
Abstract
Background:
Coronary angioplasty in advanced age is associated with higher rate of comorbidities and complications. Drug coated balloon only angioplasty (DCBA) has emerged as an alternative to treat small vessel coronary disease (SVCD), of reference vessel diameters <2.8 mm, with shorter duration of dual antiplatelet (DAPT). This is the first study to assess the DCBA efficacy in an elderly population with SVCD.
Methods and results:
We performed a prospective study of 447 patients (334 patients aged <75 and 113 patients aged ⩾75 years old) acquired from the SeQuent Please Small Vessel ‘Paclitaxel-Coated Balloon Only’ registry. In the older age group, more patients have hypertension (89% versus 77%; p = 0.006), renal insufficiency (21% versus 6%; p < 0.001), atrial fibrillation (17% versus 7%; p = 0.001), and calcified lesions (33% versus 20%; p = 0.006). At 30 days, there was one myocardial infarction requiring target lesion revascularization (TLR) in the younger group. No major adverse cardiac event (MACE) was observed in the older group. At 9 months, the MACE rate in the younger group was 4.2% and 6.1% in the older group (p = 0.453), with TLR rates at 3.9% and 3.0% (p = 0.704) respectively. There was no cardiac death observed.
Conclusion:
DBCA in the elderly with SVCD is as safe and effective compared with younger patients despite more complex anatomy and comorbidities.
Background
Developed countries are facing a rapidly aging population and with it an ever increasing health economic burden. The elderly are associated with more degenerative diseases, including coronary artery disease (CAD). Unfortunately, elderly patients are often excluded from clinical trials [Roth et al. 2012]. Nevertheless, coronary angioplasty remains the treatment of choice for symptomatic CAD regardless of the patient’s age [Bryniarski et al. 2004; Chen et al. 2010] and has been proven to be effective and safe for the elderly [Eeckhout et al. 1996; Feliciano et al. 2005]. Furthermore, elderly patients referred for percutaneous coronary interventions (PCIs) are likely to have higher risk profiles, comorbidities and in-hospital complications [Bossi et al. 2006; Sukiennik et al. 2007].
The drug coated balloon (DCB) is indicated for the treatment of coronary in-stent restenosis (ISR) [Scheller et al. 2006, 2008; Windecker et al. 2014]. There has been an increasing body of literature demonstrating the efficacy of using the DCB as a standalone therapy to treat diffuse, small vessel coronary disease (SVCD) [Latib et al. 2012]. Drug coated balloon angioplasty (DCBA) offers several benefits in a higher risk population, as it leaves no permanent foreign bodies in the vessel and does without the ‘caging effect’ brought on by a metallic stent. This in turn may allow the positive remodeling of the treated segment to take place [Kleber et al. 2015]. It also requires shorter duration of dual antiplatelet therapy (DAPT) than angioplasty with drug eluting stents (DESs) [Bonaventura et al. 2011]. Little is known in the use of the DCB in elderly patients.
We report here the safety and efficacy of DCBA in de novo SVCD in patients ⩾75 years old.
Method
We performed a prospective study of 447 consecutive patients acquired from the SeQuent Please Small Vessel ‘Paclitaxel-Coated Balloon only’ Registry, involving multiple centers in eight countries (Singapore, Malaysia, China, Brunei, Iran, France, Germany, Italy) [Zeymer et al. 2013]. All patients underwent PCI with a DCB (SeQuent Please, B. Braun, Melsungen, Germany) in lesions with a small reference diameter (<2.8 mm) and the intention to treat the lesion without additional stenting. Patients were enrolled from January 1, 2011 to December 31, 2012, and then followed up for 9 months. The patients were divided into two groups, aged <75 years old and ⩾75 years old, consisting of 334 and 113 patients, respectively.
Statistical analysis
Categorical variables were evaluated with the Chi-square test, whereas continuous variables were typically compared with the unpaired two-tailed Student’s t-test. In parameters with Gaussian distributions, samples were described using the mean and the standard deviation. Kaplan–Meier survival analyses were performed using the log-rank test. SPSS version 20.0 (IBM, Munich, Germany) was used for all analyses at a significance level of 0.05.
Results
The elderly had more risk factors and comorbidities. The proportions of hypertension, renal impairment, atrial fibrillation and history of prior PCI were significantly higher in patients ⩾75 years of age (Table 1). There was no difference in the rate of hyperlipidemia or history of prior coronary bypass surgery. A total of 76% of patients in this study were referred for PCI in the elective setting, either with stable angina or suspected CAD by prior noninvasive testing. Less than 10% presented with ST-elevation myocardial infarction (STEMI) in both groups.
