
Abstract
Background:
We sought to investigate the rate of radial artery occlusion (RAO) after same-day dual radial artery puncture. The trans-radial arterial approach (TRA) for diagnostic and interventional procedures has risen significantly in the United States. Although becoming more commonly performed, TRA is not without risk, and a potential complication is RAO. The rate of RAO after same-day dual artery puncture is unknown.
Methods:
A retrospective analysis of 27 patients who underwent same-day dual radial artery puncture for percutaneous coronary intervention (PCI) at our institution (Providence Heart Institute in Southfield, MI, USA) from November 2011 to December 2013 were included after initially presenting for cardiac catheterization at a non-PCI-capable facility. The study patients were asked to follow up for evaluation of the radial artery, including obtaining a duplex ultrasound evaluation.
Results:
The mean age of the patients was 65 years old with 66% of the patients being male. Of the 27 study participants, there were no symptoms reported that were related to RAO. Overall, one (3.7%) patient had an absent radial pulse. The modified Allen’s test was normal in all of the patients with a mean return of palmar flush time of 4 seconds. Duplex ultrasound revealed subtotal RAO in four (14.8%) patients and no patients experienced total occlusion following the intervention.
Conclusion:
Dual radial artery puncture appears to be a well-tolerated and viable strategy in patients that are transferred to a PCI-capable hospital for coronary interventions.
Introduction
Coronary artery disease (CAD) is the leading cause of mortality and morbidity in the United States. 1 Strategies to improve morbidity and mortality in patients suffering from CAD include the optimization of medical therapy and either percutaneous coronary intervention (PCI) or a surgical bypass procedure. Continuous advancements in less invasive percutaneous intervention equipment, such as drug-eluting stents and delivery catheters in addition to the proven benefit of antiplatelet and periprocedural anticoagulants has resulted in a shift toward PCI over surgical interventions for primary revascularization for CAD. 2 Radial over femoral arterial access for PCI demonstrates increased safety and fewer complications to the patient, but these approaches are not without risk. One of the most common complications associated with PCI is bleeding from the vascular access site. In fact, the risk of retroperitoneal bleeding ranges from 0.15% to 6% in the transfemoral approach. 3 Although this risk is small, it can be potentially lethal.
Accessing the coronary anatomy (left heart catheterization) via the radial artery approach has evolved as a viable and successful technique for both diagnostic and interventional procedures. The radial artery approach offers several advantages over traditional femoral artery access, such as negligible risk of internal bleeding and easily identifiable external bleeding that can be controlled by arterial compression for hemostasis. 4 Additionally, percutaneous radial artery approaches eliminate the need for prolonged immobilization after the procedure, which is anecdotally more tolerable for the patient. One of the few post-procedure complications of radial artery catheterization is radial artery occlusion (RAO). 5
The main blood supply to the hand comes from both the radial and ulnar arteries. The ulnar artery can provide single supply to the hand if RAO occurs. As a result, RAO from catheterization is typically clinically silent. However, the presence of occlusion can preclude future arterial access and catheterization through this vessel.
While previous studies have identified repeat canalization of the same radial artery as a risk factor for RAO, 6 we hypothesized that with the use of modern sheaths and catheters, anticoagulant therapy and vasodilators, this complication can be minimized and possibly eliminated. We examined a small cohort of patients who underwent diagnostic catheterization via the radial artery at a non-PCI-capable facility. These patients were found to have critical coronary artery stenosis and were subsequently transferred to our facility for urgent intervention. All of these patients underwent same-day dual radial artery puncture for PCI to the culprit coronary artery, defined as a second procedure within 24 h of the initial catheterization.
Methods
After approval by the Internal Review Board at St. John-Providence Health System, MI, USA (approval #381829), a retrospective review of all patients who received same-day dual radial artery puncture for PCI from January 2012 to December 2013 was performed. Inclusion criteria included patients older than 18 years of age who underwent radial site diagnostic coronary angiography at a facility unable to perform elective PCI and then transferred to a PCI-capable hospital with a second radial artery access on the same side within 24 hours. Patients who were at least 18 years of age and underwent radial artery access for PCI and were followed up in the outpatient clinic were included in the study. Patients younger than 18 years of age, unwilling to consent, or lost to follow up were excluded from the study. All patients signed informed, written consent to be included within the study.
