventilations 30–180 L/min.
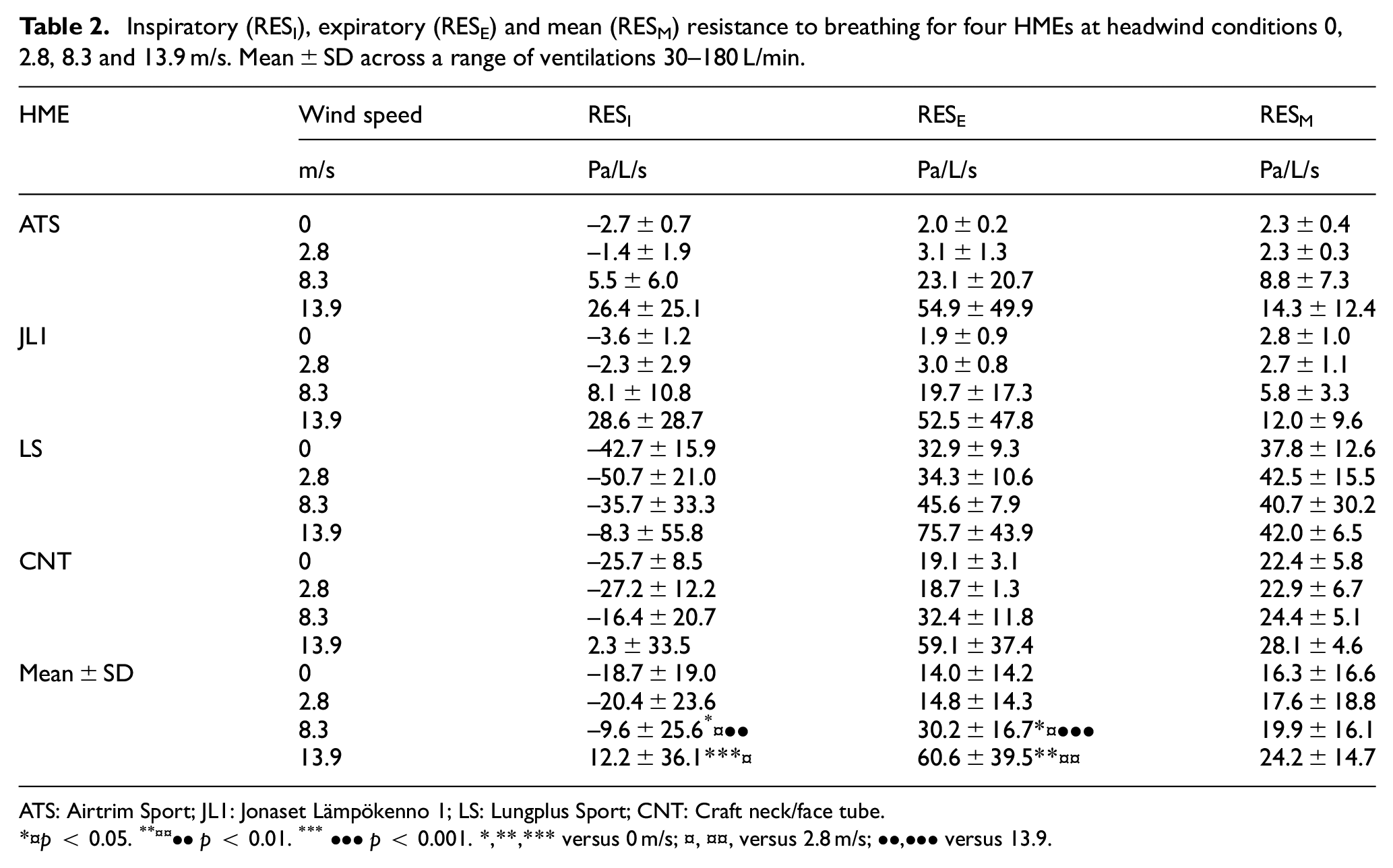
ATS: Airtrim Sport; JL1: Jonaset Lämpökenno 1; LS: Lungplus Sport; CNT: Craft neck/face tube.
p < 0.05. **¤¤••p < 0.01. ***•••p < 0.001. *,**,*** versus 0 m/s; ¤, ¤¤, versus 2.8 m/s; ••,••• versus 13.9.