Patient demographics and presentations.
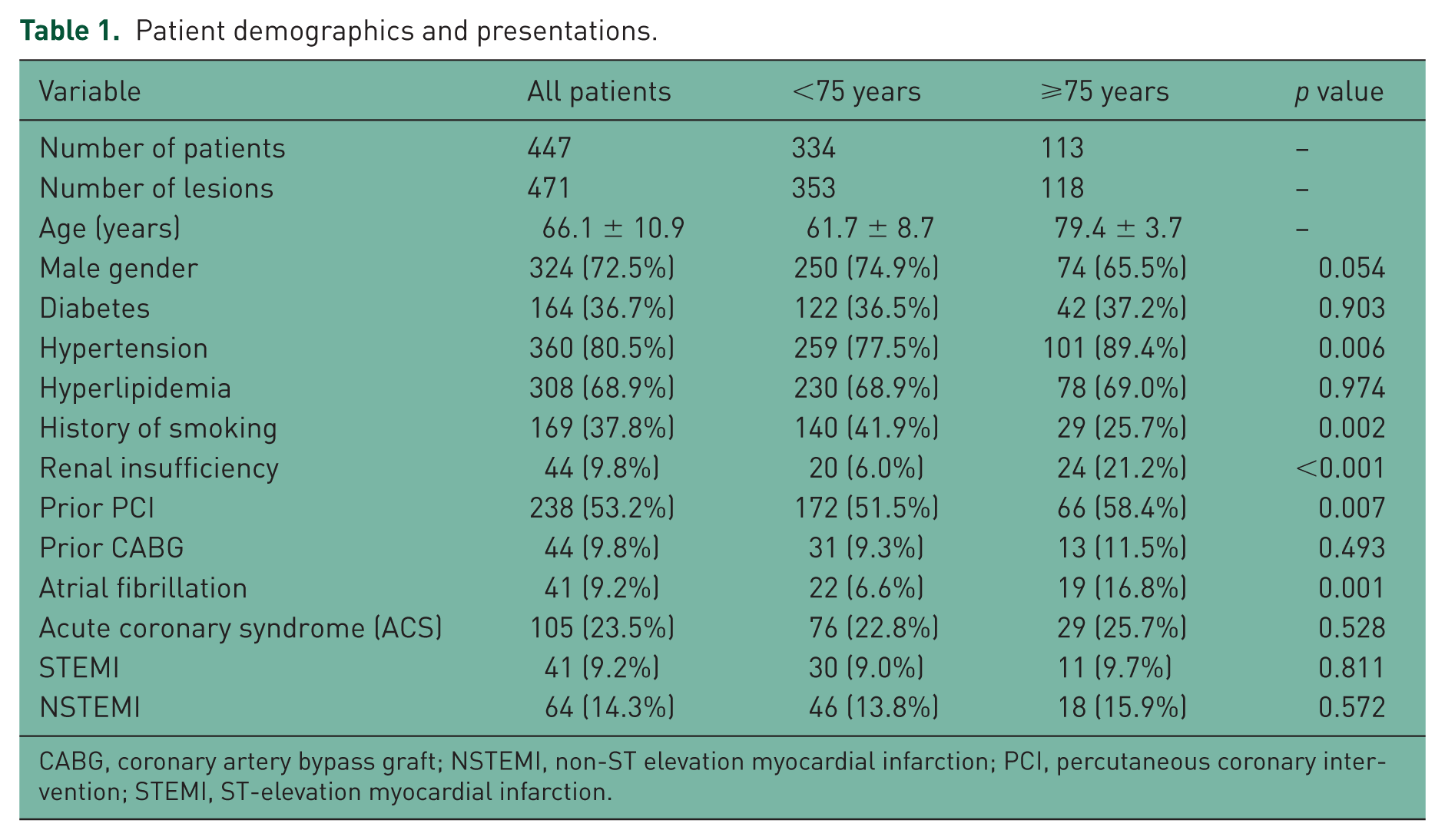
CABG, coronary artery bypass graft; NSTEMI, non-ST elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
The distributions of vessels treated with DCBA were similar in both groups. DCBs were most frequently used in the left anterior descending artery (41%), followed by the left circumflex artery and the right coronary artery. The older group’s coronary vessels had significantly more calcification than those of the younger (33.1% versus 20.7%; p = 0.006) (Table 2).
Lesion characteristics and procedural data in patient populations <75 years and ⩾75 years.