Sheath removal and hemostasis of the radial artery protocol is an important discussion. Patent hemostasis was achieved by inflating the TR band (Terumo Corporation, Tokyo, Japan) until hemostasis was achieved. Air was slowly removed from the TR band bladder until pulsatile flow was noted and then 2–3 more milliliters of air were reinserted. Patent hemostasis was confirmed with pulse-oximetry waveforms.
After discharge, patients were contacted to follow up in the outpatient clinic for evaluation of radial artery patency. Radial artery palpation, modified Allen’s test, and Barbeau’s test were used to assess the patency of the palmar arch prior to radial access. Allen’s test, modified Barbeau’s test, and radial artery ultrasound was then used to assess the radial artery during post-PCI follow up several days to weeks following the PCI (see Figure 1).

Flow chart of patient follow up.
Prior to radial access, the modified Allen’s test was performed by asking the patient to clench their fist and hold it while the examiner compressed the radial and ulnar arteries simultaneously. This technique temporarily restricts blood flow to the hand, as evidenced by pale blanching of the skin. The patient was then instructed to unclench their fist while the examiner released compression of the ulnar artery. A normal modified Allen’s test was recorded if the patient’s palmar color returned to normal within 7 seconds, indicating adequate collateral circulation. 7
Next, a modified Barbeau’s test was performed. 8 A pulse oximeter was placed on the patient’s thumb until normal arterial waveform was confirmed on the monitor. The examiner compressed both the radial and ulnar arteries to confirm the loss of waveform on the monitor. The examiner then released the ulnar compression and observed the monitor for return of normal arterial waveforms. The following grading systems were used: type A depicted no loss of waveform; type B exhibited transient loss of waveform; type C showed transient loss of waveform that was visibly dampened during recovery over the course of 2 minutes; and type D was complete loss and no return of arterial waveform within 2 minutes. Reverse modified Barbeau’s test was performed to assess radial artery patency post-PCI.
During diagnostic coronary intervention, antispasmodics and anticoagulation were given at the operator’s discretion. While the dose and choice of antispasmodics was variable amongst operators, all patients received heparin and nitroglycerin through the radial artery sheath and only a few of the patients were given verapamil through the radial sheath. All patients had a therapeutic activated clotting time (ACT) during PCI defined as an ACT > 250.
Duplex ultrasound was performed at the patient’s office follow-up visit to evaluate for patency along with presence of atherosclerotic disease by the department of radiology at our institution. Gray scale along with color and spectral Doppler analysis was performed within the involved radial artery along with use of contralateral radial artery for comparison if abnormality or variation was detected. Radial artery diameter, along with degree of atherosclerotic plaque characterized as mild, moderate, or severe was recorded. The peak systolic velocity (cm/sec) along with spectral Doppler waveform characteristics of either multiphasic (normal) or monophasic (abnormal) were recorded. Complete occlusion was described as a lack of color and spectral Doppler flow within the arterial lumen.
At the time of post-PCI evaluation, a questionnaire was completed by each patient inquiring about symptoms during the index procedure at the transferring hospital along with symptoms after the interventional procedure.
Each angiogram and electronic medical record was reviewed for baseline demographics, including age, sex, race and body mass index. Co-morbid risk factors such as hypertension, diabetes mellitus, dyslipidemia, current or former tobacco use and chronic kidney disease were recorded. Sheath size and catheter use in addition to periprocedural medications administered were documented. Complications that occurred during or after the procedure were included.
Results
In total, 33 patients met inclusion criteria and 27 patients were enrolled. A total of six patients were either unable to be contacted or refused to consent for the study. The mean age of the cohort was 65 (±15) years with predominantly White males with traditional cardiovascular risk factors (Table 1).
Patient demographics and co-morbid risk factors.

The initial diagnostic procedure characteristics are illustrated in Table 2. In total, 2 of the 27 procedures were elective (7.4%), while 24 (88.9%) were urgent and 1 (3.7%) was emergent. The right radial artery was the preferred vascular access site in 24 (88.9%) of the cases. A 5 French Terumo Glidesheath was used in all initial diagnostic angiogram procedures. All patients received a standard dose of 5000 units of intra-arterial or intravenous heparin and intra-arterial nitroglycerin during the procedure and successful patent hemostasis was achieved after each procedure using a TR band (Terumo Corporation, Tokyo, Japan). Only three (11.1%) of patients received verapamil during the procedure at the discretion of the operator.
Diagnostic coronary procedure characteristics.

