
Abstract
Objective
To investigate the preventive effect of hydration combined with reduced glutathione on contrast-induced nephropathy (CIN) after coronary intervention therapy in elderly Chinese patients with diabetes.
Methods
Patients with diabetes aged ≥65 years, who received percutaneous coronary intervention (PCI) between 1 August 2016 and 31 December 2018, were enrolled and randomized into two groups: patients treated with hydration combined with reduced glutathione (treatment group) and patients who received hydration alone (controls). Serum creatinine and creatinine clearance levels were measured in all patients before PCI and then daily for 3 days after PCI. Occurrence of CIN (the primary endpoint) was defined as serum creatinine value 25% or 44.2 mmol/l (0.5 mg/dl) above baseline at 72 h after an exposure to contrast medium.
Results
A total of 396 patients were included (treatment group, n = 204; and controls, n = 192). The CIN occurrence rate in the treatment and control group was 5.88% and 6.77%, respectively, with no statistically significant between-group difference.
Conclusion
In elderly patients with diabetes receiving PCI, the risk of CIN was not effectively lowered by hydration combined with reduced glutathione.
Keywords
Introduction
Contrast-induced nephropathy (CIN), the third major cause of hospital-acquired renal function failure,1–3 is a complex syndrome that causes acute kidney injury, usually as a result of direct exposure of blood vessels to contrast agents. Therefore, it is seen as one of the most critical clinical problems following percutaneous coronary intervention (PCI), particularly in elderly patients.4,5 Diabetes mellitus has also been defined as an independent and important risk factor for CIN in several studies. 6 In addition to old age, hypotension due to cardiac dysfunction plays an important role in the occurrence of CIN. 1
At present, methods for CIN prevention are very limited. Although considered to be an effective method, conventional hydration therapy is inadequate from the perspective of clinical practice, and other than intravenous hydration, advisable methods to prevent CIN remain unclear.7–9 Oxidative stress has been shown as a major leading factor in the development of CIN.10–12 Many factors may lead to a rise in reactive oxygen species (ROS) levels in diabetes, such as decreased ROS destruction by catalase (CAT), superoxide dismutase (SOD) and glutathione peroxidase (GSH–Px) antioxidant enzymes, or increased ROS production by enzymatic or nonenzymatic reactions. The fluctuation of enzymes involved in regulating ROS levels make the tissues vulnerable to oxidative stress. 13 As an effective antioxidant, reduced glutathione may potentially prevent CIN. Other antioxidants, such as sodium bicarbonate, N-acetylcysteine, ascorbic acid and statins, do not appear to be effective in preventing CIN. 13 However, available information is limited about how reduced glutathione may potentially prevent CIN and benefit elderly Chinese patients with diabetes. Thus, the aim of the present study was to investigate whether hydration combined with reduced glutathione is more effective than hydration alone in preventing CIN in this patient population.
Patients and methods
Study population
This randomized-controlled trial included all patients with severe coronary heart disease and type 2 diabetes mellitus, aged ≥65 years, who received PCI at Taizhou First People’s Hospital, an affiliated hospital of Wenzhou Medical University, between 1 August 2016 and 31 December 2018. Patients with creatinine clearance levels ≥60 ml/min were included, and patients were diagnosed with type 2 diabetes according to the 1999 World Health Organisation diagnostic criteria for diabetes. Patients who met the following criteria were excluded from the study: (1) refusal to participate in the clinical trial; (2) refusal to receive PCI treatment; (3) perioperative use of any nephrotoxic drugs; (4) severe hepatic and renal failure; (5) severe infectious diseases; (6) New York Heart Association functional classification (NYHA) class >3; (7) haemodynamic instability, including systolic blood pressure <90 mmHg; (8) coronary artery lesions that did not meet the revascularization treatment standard; (9) coronary artery anatomy not suitable for PCI; and (10) allergic reaction to contrast media and reduced glutathione.
The study was approved by the ethics committee of Taizhou First People's Hospital, and written informed consent was obtained from all participants. The study was registered with the Chinese clinical trial registry (registration number: ChiCTR1900028664).
Medication regimen
According to the American Heart Association/American College of Cardiology guidelines for secondary prevention for patients with coronary artery disease, 14 all patients taking part in this trial were undergoing dual antiplatelet and other therapies, including angiotensin-converting enzyme inhibitors/ angiotensin II receptor blockers, β-blockers and statins. All patients were receiving oral and/or insulin hypoglycaemic treatment.
