
Abstract
Objectives:
Coronary artery diseases are regarded as the main cause of mortality in most countries. The present study aims at evaluating variations and studying its complications in Iranian patients within past 20 years.
Methods:
This cross-sectional analytical–descriptive study retrospectively evaluated the files of 600 patients with acute myocardial infarction during a 20-year period. Basic data and laboratory information, chemotherapies and intervention treatments of patients were registered in special forms and compared regarding the mentioned time intervals.
Results:
There were 440 (73.3%) male and 160 (26.7%) female patients and mean age of the patients was 60.03 ± 11.61 years. Mean duration of hospitalization (p < 0.001) and prevalence of smoking (p < 0.001) had significantly decreased in the past two decades. There was no meaningful difference when considering mortality rate (p = 0.533) and cardiac insufficiency (p = 0.403).
Conclusion:
The results indicate prominent improvement in the management process of patients suffering from acute myocardial infarction within the past 20 years.
Introduction
Mortality rate of acute myocardial infarction has decreased from 30–35% during the 1960s to <15% at present in the developed countries [Pant et al. 2011]. The significant decrease in mortality rate of coronary artery diseases can be attributed to two factors: (1) decreased prevalence of some risk factors including hypercholesterolemia, smoking, and hypertension in these countries within the past two decades; and (2) increased evidence-based treatments such as angiotensin-converting enzyme controllers, statins, angioplasty, stent placement, and especially the application of thrombolytics for the routine treatment of coronary artery disease and excluding some other methods such as lidocaine infusion due to the probability of increasing mortality rate of the disease [Alkins et al. 2012; Davidson et al. 2012; Ragnarsson et al. 2012]. The first cause received 50–54% in studies conducted before 1990 and 44% in recent studies [McManus et al. 2011]. In studies conducted in countries adjacent to the Persian Gulf, a progression similar to that of the developed countries but to a lesser degree has been observed [Hatmi et al. 2010]. Through economic development of these countries, lifestyle and dispersion of atherosclerosis risk factors have become closer to the pattern in the western countries and more modern treatment, excluding primary angioplasty, has been used increasingly leading to a significant decrease in the mortality rate of acute myocardial infarction [Teixeira et al. 2010]. In Iran, cardiovascular diseases are also regarded as the most common mortality cause. According to some reports, lifestyle change is the main factor in this regard [Moreyra et al. 2010]. However, there are no published reports about changing treatment patterns or their fatality rate during recent decades. Considering the above-mentioned cases, we decided to evaluate the dispersion of risk factors, in-hospital complications, mortality rated of acute myocardial infarction, and changes in treatment patterns based on new guidelines during three separate time intervals: main use of chemotherapy without reperfusion therapy during 1993–1999; onset of treatment using thrombolytic factors in our center during 1999–2003; and the addition of angioplasty facilities to the previously available treatments during 2003–2012.
Materials and methods
Subjects
This multicenter cross-sectional analytical–descriptive study retrospectively evaluated files from 600 patients with acute myocardial infarction admitted to CCU wards in Iran during a 20-year period from 1993–2012. Files were collected using a cluster sampling method. Considering main variations in treatment patterns including the introduction of thrombolytic therapy in 1999 and angioplasty in 2003, the mentioned time interval has been divided into three periods: 1993–1999, 1999–2003 and 2003–2012. These three groups were matched with regards to age, gender, and risk factors. Files from 200 patients in each period hospitalized with a diagnosis of acute myocardial infarction with ST elevation during the first 24 hours after manifestation of symptoms in CCU ward were randomly selected and studied at each time interval.
Exclusion criteria
Patients with a history of previous infarction, those hospitalized 24 hours after manifestation of the symptoms, and cases with incomplete files were excluded from the study.
Methods
Basic data and laboratory information, chemotherapies and intervention treatments of these three groups including age, gender, duration of hospitalization, history of risk factors including diabetes mellitus (fasting blood glucose ≥126 mg/dl), hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg), hypercholesterolemia (cholesterol level >200 mg/dl or treatment with antihyperlipidemia drugs), and smoking, as well as familial history, myocardial infarction location, in-hospital complications, medicines consumed during hospitalization, echocardiography findings, angiography, angioplasty, and mortality rate were registered in special forms and compared over the mentioned time intervals. Cardiac insufficiency or heart failure were defined as symptoms including pulmonary edema, rales in lung auscultation, neck vein distension, lower limb edema, or left ventricular ejection fraction (LVEF) ≤45%. Mitral regurgitation was defined as blood regurgitation in echocardiography. Right ventricular infarction was defined as ST elevation in inferior leads and V4R right pericardial lead. LVEF was measured on admission by a single observer.