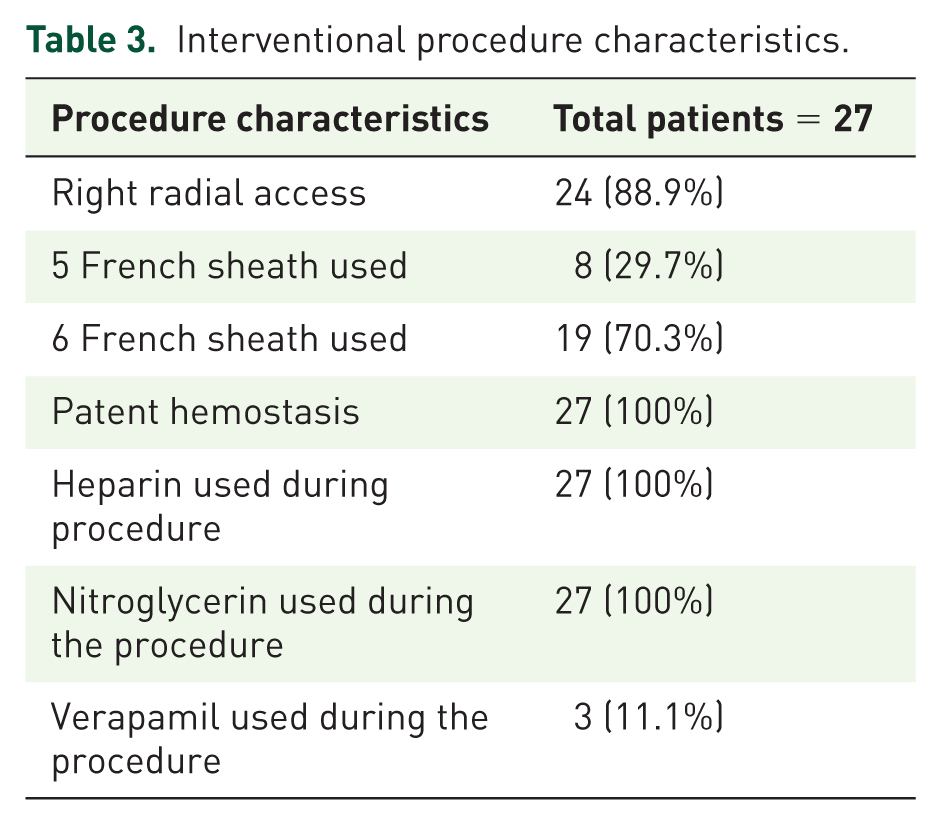
Characteristics pertaining to the coronary interventional procedure are shown in Table 3. All patients underwent same-day revascularization within 24 h of the diagnostic cardiac catheterization. The intervention was performed using a 6 French Glidesheath in 19 (70.3%) of the cases, with the remaining cases using a 5 French sheath/guiding system. All patients received heparin to maintain a therapeutic ACT > 250 s and nitroglycerin during the procedure along with successful patent hemostasis post-procedure. Additionally, three patients (11.1%) received verapamil during the interventional procedure.
Interventional procedure characteristics.
Procedural PCI characteristics are outlined in Table 4. The mean fluoroscopy time was 8.6 min for the diagnostic procedure and 15.6 min for the interventional procedure. The average contrast dose received was 125 ml of low-osmolar nonionic contrast agent and the mean time between the procedures was noted at 14 h. PCI of the left anterior descending artery occurred in 10 (37%) patients, left circumflex artery in 3 (11.1%) and the right coronary artery in 1 (3.7%). Double vessel PCI of the native coronary artery along with PCI of a bypass graft were treated in 3 (14.8%) and 1 (3.7%) case, respectively (Table 5).
Hematology and catheterization laboratory characteristics.

INR, international normalized ratio; PCI, percutaneous coronary intervention; PTT, partial thromboplastin time.
Coronary vessel PCI characteristics.

LAD, left anterior descending artery; LCX, left circumflex artery; PCI, percutaneous coronary intervention; RCA, right coronary artery.
None of the patients experienced any symptoms peri-procedure or post-procedure, regardless of the procedural outcome. Furthermore, none of the patients experienced subjective RAO symptoms at their office follow-up appointment or at the time of the duplex ultrasound evaluation. All patients indicated that they felt very comfortable during both the procedure and during post-procedure care and stated that they would elect to undergo a radial artery approach in the future if repeat catheterization was required.
During follow-up examination, 23 (85.1%) patients had a fully palpable radial pulse (grade 2–3), 3 (11.1%) patients had a weak radial pulse (grade 1) and 1 (3.7%) patient did not have a palpable radial pulse (grade 0).