Study design
This was a non-blind randomized, controlled clinical trial, in which Chinese patients aged ≥65 years were asked to participate. Patients were randomized to two groups using a computer-generated randomization schedule, as follows: (1) control group, patients scheduled to receive hydration treatment comprising a saline drip from 6 h before the operation to 12 h after the operation, at a speed of 1 ml/kg/h; or (2) treatment group, patients scheduled to receive hydration via saline drip plus 180 mg reduced glutathione (Shanghai Fudan Forward S&T Co., Ltd, Shanghai, China; diluted with 250 ml saline) daily, by intravenous drip for 4 days during PCI (6 h before and 3 days after the operation). Non-ionic isotonic contrast agent (Shanghai Bracco Sine Pharmaceutical Co., Ltd, Shanghai, China) was used for coronary angiography. Routine baseline cardiovascular and blood parameters, including left ventricular ejection fraction, amino-terminal pro-brain natriuretic peptide and low-density lipoprotein cholesterol, were obtained in all patients. The same technician (EX) in the same laboratory was appointed to measure the serum creatinine level four times, including once before the operation and once daily for three days after the operation. Briefly, venous blood (2–4 ml) was collected and sent to be analysed. Within 2 h of sample collection, the serum was separated by centrifugation at 1 509 g for 10 min at room temperature, and assayed for serum creatinine level using a Hitachi LaboSpect 008 AS automatic biochemical analyser (Hitachi Hi Tech Co., Ltd., Shanghai, China), according to the manufacturer’s instructions. The primary endpoint was occurrence of CIN, which was defined as an increase in serum creatinine of >25% or an absolute value increase of ≥0.5 mg/dl at 72 h following exposure to the contrast agent. 15 Some studies have used a creatinine increase of 0.3 mg/dl as diagnostic criteria for contrast-induced nephropathy. 16 However, use of this standard has mainly involved patients with ST elevation myocardial infarction, and patients in the present study were more widely distributed. In addition, the application of a value increase of 0.3 mg/dl would have increased the nephropathy incidence rate and enlarged the effect of error detection. In view of these factors, the conventional criteria were adopted.
Statistical analyses
The main statistical software used in this study was SPSS, version 19.0 (SPSS, Inc., Chicago, IL, USA). Continuous variables with normal distribution are reported as mean ± SD. Comparisons between means were performed using Student's t-test. Categorical variables are presented as number (%) and were analysed by χ2-test or Fisher's exact test. A P value ≤ 0.05 was considered to be statistically significant.
Results
A total of 396 patients were included in this study (hydration alone [control] group, n = 192 and combined [treatment] group, n = 204). A summary of baseline demographic, clinical and laboratory data for all patients is shown in Table 1. There were no statistically significant differences in baseline parameters between the two patient groups. The mean ± SD values for serum creatinine and creatinine clearance, measured at all four time-points in this study, are summarized in Table 2. The mean serum creatinine value increased daily in both groups, while the mean creatinine clearance rates decreased in both groups over the 3 days following PCI. No statistically significant differences were found in mean serum creatinine (P = 0.33) or mean creatinine clearance (P = 0.20) between the two groups at 3 days following PCI.
Demographic and baseline characteristics in patients with severe coronary heart disease and type 2 diabetes mellitus, aged ≥65 years, who were randomized to receive percutaneous coronary intervention and hydration with reduced glutathione (treatment group) or hydration alone (control group).

Data reported as mean ± SD, n, or n (%).
NYHA, New York Heart Association; LVEF, left ventricular ejection fraction; NT-ProBNP, amino-terminal pro-brain natriuretic peptide; SCr, serum creatinine; Ccr, creatinine clearance; LDL-C, low-density lipoprotein cholesterol; ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin II receptor blockers.
There were no statistically significant between-group differences (P > 0.05; Student’s t-test, χ2-test or Fisher’s exact test).
