
Abstract
Objective
To assess the determinants of target lesion revascularization (TLR) after drug-coated balloon (DCB) angioplasty for de novo small coronary artery lesions.
Methods
This retrospective study enrolled consecutive lesions from patients that were in a stable condition and had undergone successful DCB treatment for de novo small coronary artery lesions. The study endpoint was TLR and major adverse cardiac events at 12 months.
Results
A total of 68 patients with 83 lesions were enrolled in the study. Of these, 11 (13.3%) lesions required TLR. Mean ± SD pre-dilatation balloon diameters were similar in the non-TLR (2.33 ± 0.72 mm) and TLR (2.18 ± 0.36 mm) groups. A comparison of the two groups showed that post/pre-lumen area ratio during pre-dilatation (%) by plain old balloon angioplasty (POBA) was significantly and negatively associated with TLR and the optimal cut-off point was 170%. Cox proportional hazard and multivariate regression analyses showed that post/pre-lumen area ratio was the only independent predictor of TLR (hazard ratio 0.9318; 95% confidence interval 0.9001, 0.9645).
Conclusion
Greater pre-dilatation using POBA, assessed as the post/pre-lumen area ratio, may be independently associated with a lower 12-month TLR rate in patients undergoing DCB angioplasty for de novo small coronary lesions.
Introduction
The introduction of drug-eluting stents (DES) has revolutionized the percutaneous coronary intervention (PCI) strategies for de novo lesions by reducing the incidence of restenosis and subsequent target lesion revascularization (TLR).1,2 Despite these improvements, DES implantation has been associated with significant limitations, such as the necessity for dual antiplatelet agent administration.3–6
Drug-coated balloons (DCB) have been used to deliver antiproliferative agents such as paclitaxel to the coronary vessel walls, thereby inhibiting neointimal proliferation after angioplasty.7,8 Theoretically, DCB treatment of de novo lesions omits the need for stents and shortens treatment with dual antiplatelet agents. 9 DCB angioplasty has been shown to be safe and effective for de novo lesions, with low rates of subsequent TLR and major adverse cardiac events (MACE).10–16 Restenosis has been shown to develop, however, in a significant proportion of treated coronary vessels <2.75 mm in diameter,7,8 emphasizing the need to determine middle-term outcomes after DCB treatment for de novo coronary lesions. To improve PCI strategies in patients with de novo small coronary artery lesions, in whom DES implantation has still some limitations, the present study evaluated the potential determinants of restenosis after DCB treatment for these lesions.
Patients and methods
Patient population
This retrospective study enrolled consecutive lesions from patients that were in a stable condition and had undergone successful DCB treatment for de novo small coronary artery lesions under intravascular ultrasound (IVUS) guidance between April 2016 and December 2019 at the Department of Cardiology, Kanazawa Medical University, Uchinada, Japan. The exclusion criteria were as follows: (i) imaging devices were not used during PCI; (ii) patients that were imaged only by optical coherence tomography (OCT)/optical frequency domain imaging (OFDI) devices. TLR was defined as ≥90% stenosis on angiography requiring revascularization and lesions were categorized into two groups: those that did and did not undergo TLR.
The study protocol complied with the Declaration of Helsinki and was approved by the ethics committee of Kanazawa Medical University on 1 May 2020 (no. I498). Informed consent was obtained in the form of an opt-out option on our hospital website and those that rejected enrolment were not included in the study. The personal details of the patients were removed so that they could not be identified in any way during the data analysis. The techniques and equipment used for PCI are continuously changing to keep up with research in this field. However, during the period of this study, there were no major changes or advancements in the techniques and equipment used for PCI. The reporting of this study conforms to STROBE guidelines. 17
PCI procedure
All patients were treated with 100 mg/day aspirin and 75 mg/day clopidogrel or 3.75 mg/day prasugrel at least 5 days before PCI. Before DCB treatment, each lesion was routinely prepared using a semi-compliant balloon, Scoring balloon (Flextome™ Cutting Balloon™; WOLVERINE™ Cutting Balloon; Boston Scientific, Natick, MA, USA) or the non-slipping balloons (Lacrosse NSE®, NSE ALPHA®, NSE ADVANCE®; NIPRO, Osaka, Japan), with a diameter 75–100% of the vessel diameter, as evaluated by IVUS. Balloon inflation pressure was nominal to rated. Coronary calcification was initially assessed angiographically, with results confirmed by IVUS imaging. The extent of calcification on IVUS images was graded as follows: grade 1 (0° to 180°), grade 2 (180° to 270°) or grade 3 (270° to 360°). Rotational atherectomy was applied to the heavily calcified lesions, defined as grades 2 to 3. The burr/vessel diameter ratio ranged from 0.5 to 0.7 and the rotational speed of the burr ranged from 170 000 to 200 000 rpm. After an interval of at least 10 min after lesion preparation, DCB was applied to lesions without severe flow limitation due to type D or E dissection or a severely recoiled lesion. If these complications occurred, bail-out stenting was performed, which led to the patient being excluded from the study.