Statistical analysis
The data was stated as mean ± standard deviation, frequency, and percentage, and SPSS-16 statistical software was used to statistically analyze the data. Quantitative variables were compared using the Student’s t-test (independent samples) or one-way analysis of variance (ANOVA) and contingency tables. Chi-squared test or Fisher’s exact test was used to compare categorical variables. The results were regarded as statistically significant if p ≤ 0.05 in all understudy cases.
Results
Out of 870 studied files, 600 patients with primary diagnosis of acute myocardial infarction hospitalized 24 hours after onset of the symptoms at a CCU ward during the mentioned time intervals entered the study. The mean age of the patients was 60.03 ± 11.61 years and mean duration of hospitalization was 8.93 ± 5.38 days (1–33 days). The population consisted of 73.3% male patients and the mean ejection fraction of the left ventricle was 42.63 ± 10.13% (20–60%) in echocardiography of the studied patients. There was a history of diabetes mellitus in 94 (15.7%), smoking in 261 (43.5%), hypertension in 236 (39.3%), high blood lipid levels in 68 (11.3%), and positive familial history in 50 cases (8.3%). Regarding the site of infarction, there were 369 (61.5%) cases with anterior, 199 (33.2%) cases with inferior or inferior–lateral or posterior–inferior, and 32 (5.3%) cases with posterior–right ventricle infarction. Basic characteristics of the patients in the three mentioned groups have been compared in Table 1. With regard to treatments, aspirin was used in 527 (87.8%), heparin in 554 (92.3%), beta blockers in 414 (69%), angiotensin-converting enzyme inhibitors (ACEIs) in 363 (60.5%), calcium channel blockers in 138 (23%), lidocaine in 175 (29.2%), amiodarone in 16 (2.7%), streptokinase in 81 (13.5%), diuretics in 220 (36.7%), digoxin in 117 (19.5%), and nitrates in 579 (96.5%) of the cases. Angioplasty was used in only 20 (3.3%) cases. The treatment pattern of the patients in three mentioned time intervals has been compared in Table 2. In all of the patients, cardiac insufficiency was seen in 127 (21.2%), fibrillation or ventricular tachycardia during the first 2 days of hospitalization in 58 (9.7%), fibrillation or ventricular tachycardia after 2 days of hospitalization in 22 (3.7%), mitral valve insufficiency in 11 (1.8%), ventricular septal defect (VSD) in 15 (2.5%), pericarditis in 25 (4.2%), and cardiogenic shock in 29 (4.8%) cases. The total mortality rate of the studied patients’ was 111 (18.5%). Mortality and morbidity rate of the patients in three mentioned time intervals have been compared in Table 3.
Separate comparison of general factors among the three groups of patients.

Group 1: 1993–1999; Group 2: 1999–2003; Group 3: 2003–2012.
Separate comparison of applied treatment methods among the three groups of patients.

Group 1: 1993–1999; Group 2: 1999–2003; Group 3: 2003–2012.
ACEI, angiotensin-converting enzyme inhibitor.
Separate comparison of myocardial infarction complications among the three groups of patients.
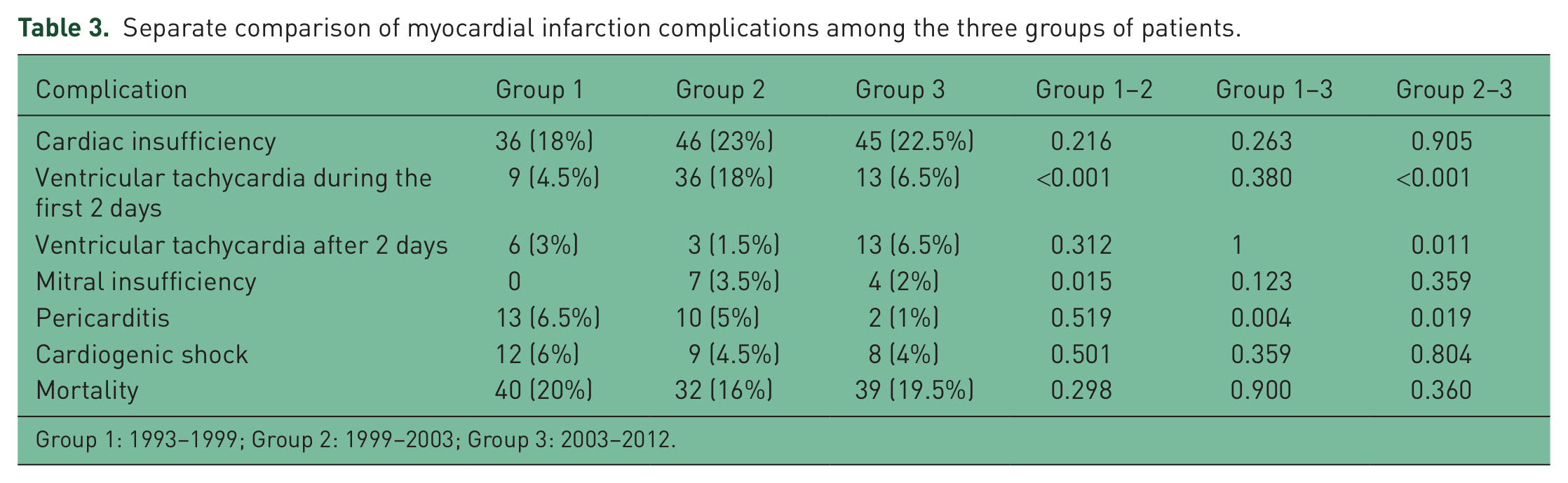
Group 1: 1993–1999; Group 2: 1999–2003; Group 3: 2003–2012.