ACC, American College of Cardiology; AHA, American Heart Association; DCB, drug coated balloon; LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery.
There was no significant difference in the proportion of tortuous vessels, American Heart Association (AHA) / American College of Cardiology (ACC) type B2/C lesions, as well as in the reference diameter and length of intervened lesions. The lesion stenosis was numerically higher in the older group compared with the younger group (87.1 ± 9.9% versus 84.8 ± 11.6%; p = 0.056).
A total of 357 and 121 DCBs were used, with procedural success rate at 99.4% and 97.4% in the younger and older groups, respectively. As per the DCB inflation protocol, the mean DCB inflation time was over 45 seconds in both groups. There was no difference in the bailout stenting rate (due to DCB induced major dissections or excessive recoil), which was 7.3% in the younger and 6.7% in the older group (p = 0.826).
Tables 3 and 4 show the types and duration of DAPT given to the subjects during the follow-up period. All patients received aspirin. In addition to that, most patients were given clopidogrel (80.8% and 83.2% in the younger and older groups, respectively) as the second antiplatelet agent. There was significantly more liberal usage of novel antiplatelet agents (prasugrel and ticagrelor) in the <75 years old compared with those ⩾75 years old (12.9% versus 5.3%; p <0.05).
Periprocedural antiplatelet therapy in patient populations <75 years and ⩾75 years.

GP IIb/IIIA, glyocoprotein IIb/IIIa.
Duration of dual antiplatelet therapy during follow up in patient populations <75 years and ⩾75 years.

Despite common recommendation for short-term dual antiplatelet (4 weeks) agents following PCI with DCB [Bonaventura et al. 2011], a small portion of patients received aspirin as the sole antiplatelet therapy, and the proportion was higher in the older group (3.9% versus 7.1%). Most of the patients were given DAPT for 1 month (56.6% in the younger and 69.0% in the older groups). No differences were noted in terms of DAPT duration (Table 4, p = 0.257).
At 30 days, there was 1 case of myocardial infarction (MI) requiring target lesion revascularization (TLR) in the younger group. No major adverse cardiac event (MACE) such as MI, TLR or death was observed in the older group. After 9 months, the MACE rates were 4.2% and 6.1% (p = 0.453) and TLR rates were 3.9% and 3.0% (p = 0.704) in the younger and elderly patients, respectively. There was no additional death reported during the observation period (Table 5).
Clinical outcomes in patient populations <75 years and ⩾75 years.
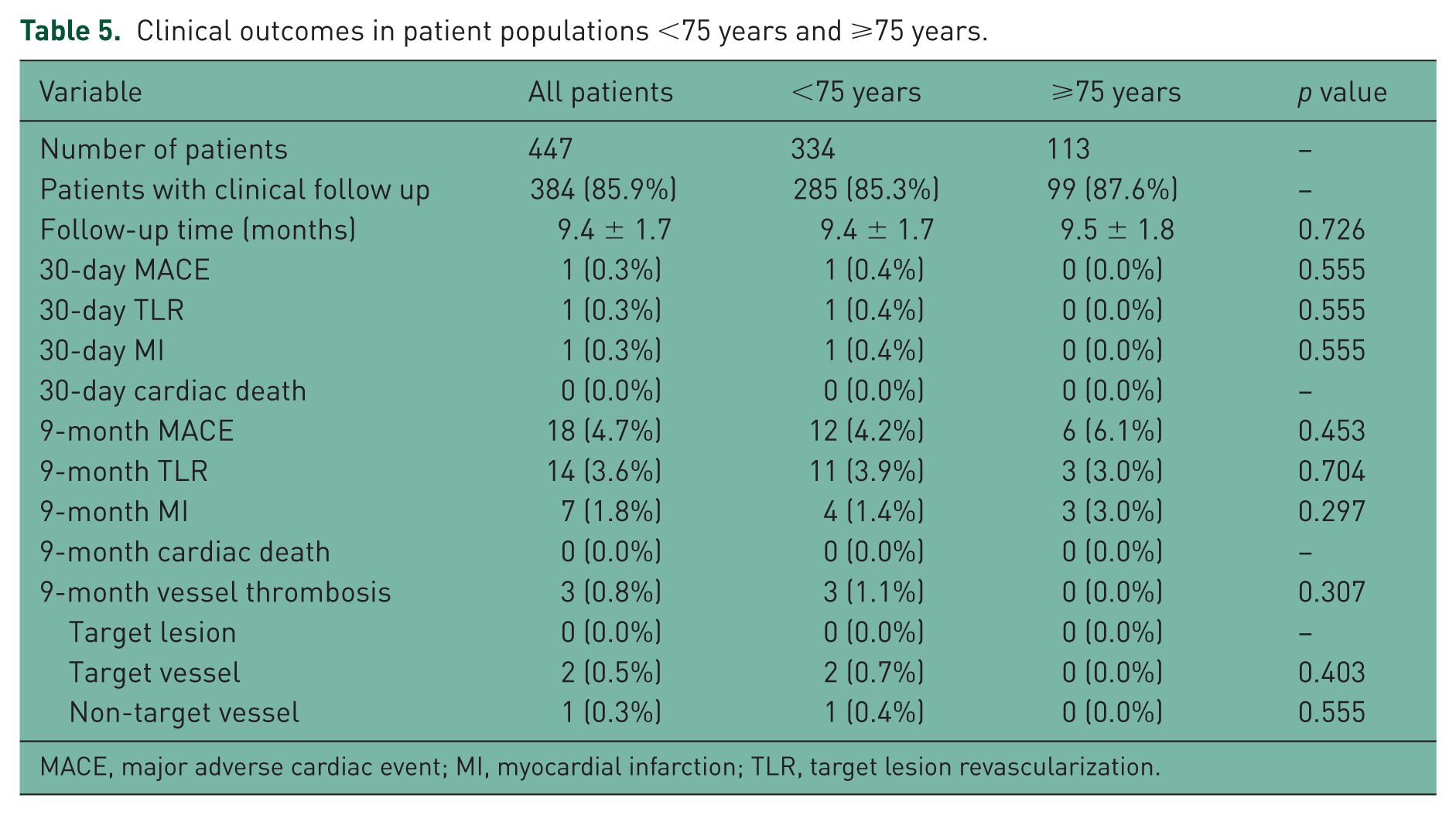
MACE, major adverse cardiac event; MI, myocardial infarction; TLR, target lesion revascularization.