Drug-coated balloons (SeQuent® Please; B. Braun Melsungen AG, Melsungen, Germany and NIPRO) were inserted into coronary arteries as described previously. 13 DCB diameters ranged from 2.00 mm to 2.75 mm, with the balloon diameter depending on vessel diameter after lesion preparation. The length of each DCB was designed to cover the area covered by the preparation balloon. Balloon inflation pressure was increased gradually to nominal and inflation times ranged from 45 to 60 s. All PCI procedures were self-recorded by the operator and independently reviewed off-line by two senior coronary interventionalists (T.A.T. & Y.K.), with differences resolved by consensus. After PCI, all patients received dual antiplatelet therapy for at least 4 months and single therapy thereafter.
Post/pre-lumen area ratio in plain old balloon angioplasty
As a potential variable representing vessel response to predilatation using plain old balloon angioplasty (POBA), the post/pre-lumen area ratio (%) was defined as the lumen area after the POBA procedure for the culprit lesion divided by the lumen area before assessment of the minimum lumen area by IVUS. Areas were measured online by two well-trained medical engineers (T.N. & S.T.). Intra- and inter-observer variabilities of measurements were <5%.
Follow-up observations
After PCI, ambulatory patients were followed-up for 12 months in the Kanazawa Medical University Hospital, Uchinada, Japan. The study endpoint was defined as the TLR and MACE (a combination of all-cause death and myocardial infarction).
Statistical analyses
All statistical analyses were performed using Microsoft Excel 2016 MSO (16.0.12527.20260) 32 bit (Microsoft Corporation, Santa Rosa, CA, USA). Continuous, normally distributed variables are expressed as mean ± SD and compared using unpaired t-tests. Continuous variables that were not normally distributed are expressed as median and interquartile range (IQR) and compared using Mann–Whitney U-test. Categorical variables are expressed as n (%) and compared using χ2-test. Clinical characteristics of the study participants were analysed on a patient basis. Target lesion, procedure and outcome characteristics were analysed on a lesion basis. The optimal cut-off points of post/pre-POBA lumen area ratio (%) were determined using receiver operating characteristic (ROC) curve analysis and used to predict clinical outcomes.
Univariate and multivariate analyses of factors predicting outcomes were performed using Cox proportional hazards models. The multivariate model for factors predicting time to TLR was evaluated using a stepwise forward elimination procedure for the following categories: nine patient characteristics (age, sex [male], body mass index [BMI] and occurrence of hypertension, dyslipidaemia, diabetes mellitus, smoking, chronic kidney disease and haemodialysis); five target lesion characteristics (target vessel calcification class as detected angiographically or by IVUS, minimum and maximum lumen diameter, minimum lumen area and target lesion plaque volume area); nine procedure characteristics (balloon type, balloon diameter and length, balloon/previous maximum lumen diameter, rotablator use, DCB diameter and length, geographic miss and balloon/DCB diameter ratio); and six outcome characteristics (minimum and maximum lumen diameter after POBA, target lesion area, target lesion plaque volume area, plaque volume reduction ratio and post/pre POBA lumen area ratio [%]). As a final step, in order to investigate the contribution of each variable in all study participants, all variables with P-values < 0.1 in these multivariate analyses and in these four categories were included in the multivariate model.
Prognostic outcomes were evaluated using the Kaplan–Meier method and compared using the log-rank test. All statistical tests were two -sided and a P-value < 0.05 was considered statistically significant.
Results
This retrospective study enrolled 148 consecutive lesions from 109 patients that were in a stable condition and had undergone successful DCB treatment for de novo small coronary artery lesions under IVUS guidance (Figure 1). Of these, 11 lesions in nine patients were excluded because imaging devices were not used during PCI and 54 lesions in 32 patients were excluded because they were imaged only by OCT/OFDI devices. Thus, this study enrolled 83 lesions from 68 patients, all of whom underwent PCI under IVUS guidance. Of the 83 lesions, 11 (13.3%) required TLR, whereas 72 (86.7%) did not. No cardiac deaths or other cardiac events were observed.