All of the patients demonstrated a normal modified Allen’s test with a 4 second mean return of palmar color. A total of 23 (85.1%) patients had either type A or B Barbeau’s test indicting no transient loss of waveform. Overall, 4 (14.9%) patients had type C Barbeau’s test indicting a transient loss of waveform with dampening in recovery and no patients displayed a type D Barbeau’s test, which correlates with a complete loss of waveform (Table 6).
Post-procedure office follow-up examination.
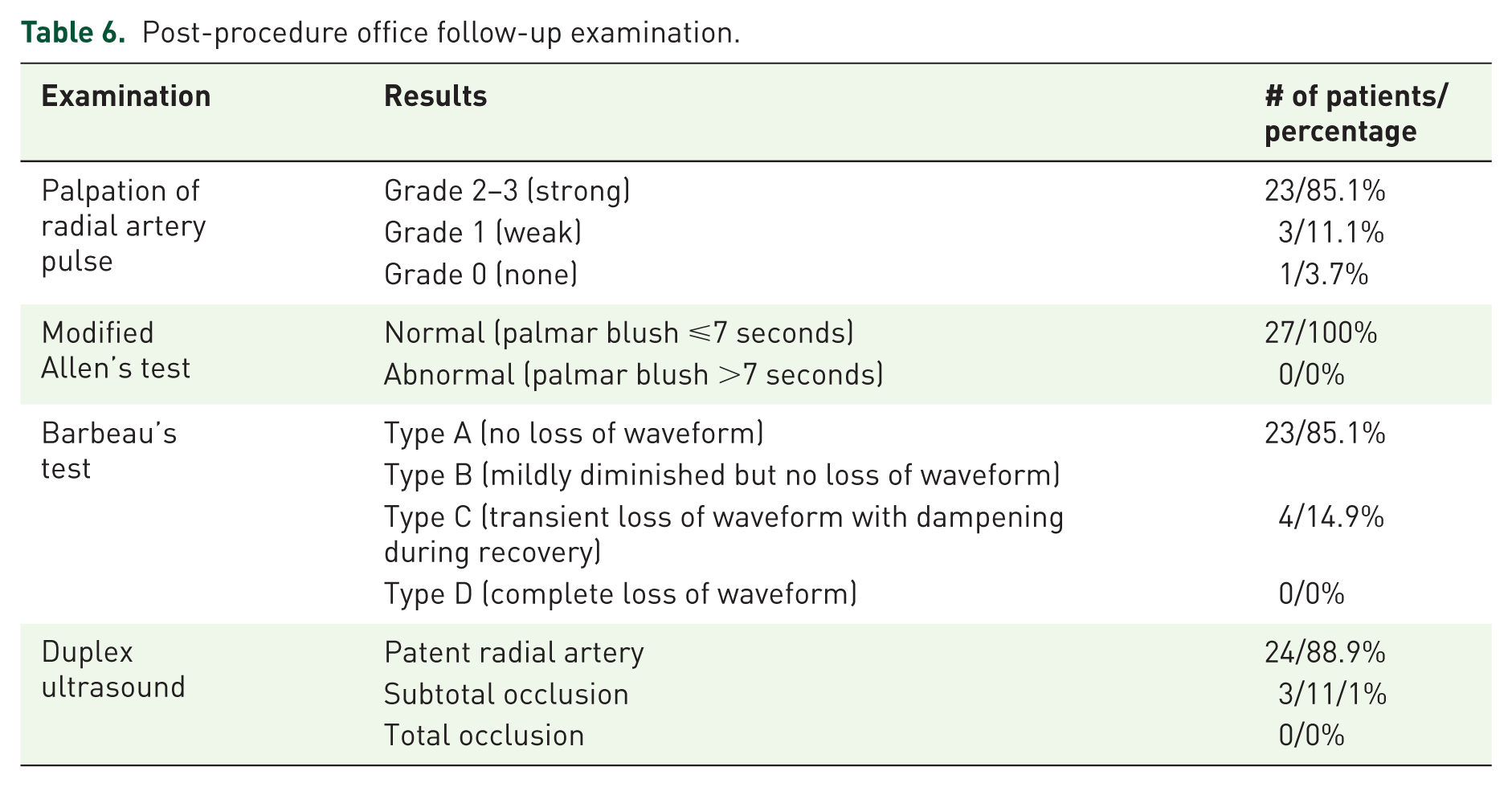
Duplex ultrasound revealed subtotal RAO in 3 (11.1%) patients with type C Barbeau’s test (Figure 1, example). The remaining 24 (88.9%) patients had no evidence of occlusion (subtotal or total) when examined by duplex ultrasound (Table 6).