Also, there was a significant difference (p < 0.05) in RESE between different
Inspiratory (RESI), expiratory (RESE) and mean (RESM) resistance to breathing for four HMEs at ventilations (
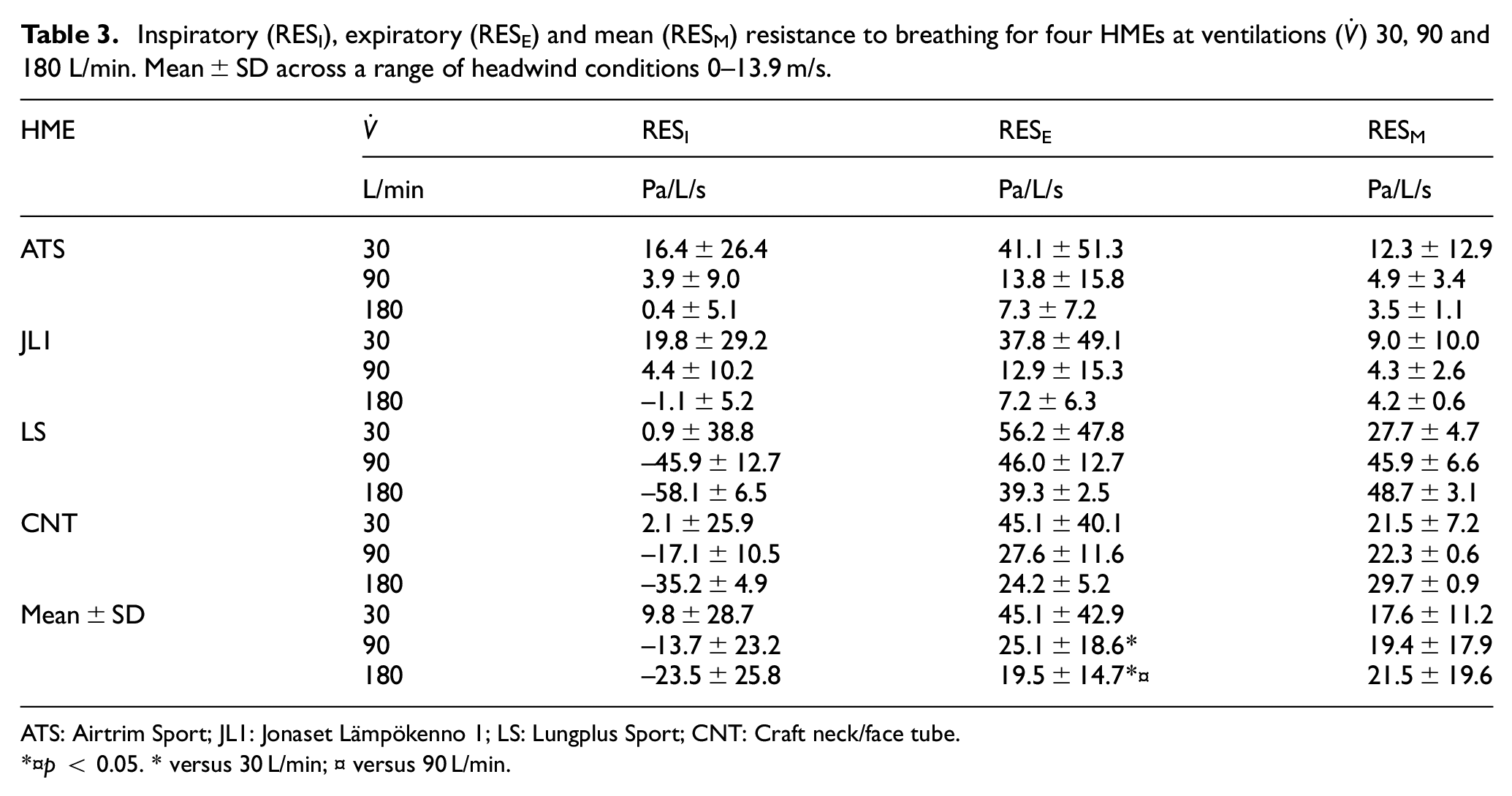
ATS: Airtrim Sport; JL1: Jonaset Lämpökenno 1; LS: Lungplus Sport; CNT: Craft neck/face tube.
p < 0.05. * versus 30 L/min; ¤ versus 90 L/min.