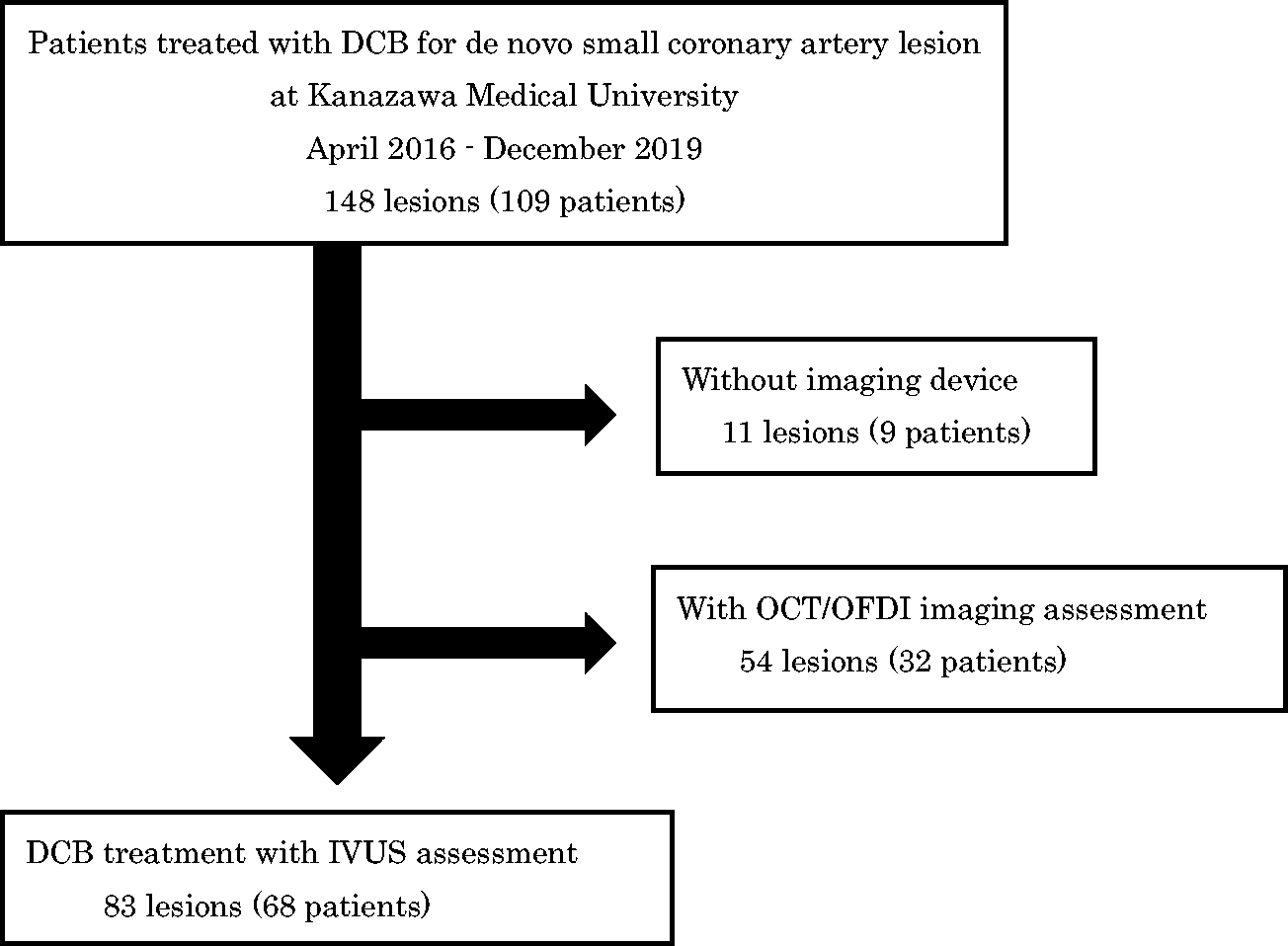
Study flow chart for a retrospective study that enrolled 148 consecutive lesions from 109 patients that were in a stable condition and had undergone successful drug-coated balloon (DCB) treatment for de novo small coronary artery lesions under intravascular ultrasound (IVUS) guidance. OCT, optical coherence tomography; OFDI, optical frequency domain imaging.