The Kaplan–Meier survival curve (Figure 1) showed no difference in survival from MACE within the two groups during the observation period (log-rank test p = 0.527).

Kaplan–Meier curve of survival from MACE.
Discussion
With its introduction in 2001, the DES has quickly become the gold standard device in the percutaneous treatment of obstructive CAD. Despite its many benefits, DES has limitations, such as late stent thrombosis, impaired endothelial function [Moses et al. 2003] and loss of vasomotor function due to the caging effect from a permanent scaffold. To prevent this phenomenon, patients are given prolonged DAPT up to 12 months following DES implantation. However, this may not be well tolerated by patients with high risk of bleeding, especially in elderly patients with significant comorbidities. Hence there remained a proportion of patients to whom a bare metal stent (BMS) had to be implanted. A promising alternative in this population is the usage of the DCB.
The benefits of the DCB in ISR have been demonstrated in clinical trials and endorsed by European guidelines [Scheller et al. 2006; Maier et al. 2008; Unverdorben et al. 2009; Windecker et al. 2014]. DCBA has recently been used in the treatment of de novo CAD, even though it is still limited to small randomized trials. A meta-analysis study revealed that DCBA showed similar results to standard coronary stenting (mixed BMS and DES) with a risk ratio (RR) for TLR of 1.09 (p = 0.70) and relative risk (RR) for MACE of 0.95 (p = 0.776). Compared with DES angioplasty, the DCBA RR for TLR was 1.53 (p = 0.117) and the RR for MACE was 1.23 (p = 0.750) [Froehlich et al. 2013]. However, the study was limited by heterogeneity amongst the included studies and the different types of DCB used.
DCBA may see the greatest potential when used in treating de novo small coronary lesions. Recent studies comparing DCBA with DES angioplasty showed mixed results. The PICOLETTO trial (first generation DIOR paclitaxel-coated balloon versus paclitaxel eluting stent during PCI of small coronary vessels) failed to show noninferiority of DCB to DES with lower TLR in the DES arm (TAXUS Liberte) (10.3% versus 32.1%; p = 0.043) [Cortese et al. 2010]. It was argued that the failure was due to the technology of the balloon coating which resulted in less paclitaxel delivered to the targeted lesion compared with those in newer second generation DIOR and Paccocath DCBs [Byrne et al. 2011]. In the prospective Bello (Balloon Elution and Late Loss Optimization) study, paclitaxel DCBA was associated with less angiographic late (6 month) loss [0.08 ± 0.38 mm versus 0.29 ± 0.44 mm; p (noninferiority) < 0.001; p (superiority) = 0.001] and similar rates of restenosis (10% versus 14.6%; p = 0.35) and revascularization (4.4% versus 7.6%; p = 0.37) to paclitaxel eluting DES in treating SVCD [Latib et al. 2012].