Duplex ultrasound of the right radial artery at the distal forearm. Color Doppler shows evidence of subtotal occlusion of the radial artery at the postoperative follow-up appointment.
Discussion
The evolution of percutaneous cardiac catheterization access sites has drastically improved from the original approach involving cut-down access to the brachial artery for intervention. Over the past decades, less invasive and more controlled arterial access has been achieved. Previously the standard and preferred method of arterial access, the femoral artery approach is quickly falling out of favor by interventionalists worldwide due to safer, less complicated access sites like the radial artery.9–14 Amongst other reasons, the radial artery has less frequent and less major bleeding site complications compared with the femoral artery access site. For this reason, the radial approach has become the preferred method of intervention in Europe, Canada and other countries outside of the United States.15,16 However, use of the radial artery continues to gain favor in the United States for elective catheterization given the improved outcomes and increased patient comfort compared with the femoral approach. Moreover, the RIFLE STEACS trial demonstrated improved outcomes for the radial approach in patients undergoing emergent intervention for acute coronary syndromes. 17
Since being first described in 1989 and 1993,15,16 the radial artery puncture for PCI has continued to become more popular; however, the risks associated with radial artery access still exist. Historically, one of the most commonly reported risks included radial artery occlusion, occurring in up to 15–20% of procedures in 2005. 18 However, due to advancements in guidewire, sheath and catheter technology, the risk of RAO has reportedly dropped dramatically to only 1–10% at 24 h and 2–4% at 30 days post-procedure. 19 The use of antiplatelet and anticoagulant medications has played a major role in improving these complication rates, as well. Furthermore, antispasmodic agents like nitroglycerin and verapamil have aided the interventionalist in limiting complications secondary to radial artery vasospasm.
Utilizing the radial artery approach for diagnostic and interventional procedures whenever technically feasible is ideal compared with the traditional femoral access. Lower complication rates from bleeding and fewer infections make the radial approach superior to femoral access, along with the RIFLE STEACS trial showing improved major adverse cardiovascular events. When compared with the traditional femoral approach, the trans-radial approach for intervention was associated with a 78% reduction in bleeding and 80% reduction in the need for blood transfusion post-procedure. 20
While there were four patients within the small sample size that developed RAO, this appears to not be clinically relevant since palmar arch flow was adequate as assessed by follow up Allen’s and Barbeau’s tests. As evidenced in our study, the safety of same-day radial artery puncture is significant and can be performed, especially when concerns for RAO are feared. However, the results within this study need to be confirmed by large, randomized controlled trials.
Study limitations
There are several limitations to our study. First, the small patient sample size may underestimate the true incidence of RAO after same-day dual radial artery puncture and further studies are needed with larger enrollment numbers. Second, the lack of randomization introduces the possibility of selection bias in deciding which patients were suitable to proceed with dual radial artery puncture for intervention. Next, in order to accurately assess whether or not each patient with subtotal occlusion of the radial artery was caused by the same-day dual arterial access intervention, pre-procedure duplex ultrasound would need to be performed. During follow-up visitation the patients that did experience RAO had some degree of calcification and pre-procedural duplex ultrasound would have been beneficial to assess for stenotic lesions prior to radial artery puncture during our study. Also, it is important to note that the risk of RAO and thrombosis is highest within the first 24 h. Another consideration for future investigation would be to perform upper extremity angiography prior to repeat access of the radial artery to assess patency. Hence, the retrospective design of this study limits our findings in this regard. Next, the total sheath dwelling time is variable between patients. While fluoroscopy time was documented for each procedure, the sheath dwelling time would be a more beneficial marker for RAO and future investigations should take this into account. These future investigations could also assess the patients that developed RAO to examine whether any statistically significant differences exist with regard to sheath sizes, procedural confounders, or patient demographics. Furthermore, the lack of inferential statistics is a limitation to the study findings and finally, the possibility of recall bias may have skewed the responses on the questionnaire provided to the patients at the time of follow up.
Conclusion
This is the first study reporting the rate of RAO after same-day dual radial artery puncture. Although we identified four patients with subtotal RAO post-procedure, each patient remained symptom free and without limitations. Dual radial artery puncture appears to be a viable and well-tolerated strategy for patients who must be transferred to a PCI-capable hospital for coronary interventions.