The baseline characteristics of the patients and lesions are summarized in Table 1. In the total cohort, the mean ± SD patient age was 68.6 ± 10.6 years and 73.5% (50 of 68 patients) were male. Of the 68 patients, 55 patients had hypertension (80.9%), 48 had dyslipidaemia (70.6%), 30 had diabetes mellitus (44.1%), 13 had chronic kidney disease (19.1%), nine were on haemodialysis (13.2%) and 23 had a smoking habit (33.8%). Significant differences existed in sex, diabetes mellitus and culprit lesion distribution between the TLR and non-TLR groups. The most prevalent target vessel was the left anterior descending artery (43 of 83 lesions, 51.8%), followed by the left circumflex artery (26 of 72 lesions, 31.3%) and the right coronary artery (14 of 83 lesions, 16.9%). As for lesion calcification, the TLR group showed significantly greater prevalence of angiographically-detected calcification compared with the non-TLR group (eight of 11 lesions [72.7%] versus 25 of 72 lesions [34.7%], respectively; P = 0.016). However, no significant difference was observed in the prevalence of IVUS-detected calcification between the two groups.
Baseline clinical, demographic and lesion characteristics of patients (n = 109) that were in a stable condition and had undergone successful drug-coated balloon treatment for de novo small coronary artery lesions under intravascular ultrasound (IVUS) guidance.

Data presented as mean ± SD or n of patients/lesions (%).
aBetween-group comparisons undertaken using unpaired t-test for continuous, normally distributed variables and χ2-test for categorical variables; NS, no significant between-group difference (P ≥ 0.05).
TLR, target lesion revascularization; STEMI, ST elevation myocardial infarction; LVEF, left ventricular ejection fraction; LMT, left main trunk; RCA, right coronary artery; LAD, left anterior descending artery; LCx, left circumflex artery.
A comparison of the procedural characteristics in the two groups showed that the trans-radial approach was significantly more frequently used in the non-TLR group compared with the TLR group (P < 0.001) (Table 2). Mean ± SD balloon diameters used for pre-dilatation were similar in the non-TLR (2.33 ± 0.72 mm) and TLR (2.18 ± 0.36 mm) groups. The balloon (nominal size) to artery diameter ratio evaluated by IVUS (B/A ratio) during pre-dilatation using POBA was significantly higher in the non-TLR group than in the TLR group (1.38 ± 0.2 versus 1.05 ± 0.22, P < 0.001), but there were no significant differences in DCB diameter, DCB total length or geographical mismatch rate between the two groups. Scoring balloons, defined as cutting (Flextome™ Cutting Balloon™; WOLVERINE™ Cutting Balloon; Boston Scientific) and non-slipping (Lacrosse NSE®, NSE ALPHA®, NSE ADVANCE®; NIPRO) balloons, were used in 58 (69.9%) of the 83 lesions.
Characteristics of the procedure undertaken in 83 lesions in patients (n = 109) that were in a stable condition and had undergone successful drug-coated balloon treatment for de novo small coronary artery lesions under intravascular ultrasound guidance.

Data presented as mean ± SD or n of lesions (%).
aBetween-group comparisons undertaken using unpaired t-test for continuous, normally distributed variables and χ2-test for categorical variables; NS, no significant between-group difference (P ≥ 0.05).
bExistence of a difference in balloon length between plain old balloon angioplasty (POBA) and drug-coated balloon (DCB).
TLR, target lesion revascularization; B/A ratio, balloon-to-artery (maximum lumen diameter of pre-dilatation using POBA) ratio.
Minimum vessel diameters, evaluated using intracoronary isosorbide injection, before (1.57 ± 0.16 mm versus 1.78 ± 0.47 mm) and after (2.07 ± 0.27 mm versus 2.20 ± 0.58 mm) POBA, did not differ significantly between the non-TLR and TLR groups (Table 3). Maximum vessel diameter before POBA was significantly lower in the non-TLR group than in the TLR group compared with the non-TLR group (1.70 ± 0.21 mm versus 2.16 ± 0.52 mm, P = 0.015), but this difference disappeared after POBA (2.41 ± 0.32 mm versus 2.51 ± 0.62 mm, respectively). Although lumen area (2.07 ± 0.42 mm2 versus 3.25 ± 1.67 mm2, P = 0.040) and percentage plaque area (76.0 ± 6.98% versus 64.37 ± 4.60%, P = 0.030) differed significantly between the non-TLR and TLR groups before POBA, neither lumen area nor percentage plaque area differed significantly between these two groups after POBA. To assess the net effects of POBA dilatation, changes of lumen area and plaque reduction were compared. Both post/pre-POBA lumen area ratio (200.8 ± 31.8 versus 138.8 ± 23.0, P < 0.001) and lumen plaque reduction (30.1 ± 14.7 versus 19.6 ± 13.7, P = 0.030) were significantly greater in the non-TLR compared with the TLR group.
