
Abstract
Acute coronary syndromes are a clinical entity frequently encountered in practice and are responsible for significant morbidity and mortality, despite therapeutic advances. The initiation of early reperfusion therapy reduces mortality and morbidity and improves patients’ prognosis, but this depends on how quickly patients receive their treatment. Although it is often easy to diagnose in the presence of typical symptoms, certain patients, such as diabetics, sometimes have atypical symptoms, resulting in a delay in management. In nearly 50% of cases, inferior wall ischaemia is accompanied by right ventricular myocardial infarction; the clinical outcomes range from no hemodynamic compromise to severe hypotension and cardiogenic shock. In this article, we present the case of a 54-year-old male patient with active smoking and poorly controlled type 2 diabetes as cardiovascular risk factors who initially consulted at the first hour for epigastric pain, for which he received symptomatic treatment. As the symptoms persisted, he was admitted to our department at the eighth hour, where he was diagnosed with a biventricular infarction.
Keywords
Introduction
Cardiovascular disease (CVD) is the most common cause of death and morbidity worldwide, and acute coronary syndrome (ACS) is often the first clinical manifestation of CVD. 1 Electrocardiography (ECG) should be done as soon as possible (within 10 minutes of presentation) for patients who may have ACS in order to differentiate STEMI (ST-segment elevation myocardial infarction) from non-ST-segment elevation ACS (NSTE-ACS). Approximately 30% of ACS are due to STEMI, which is brought on by total coronary artery occlusion, whereas in 70% of cases, there is no significant ST-segment elevation on electrocardiography (NSTE-ACS) due to intermittent or partial artery occlusion. 2 An early invasive strategy is mandatory as soon as possible, but this requires an early diagnosis, in particular by recognizing the different clinical forms. As the treatment strategy varies according to the diagnosis, the medical history is crucial and must be taken quickly by recognizing the main symptom and gathering information on past medical history, coronary risk factors, and family history. Although chest pain is the main symptom of ACS, atypical symptoms are also frequently seen in the elderly, diabetics, and women, resulting in a delay in treatment. 3 Diabetes mellitus not only plays an important role in the development of coronary heart disease but has also been associated with early and late mortality following ACS. 4 When suffering from acute myocardial infarction (AMI), diabetics are more likely to experience delays in treatment and to present with atypical chest pain. 5 Our article was written according to CAse REports (CARE) guidelines. 6
Case presentation
It is about a 54-year-old male patient with active smoking and poorly controlled type 2 diabetes as cardiovascular risk factors and no past medical history. He presented intense epigastric pain accompanied by nausea and vomiting, which led to his consultation at the first hour from the presumed onset of the pain, where the patient received symptomatic treatment with omeprazole 40 mg (IV) and paracetamol 1 g twice per day and was then sent home. With the persistence of the same symptoms, he consulted to our department at the eighth hour later. On admission, the patient was conscious but still in pain, with a BP of 85/55 mm Hg and a heart rate (HR) of 120 bpm. The ECG showed a complete right bundle branch with ST-segment elevation in the anterior, inferior, and right leads (Figure 1). His biological work-up showed troponin of 10,000 pg/ml (NV < 17 pg/ml), blood glucose of 2.7 g/l with no acetonuria, complete blood count (CBC), and electrolytes were unremarkable. Transthoracic echocardiography showed severe left ventricular dysfunction associated with right ventricular dysfunction (Figure 2). The patient was then put on aspirin 300 mg (loading dose), clopidogrel 300 mg (loading dose), and dobutamine (10 µg/kg/min) and taken directly to the catheterization room, where coronary angiography revealed an occlusion of the proximal left anterior descending artery and an occlusion of the mid-right coronary artery (Figure 3). During the procedure, the patient’s hemodynamic state deteriorated, prompting intubation and the addition of other vasoactive drugs (adrenaline at 1 mg/h, noradrenaline at 0.7 µg/kg/min), which was followed by electromechanical dissociation and nonresuscitated cardiac arrest after 30 minutes of cardiopulmonary reanimation.

(a) Electrocardiography showing a right bundle branch with an ST-elevation in the anterior leads. (b) ST-elevation in the right-sided leads specially in V4R suggestive of Right ventricle myocardial infarction.