The prospective PEPCAD I study showed that using DCB only angioplasty to treat SVCD resulted in good 6-month angiographic and 12-month clinical outcomes that persisted up to 36 months. The rate of TLR in patients treated only with DCBA was 4.9% within 12 months, but was significantly higher in those requiring bailout stenting with BMS (28.1%; p < 0.001) [Unverdorben et al. 2013]. The current consensus among the DCB operators is to discourage the routine implantation of a BMS in the DCB-treated segment in the absence of high-grade dissection or recoil [Kleber et al. 2010]. It is important to highlight the low bailout stenting rate of 7.2% in this registry, suggesting a learning curve to move back to the balloon only angioplasty practice.
As a subgroup analysis of the SeQuent Please Small Vessel Paclitaxel-Coated Balloon only Registry, the advantage of the study was that the patients were recruited from multinational populations. To date, this is the first study to assess the DCBA efficacy and safety in elderly population with small coronary vessel lesions. Importantly, the older group in this study had significantly more risk factors and comorbidities, such as diabetes (37.2%), hypertension (89.4%), renal impairment (21.2%) and atrial fibrillation (16.8%). In addition, the patients in this arm had more calcified lesions which contributed to more unfavorable long-term PCI results [Bossi et al. 2006]. In spite of that, procedural success in the elderly group was high (97.5%) with a low bailout stenting rate of 6.7%. The 9-month MACE rate in this cohort of high risk elderly patient was a respectable 6.1%.
Stent implantation in a calcified coronary artery may result in underexpansion and malapposition, leading to a higher MACE rate. One might argue that by performing DCB only angioplasty in the elderly with calcified arteries, the associated complication of suboptimal stent deployment was avoided.
More than half of the patients received DAPT for only 1 month, which is a major advantage of DCBA. Following DES implantation, premature discontinuation of clopidogrel poses a 30-fold increase in the risk of in-stent thrombosis [Iakovou et al. 2005]. As the older patients tend to have more comorbidities such as anaemia, chronic kidney disease or cancer, they become less tolerant to prolonged DAPT duration. In this study, despite a shortened DAPT regime, DCBA was associated with a low 9-month MACE (4.2% versus 6.1%; p = 0.453) and 9-month TLR (3.9% versus 3.0%; p = 0.70) in both the under 75 years old and the over 75 years old respectively.
The DCBA result derived from our DCB study is comparable with that of angioplasty with the everolimus-eluting stent from the SPIRIT Small Vessel Trial, which showed a clinically driven TLR rate of 5.1% after 1 year [Cannon et al. 2012]. The XIMA Trial (Xience or Vision Stents for the Management of Angina in the Elderly), comparing the everolimus-eluting stent and BMS usage in patients >80 years old, revealed a lower 1-year TLR rate in the DES group (2.0% versus 7.0%; p < 0.001) than the BMS group [De Belder et al. 2014]. Nevertheless, the XIMA trial could not be directly compared with this study as it was not dedicated to small vessel coronary lesion.
Limitations
There are several limitations in this study. First, as a subgroup analysis of the SeQuent Please Small Vessel ‘Paclitaxel-Coated Balloon only’ Registry, the findings were for hypothesis generation. Our observational study was designed with consecutive sampling; hence it might lead to selection bias and unmeasured confounders. Second, the duration of follow up might not be long enough to evaluate the long-term outcome of coronary revascularization, although studies showed that procedure-related MACEs mostly occur within 6 months postprocedure. Third, to assess DCBA efficacy and safety in the elderly, the outcome should be compared with modern DES implantation in the same controlled population.
Conclusion
To our knowledge, this is the first report on the use of the DCB in elderly patients with SVCD. The use of DCBA to treat the elderly with SVCD appeared to be safe and effective despite their more complex anatomy and less aggressive antiplatelet regime. The procedure outcome compares favorably with the published data on second generation DES.
Footnotes
Acknowledgements
We thank Denny Herberger (Medical Scientific Affairs, B. Braun Vascular Systems) for his valuable logistic support.
Conflict of interest statement
M.W.W. is an employee of B. Braun Vascular Systems, Berlin, Germany. The other authors declare no conflicts of interest in preparing this article.
Funding
Data acquisition and analysis of this clinical research were funded by B. Braun Melsungen AG.