Lesion characteristics and procedure outcomes in 83 lesions in patients (n = 109) that were in a stable condition and had undergone successful drug-coated balloon treatment for de novo small coronary artery lesions under intravascular ultrasound guidance.

Data presented as mean ± SD or n of lesions (%).
aBetween-group comparisons undertaken using unpaired t-test for continuous, normally distributed variables and χ2-test for categorical variables; NS, no significant between-group difference (P ≥ 0.05).
bValues were measured at the minimum lumen area site.
cDissection type (The National Heart, Lung, and Blood Institute).
dPost/pre-lumen area: post-POBA lumen area/pre-POBA lumen area.
TLR, target lesion revascularization; POBA, plain old balloon angioplasty.
A ROC curve analysis was performed to determine the optimal post/pre-POBA lumen area ratio (%) cut-off point predictive of the need for TLR during follow-up. This analysis showed that a ratio of 170% was optimal, with a sensitivity of 1.000 and a false positive rate of 0.028 (see supplementary materials, Figure 1). Analyses of lesions with low (<170%) and high (≥170%) post/pre-POBA lumen area ratios (%) showed that the prevalence of TLR was significantly greater in the low than in the high ratio (%) group (11 versus 0; log-rank test χ2: 81.72, P < 0.0001) (Figure 2).
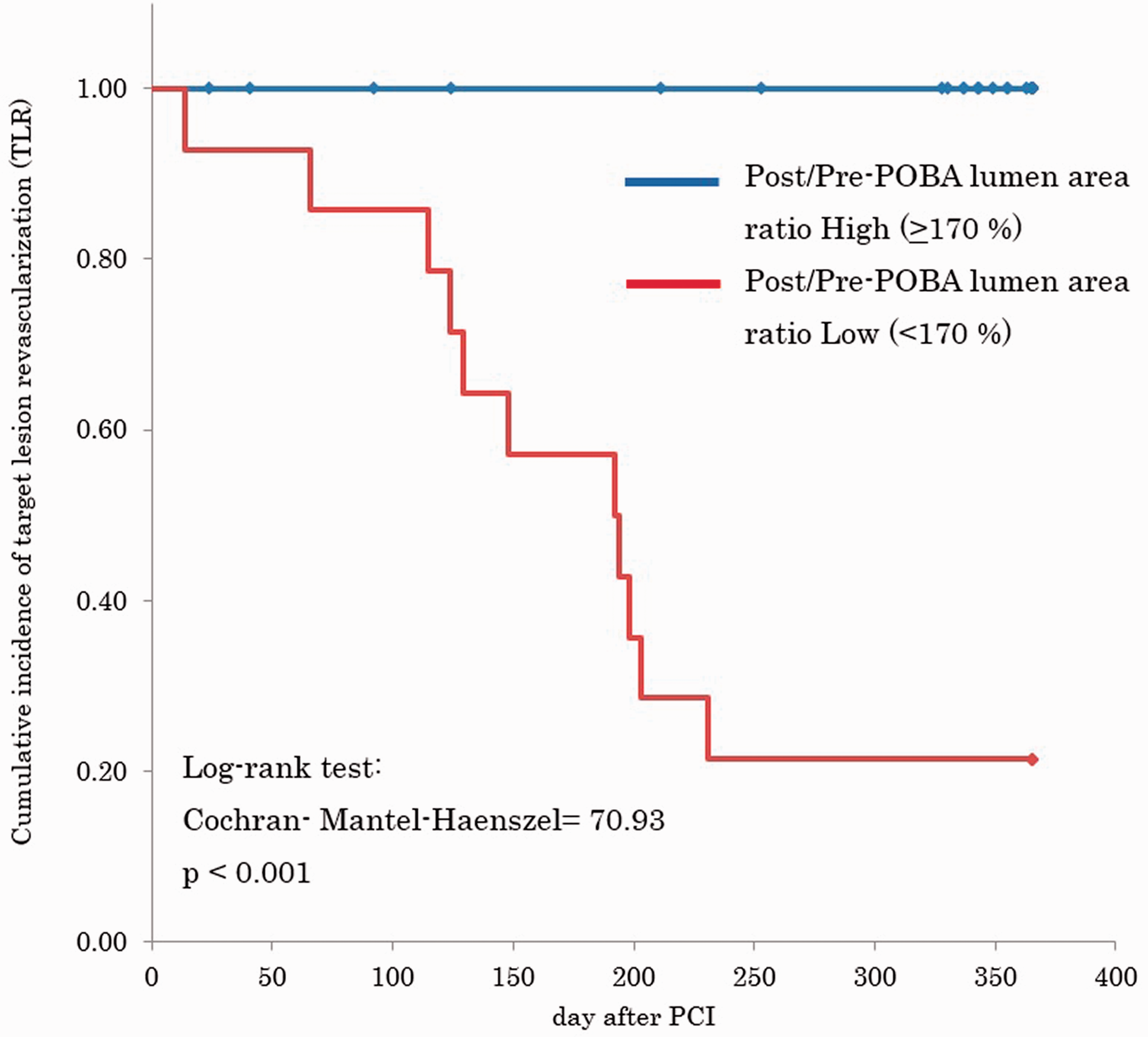
Cumulative Kaplan–Meier estimates of free from the target lesion revascularization after drug-coated balloon treatment for de novo lesions in 109 patients that were in a stable. PCI, percutaneous coronary intervention; POBA, plain old balloon angioplasty. Log-rank test: Cochran-Mantel-Haenszel = 70.93, P < 0.001. The colour version of this figure is available at: http://imr.sagepub.com.