Evaluation of contrast-induced nephropathy in patients with severe coronary heart disease and type 2 diabetes mellitus, aged ≥65 years, who were randomized to receive percutaneous coronary intervention and hydration with reduced glutathione (treatment group) or hydration alone (control group).
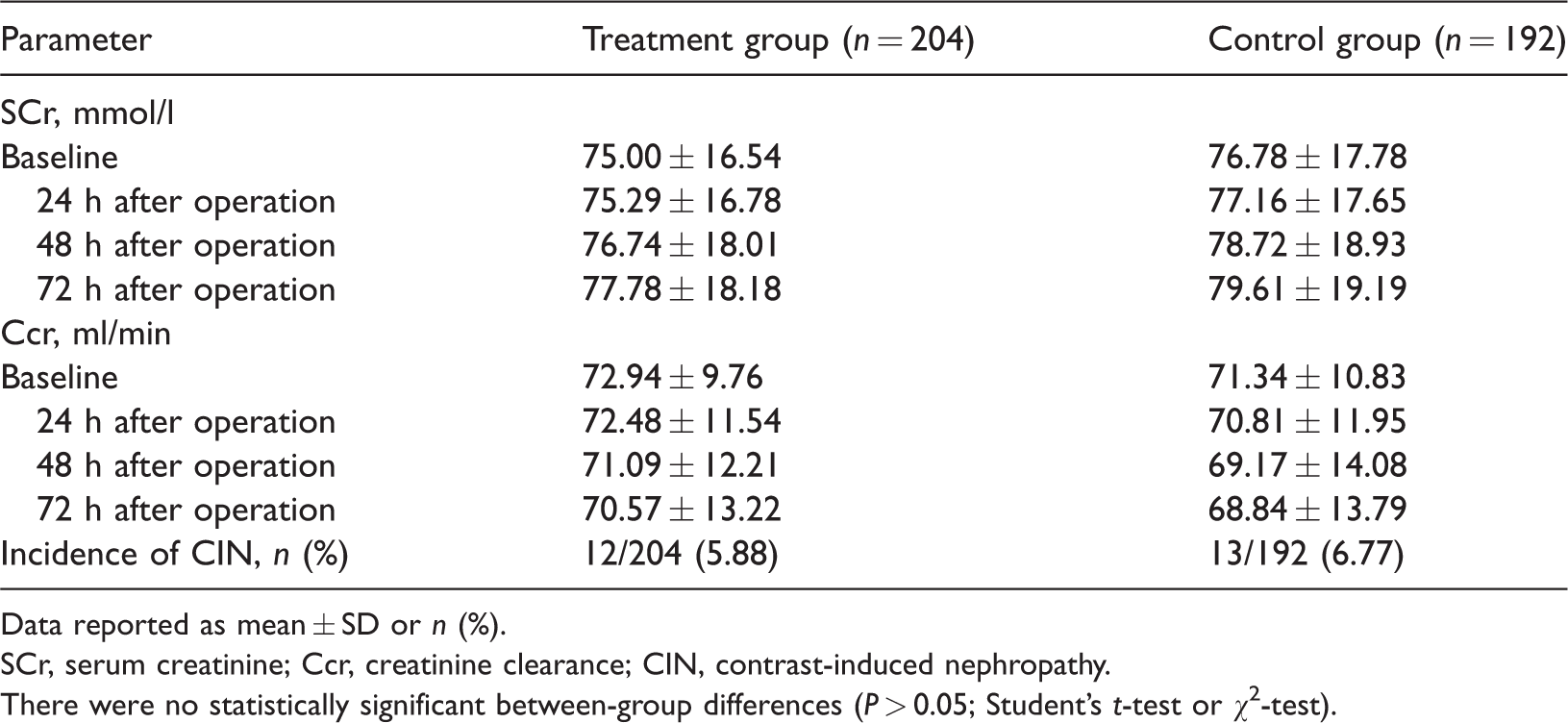
Data reported as mean ± SD or n (%).
SCr, serum creatinine; Ccr, creatinine clearance; CIN, contrast-induced nephropathy.
There were no statistically significant between-group differences (P > 0.05; Student’s t-test or χ2-test).
In the treatment group, 12 out of 204 patients developed CIN following PCI, with an incidence rate of 5.88%, while 13 of 192 patients (6.77%) developed CIN in the control group. There was no statistically significant difference in the incidence of CIN between the two groups (P = 0.43; χ2-test). There were no serious adverse events during this study, such as renal replacement therapy or death.
Discussion
The pathophysiological mechanism of CIN remains uncertain, but renal hypoxia and oxidative stress are known to play important roles in the occurrence of CIN, 17 and age is also a major risk factor. Increasing age is usually accompanied by the occurrence of various chronic diseases that may promote the occurrence of CIN. Diabetes mellitus, for example, plays an important role in CIN development. In patients with diabetes, the application of iodine contrast agent increases the activity of renal tubular transport and the consumption of oxygen, which then leads to renal medulla hypoxia and ROS production. 18 Diabetes can also amplify the above changes, destroying the renal protective mechanism, 18 and make CIN more likely to occur. Therefore, there is a need to attach more importance on preventing CIN in elderly patients with diabetes.
Reduced glutathione combines with oxygen radicals through sulfhydryl groups, transforming oxygen radicals into acidic substances to accelerate their elimination. Thus, reduced glutathione plays a crucial part in maintaining the stability of the internal environment and cell biological function. 19 When levels of endogenous reduced glutathione are decreased in the pathological state, timely supplementation of exogenous reduced glutathione can maintain the integrity of the cell membrane, reduce cell damage and stabilize the endothelial cells of renal tubules, so as to achieve renal protection. 19 Despite this, Jin et al. 20 found that reduced glutathione did not further reduce the incidence of CIN in elderly patients undergoing angiography or PCI.
In the current trial investigating elderly patients with diabetes undergoing PCI, serum creatinine and creatinine clearance were studied in two randomly assigned groups. No statistically significant difference in serum creatinine or creatinine clearance levels was found between patients treated with hydration alone and those treated with hydration combined with reduced glutathione. There was also no statistically significant difference in the incidence rate of CIN between the two groups. Thus, according to currently available data, the combined use of reduced glutathione with hydration does not appear to further reduce the incidence of CIN. It is noteworthy that the present study was conducted on elderly patients with diabetes who underwent coronary intervention, however, further data are required to support the present results.
The results of the present study may be limited by several factors. First, the sample size is relatively small, and secondly, this was a single centre study. Thus, the results may not be generalizable to the wider population. Finally, the non-blinded design of the study leads to a degree of uncertainty in the present data. Therefore, a double-blind, multicentre study with a larger sample size should be conducted to confirm the present results.
In conclusion, the present study suggests that in elderly patients with diabetes receiving PCI, the risk of CIN is not effectively lowered by hydration combined with reduced glutathione versus hydration alone. Further studies are required to confirm these results.
Footnotes
Data accessibility
Original data supporting the results of this study are available from the corresponding author upon request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.