Confidence intervals (CI), effect sizes (Cohen’s d) and p-values for RES between different HMEs,
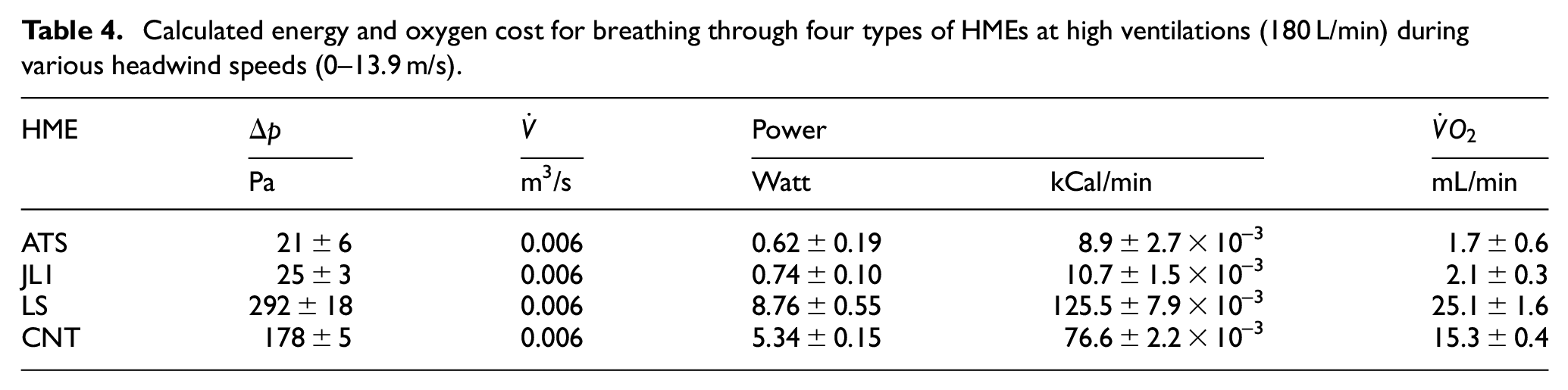
The PREQ for breathing through each of the four representative HMEs is presented in Table 4. The calculated energy requirement is very small, at less than 9 W and 130 × 10-3 kCal/min, with a maximal oxygen cost of 25 mL/min.
Calculated energy and oxygen cost for breathing through four types of HMEs at high ventilations (180 L/min) during various headwind speeds (0–13.9 m/s).
Discussion
To the best of the authors’ knowledge, this is the first study to evaluate RES in various heat and moisture exchangers available on the market, intended for use during physical activity in the cold. The results showed significant differences in RES between HMEs from different manufacturers, while the difference was small, and in some cases not significant, between different models/filters within the same brand. There was a positive association between RES and
The HMEs could be grouped into four categories based on RES: (1) Airtrim and Jonaset models, (2) Craft neck/face tube, (3) Lungplus models and (4) CT Mask models. The lowest RES occurred in the HMEs from the Airtrim and Jonaset brands, which use large filters, but these HMEs also have relatively large dead space. The Craft neck/face tube had higher RES compared to the Airtrim and Jonaset models, but RES was still relatively low for this type of product which offers both facial and respiratory protection.
The Lungplus models, which are designed to be held in the mouth, had higher RES, likely due to the smaller cross-sectional area. These HMEs probably approach the level at which RES may interfere with the user’s normal ventilation and WOB. As a comparison, the difference in RES between the Lungplus models is approximately equivalent to the RES found between hardware of aerobic energy measurement systems.
29
This difference has also been found to result in significantly different breathing frequency and ventilation during submaximal and maximal exercise, but no difference was noted in tidal volume, energy cost and performance in high-ventilating athletes.
28
In a similar study where the difference in RES between the hardware was smaller, on par with the actual RES for the LS model, less RES resulted in lower submaximal energy cost for both recreational and trained endurance athletes, while the ventilation was lower only for the latter group.
27
For the maximal test, there were no differences in ventilation and
The HMEs with the highest RES were the CT Mask models. It was not possible to measure RES on the highest ventilation for this type of HME because Δp exceeded the equipment measuring range. However, based on the RES from the lowest ventilation, the RES of these models at low ventilations exceeded several times the RES found in hardware of aerobic energy measurement systems. 29
When a headwind was introduced, RES decreased during inspiration and increased during expiration; this shift is particularly prominent for low ventilations. Thus, a slightly different distribution of WOB may result between the respiratory muscles. The influence of headwind showed that RESI and RESE changed significantly, except in the first scenario from no wind to low wind speed (2.8 m/s). As shown in Table 2, the values for RESI became less negative or even positive with increasing headwind, while the RESE values increased even more. However, as one decreased and the other increased, the average RES (RESM) remained unchanged. A trend developed towards an increased RESM with increased headwind for the ATS and JL1 HMEs, but not for LS and CNT, which is likely due to the higher permeability of their large filters, which also results in slightly higher sensitivity to headwind speeds. Regarding RES between different
The energy requirement and oxygen cost for breathing through the HMEs are relatively small, but one cannot ignore that a small effect could still influence athletes’ performance (Table 4). Given the perspective that cross-country skiers and biathletes have a
The calculations in Supplemental Appendix A, Table 5, shows that the negative effect of HME dead space on pulmonary gas fractions decreases with increased tidal volume. For submaximal ventilations with not fully utilised inspiratory and expiratory residual volumes, the negative impact on pulmonary gas fractions when using HME can be compensated for by an increase in VT similar to the HME volume or an increase in breathing frequency. However, the WOB may increase, thus impairing the user’s mechanical efficiency. Whether a deterioration of the pulmonary gas fractions has any practical significance for the user’s performance depends on whether the partial pressure change of the gases has an effect on the gas transfer across the alveolar-capillary membrane. Such a scenario could cause negative consequences for O2 saturation and CO2 removal of the arterial blood, which should become more critical with low ambient air pressure occurring at higher altitudes.