Univariate analysis showed that male sex the among patient characteristics, calcification (angiographically-detected), minimum and maximum lumen diameter, and minimum lumen area before POBA among the target lesion characteristics, rotablator use and balloon/pre-dilatation maximum lumen diameter ratio among the procedures, and plaque volume reduction ratio, post/pre-POBA lumen area ratio (%) and occurrence of dissection among the outcome characteristics were significantly associated with TLR (P < 0.05 for all) (Table 4). Subsequent multivariate regression analysis incorporating variables with significant relationships in the univariate analyses showed that minimum lumen diameter and minimum lumen area among the target lesion characteristics, balloon/pre-dilatation maximum lumen diameter ratio among the procedure characteristics and post/pre-POBA lumen area ratio among the outcome characteristics were significantly associated with TLR (P < 0.05 for all). When all of variables with P-values <0.1 in these subgroups in the multivariate analyses were incorporated into multivariate analysis, only post/pre-POBA lumen area ratio showed an independent association with TLR (hazard ratio 0.9318; 95% confidence interval 0.9001, 0.9645; P < 0.001).
Univariate and multivariate analysis of target lesion revascularization (TLR) in 83 lesions in patients (n = 109) that were in a stable condition and had undergone successful drug-coated balloon treatment for de novo small coronary artery lesions under intravascular ultrasound guidance.
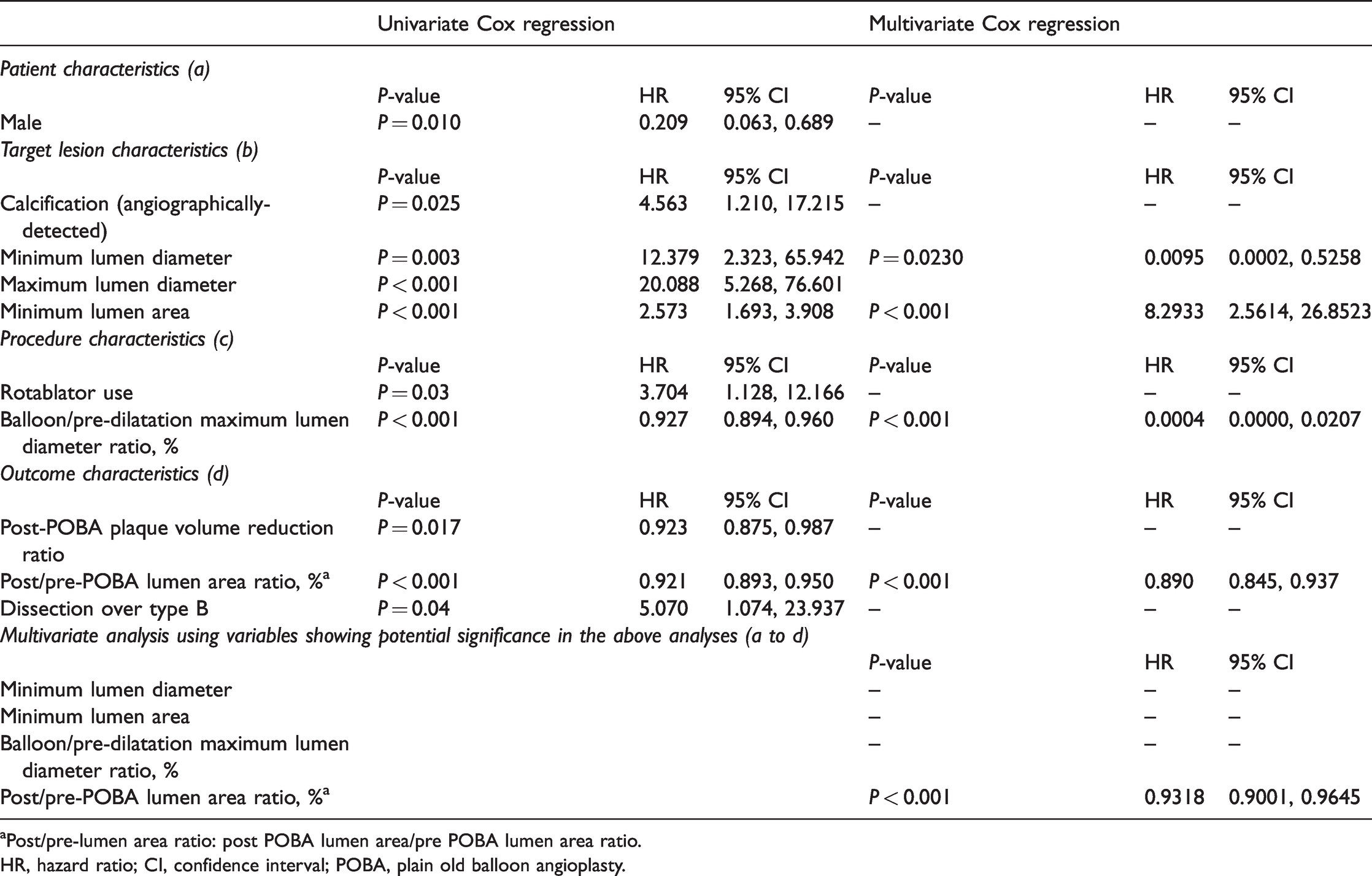
aPost/pre-lumen area ratio: post POBA lumen area/pre POBA lumen area ratio.
HR, hazard ratio; CI, confidence interval; POBA, plain old balloon angioplasty.
Discussion
Drug-coated balloons were developed to overcome neointimal hyperplasia and were first tested in the treatment of in-stent restenosis, showing excellent results that were maintained for several years. 18 DCBs were also expected to show favourable results in the treatment of de novo lesions, with an open label randomized study suggesting their non-inferiority when compared with DES. 15 Although DCBs were reported to show clinical efficacy,19,20 less is known about their effectiveness in small vessels, in which the encumbrance of a stent may limit their potential. The present study assessed factors associated with clinical outcomes after DCB treatment, including patient characteristics, target lesion characteristics and PCI procedure-related parameters. This current