Discussion
Regarding the prevalence of risk factors in myocardial infarction within the past 20 years, our study indicates a decrease in smoking and an increase in hypercholesterolemia prevalence, although chronological evaluation of the groups did not reflect any meaningful difference with respect to diabetes mellitus, positive family history or patients’ gender. Hypertension had increased significantly during the past two decades in comparison with the first group. As hypertension was registered based on a description of the patients’ conditions, its increase cannot be merely attributed to an increase in prevalence. Enhancing people’s knowledge level, improvement of public health, and availability of more therapeutic centers during recent years might have been helpful in detecting more cases. Studies conducted in the developed countries refer to a decrease in hypercholesterolemia, smoking, and hypertension during the past two decades [Bauer et al. 2011; Dresslerova and Vojacek, 2010; Shamshad et al. 2010]. It should be mentioned that the decrease was associated with a high prevalence of obesity and diabetes [Mihalcea and Pandele, 2009]. The increase in hypercholesterolemia over the past 20 years might be attributed to negative lifestyle changes such as physical activity and nutrition [Ma et al. 2009; Volpp et al. 2009]. Aspirin and heparin were used in almost all cases in the last two groups, consumption of beta blockers has increased by a factor of two during this period, and ACEIs have been prescribed in >90% of the patients near the end of the study. Both cases correspond with modern guidelines [Goldberg et al. 2009]. Duration of hospitalization has decreased meaningfully within this period. This is also in correspondence with recent treatment strategies emphasizing early mobility of the patients [Bezdah et al. 2007]. During the first study period, although streptokinase was at least available within the past 1.5–2 years at the CCU ward, it was used in only two cases (1%). It was only used in 26.5% of cases during the third period which includes the highest rate of consumption. In other words, prescription of thrombolytic factors have both been started with delay and used in lower amounts in our center. According to what has been stated about reperfusion-independent treatment groups, delay in using reperfusion-dependent treatments cannot be justified merely by relying on any delay in knowledge and information of the therapists regarding modern treatment methods [Gasior et al. 2007]. Secondary forms of reperfusion-based treatments (e.g. angioplasty) have been used even less than thrombolytic therapy, being conducted in only 1.5% of cases during the second period and 8.5% of the patients within the first 24 hours after hospitalization during the third period. Certainly, the unsuitable setting of emergency conditions in Iran can be considered as being the main reason for this. The sets are mostly used for those patients placed in list of angiography or angioplasty for several months. There is no unoccupied angiography ward to transfer the patients whose the maximum permitted delay is 90 minutes from hospital door to open their vessel using a balloon [Perez-Vizcayno et al. 2007]. As the superiority of angioplasty over thrombolytic therapy has been completely proven in different studies [Christenson et al. 2007], the angioplasty to thrombolytic therapy ratio is increasing in the developed countries. Considering that the mortality rate of acute myocardial infarction has decreased from 30–35% to less than 15% in the developed countries [Holay et al. 2007], some points should be noted to justify the finding which is in contrast with our presuppose.
(1) Since there are a limited number of CCU beds, high-risk patients with a naturally high rate of morbidity and mortality are often transferred to the CCU ward. Therefore, the mentioned theory cannot justify the lack of any significant change of prognosis of the patients within the past 20 years.
(2) Low prevalence of reperfusion-based treatments seems a more essential issue such that only 26.5% of our patients received thrombolytic during the best period of three mentioned time intervals. Considering that the prescription of thrombolytics is associated with an 18% decrease in mortality risk, it is evident that general results will lack any statistical difference.
Another important point is the effects of the mentioned treatments on mortality and 1-month and longer complications, which were ignored in our study, need further study.
Conclusion
The results indicated prominent improvement in the management of patients suffering from acute myocardial infarction within the past 20 years in accordance with international guidelines. However, there was no significant variation in the prevalence of the main complications and mortality of the patients because of the lack of any appropriate development of treatments based on reperfusion of coronary arteries.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.