The calculations presented in Supplemental Appendix B, Table 6, show that the Airtrim filter cell walls swelled after being exposed to a water bath. Thus, moisture causes a reduction in the size of the cells for this type of paper-like filter, which likely results in an increased RES. However, the increase in filter wall area was similar to the difference between the two tested filters. The expected increase in RES should therefore be approximately the same as the small difference between the two filters. Moreover, the filters became considerably softer when wet as compared to the dry condition. A filter that holds more moisture may possibly contribute to more evaporation, but conceivably is also an increased risk of ice formation. Of further note was the formation of crystals on the bottom of the water bath, consisting mostly of salt, which shows that the manufacturer is likely to prepare the filters with salt in order to counteract icing. Another explanation may be that the salt helps to keep the fibers together when the filter gets wet.
The findings from the current study show very small negative effects of the use of HMEs on athletes’ physiology and performance, such as changed pulmonary gas fractions due to increased dead space, resistance to breathing, and energy requirement for driving the inhaled and exhaled air through the filter. At least during training, any moderate to high-intensity exercise, with corresponding ventilation and energy expenditure, should be possible without decisive influence in these respects. However, conceivable disturbances, such as discomfort of wearing an HME and possible ice formation in the filter, can disturb the user, even during training. For professional work and light physical activities where ventilation and VT are usually low, as well as in combination with asthma and being unaccustomed to exercise, the use of an HME can have more noticeable effects on the user. In order to investigate the possible occurrence of ice formation, athletes and coaches can inspect the filters during training in the cold so as to investigate whether this can cause problems or not with ventilation and increased RES and WOB. Whether a wet filter surface affects the shear stress of the boundary layer and thus RES was not investigated in this study. Variations in air temperature and density likely have some minor effect on RES. Lower temperature and altitude increase the density of the air and vice versa. Leakage is a factor that can greatly change RES, WOB, and temperature and humidity of the inhaled air. However, this study did not address leakage issues resulting from poor fit or equipment issues. During this study, certain types of HME had to be taped to the plastic face surface to avoid leakage while taking measurements. Realizing that people will not have HMEs taped to their faces, possible leakage may be unavoidable.
Pros and cons exist for the different HME designs in terms of dead space, RES, WOB, sensitivity to wind conditions and possible leakage problems. Potential negative consequences of HME usage due to RES, dead space and WOB on physiology and performance measures, as well as possible positive effects in preventing asthma in winter endurance athletes, are topics for future investigation. With so little difference in RES values between filters, the multitude of filter options seems unnecessary. It remains to be seen whether differences between the various filters influence the ability of an HME to humidify and heat the inhaled air.
Conclusion
Unsurprisingly, the results of this study show that breathing resistance varies between HMEs depending on design, model, filters, minute ventilation, and wind conditions. Most HMEs on the Nordic market have low breathing resistance and should only affect work of breathing to a very small extent, even at high ventilations and headwind speeds. The effect of HME dead space on pulmonary gas fractions varies depending on the HME volume and size of the tidal volume.
Supplemental Material
sj-pdf-1-pip-10.1177_1754337120980661 – Supplemental material for Breathing resistance in heat and moisture exchanging devices
Supplemental material, sj-pdf-1-pip-10.1177_1754337120980661 for Breathing resistance in heat and moisture exchanging devices by Mats Ainegren, Helen Hanstock and Nikolai Stenfors in Proceedings of the Institution of Mechanical Engineers, Part P: Journal of Sports Engineering and Technology
Footnotes
Acknowledgements
Many thanks go to the research engineers Per Skoglund, William Sjöström and Dr Carlos Botero (Sports Tech Research Centre, Mid Sweden University) for making the head in ABS plastics and for scanning and calculating the HME filter areas.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to thank The Swedish Heart-Lung Foundation for financial support for the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.