study found that a post/pre-lumen area ratio during pre-dilatation using POBA < 170% was an independent predictor of 12-month TLR after DCB treatment for de novo small coronary artery lesions. To the best of our knowledge, this current study is the first to show that vessel response to POBA prior to DCB may be an independent prognostic predictor of a need for TLR within 12 months.
The prevalence of MACE (including TLR) in the present study (13.3%) was slightly higher than in previous studies performed in Western (7.5%) 15 and Japanese populations (5.7%). 21 The higher prevalence in the present study may have resulted from the higher prevalence of lesion calcification, a lesion-specific predictor of poor prognosis after PCI. 22 Although BMI was lower in the current study participants than in Western populations, other patient characteristics, such as age, sex distribution and prevalence of coronary risk factors, were similar, indicating that the current study population was representative of patients that undergo PCI in current clinical settings. 23
Compared with DES, the advantages of DCB treatment are greater in patients with planned non-cardiac surgery or a high bleeding risk, thus avoiding the need for long-term dual antiplatelet therapy. 24 Stent-less PCI using DCB may also have advantages when DES deployment is difficult, including in small-diameter or tortuous lesions, and in patients with a metal allergy.15,25 However, similar to the POBA procedure, DCB may be associated with coronary dissection after balloon dilatation.13,14 The criteria for bail-out stenting during the DCB procedure have not been established, unlike type D to F in the National Heart, Lung, and Blood Institute criteria (the dissection with flow limitation) for the POBA procedure. 26
Although angiographic results, usually those of quantitative coronary angiography, have been reported before and after DCB procedures, this analysis is possible only after the completion of PCI procedures. Thus, these angiographic findings cannot be applied to PCI procedures in real time. Based on these considerations, the present study assessed potential predictors of outcome after the DCB procedure, including clinical, angiographic and IVUS-based variables simultaneously measured during PCI sessions. Although OCT/OFDI can provide more precise information about vessel dimensions and wall characteristics than IVUS, the current study did not include patients assessed by these new devices because of their limited availability.
Several hypotheses may explain the principal finding of the present study, that initial vessel response to POBA defined as a post/pre-lumen area ratio ≥ 170% was significantly and independently associated with favourable 12-month outcomes after DCB. First, a larger gain in vessel area may be associated with reduced late loss. Greater vessel dilatation in response to POBA indicates that these vessel walls have high distensibility with paclitaxel eluted from the balloon, which may be more efficient in inhibiting subsequent smooth muscle cell proliferation after balloon injury. Secondly, the percentage plaque area before dilatation was significantly greater in the non-TLR group than in the TLR group, but this difference became insignificant after the POBA procedure, suggesting a between-group difference in plaque response to POBA. This may be supported by the findings that plaque volume and its reduction (both absolute and relative to pre-POBA dilatation) were not associated with clinical outcomes. Univariate analyses also found that the balloon/pre-maximum lumen diameter and plaque volume reduction ratio were significantly associated with clinical outcomes, but that these factors were no longer significant on multivariate analysis. Future studies with larger sized samples are needed to evaluate the reasons underlying these differences among the examined variables.
In contrast to DES, which can diminish vessel recoil by radial force of stent strut, DCB treatment is influenced by recoil to a greater extent.13,14 To date, however, an efficient method of avoiding recoil has not been established. Even under this condition, acute gain can be considered as an important predictor of restenosis. Theoretically, vessel diameter, lesion morphology and changes in these parameters caused by DCB treatment may influence vessel recoil and outcomes. The present study found that greater post/pre-lumen area ratio in pre-dilatation using POBA was significantly and independently associated with a reduced need for TLR. In addition, the lack of an independent association between the presence of calcification and clinical outcomes suggests that response to pre-dilatation using POBA can represent the ‘total distensibility’ of the coronary artery, a novel indicator easily measured during the PCI procedure in real time. Additional studies are needed to assess the influence of tissue characteristics such as calcification or lipid core, and dissection caused by balloon dilatation on clinical outcomes.
The present study had several limitations. First, this was a small observational analysis from a single centre with a retrospective two-arm design. Unrecognized confounding factors may have influenced the results. Secondly, because this was a nonrandomized, retrospective observational study, the possibility of patient selection bias could not be excluded. Thirdly, a significant part of the treatment protocol, including the PCI procedure, was operator-dependent, which may have inadvertently influenced the study results. Fourthly, tissue morphology on intravascular imaging was not compared, thus preventing assessment of the associations between tissue characteristics and clinical outcomes. Fifthly, due to the limited number of enrolled patients, it is possible that false positive/negative associations with TLR existed. However, multivariate Cox analysis without variable selection did not detect additional variables with potential significance (data not shown). Studies in larger patient populations are needed to definitively determine the effect of DCB treatment on de novo lesions.
In conclusion, a greater degree of pre-dilatation using POBA might be an independent prognostic marker of a lower 12-month TLR rate in patients undergoing DCB treatment for de novo small coronary artery lesions.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221113779 - Supplemental material for Response to pre-dilatation with POBA can predict target lesion revascularization after DCB angioplasty for de novo small coronary artery lesions
Supplemental material, sj-pdf-1-imr-10.1177_03000605221113779 for Response to pre-dilatation with POBA can predict target lesion revascularization after DCB angioplasty for de novo small coronary artery lesions by Taka-aki Takamura, Yasuyuki Kawai, Satori Akita, Minako Oda, Hironobu Akao, Tohru Nakagawa, Shunsuke Takama, Taketsugu Tsuchiya, Michihiko Kitayama and Kouji Kajinami in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605221113779 - Supplemental material for Response to pre-dilatation with POBA can predict target lesion revascularization after DCB angioplasty for de novo small coronary artery lesions
Supplemental material, sj-pdf-2-imr-10.1177_03000605221113779 for Response to pre-dilatation with POBA can predict target lesion revascularization after DCB angioplasty for de novo small coronary artery lesions by Taka-aki Takamura, Yasuyuki Kawai, Satori Akita, Minako Oda, Hironobu Akao, Tohru Nakagawa, Shunsuke Takama, Taketsugu Tsuchiya, Michihiko Kitayama and Kouji Kajinami in Journal of International Medical Research
Footnotes
Author contributions
T.A.T.: overall study design and planning, data collection and analysis, preparation of the draft manuscript; Y.K.: advice study plan and data interpretation; S.A., M.O., H.A., T.T. and M.K.: discussions on PCI strategies and management of PCI procedures; T.N. and S.T.: intravascular image analysis; K.K.: final data analysis and manuscript preparation.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported partly by a grant from Fukuda Foundation for Medical Technology to T.A.T.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.