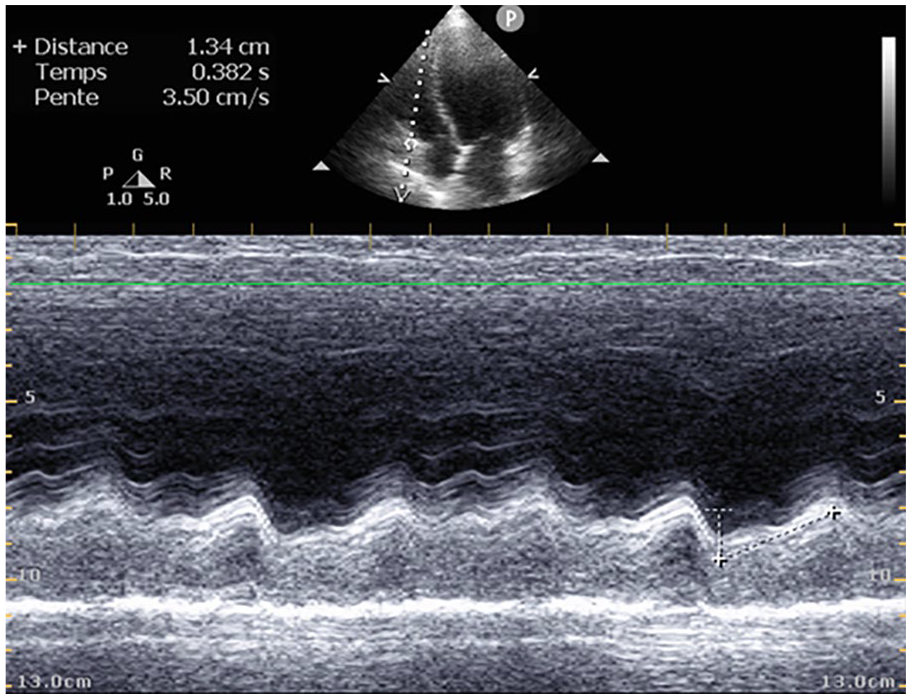
Echocardiography showing right ventricle systolic dysfunction by using tricuspid annular systolic plane excursion-method.
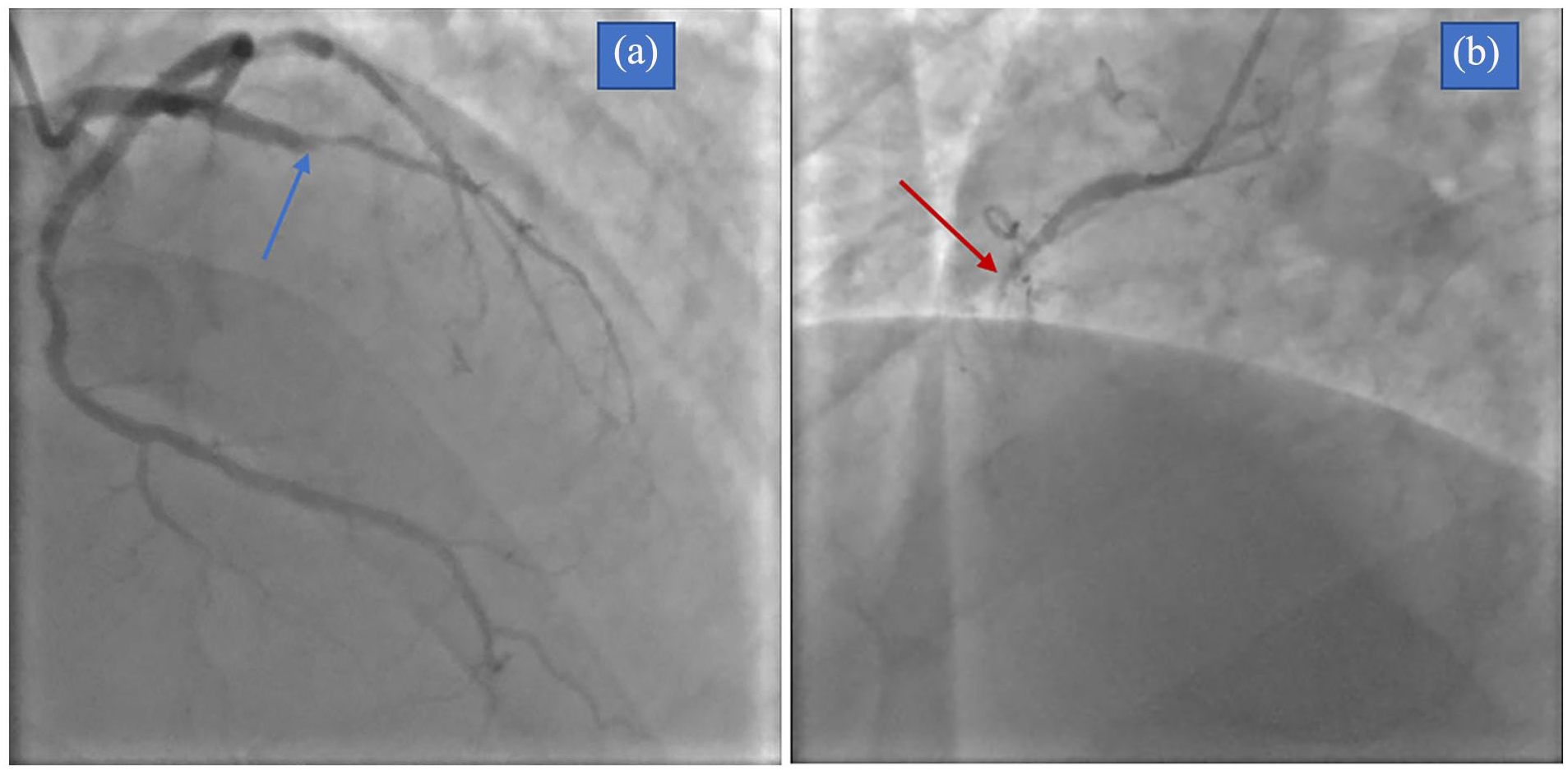
(a) Coronary angiography showing an occlusion of the proximal left anterior descending artery (blue arrows). (b) Occlusion of the proximal right coronary artery (red arrows).
Discussion
AMI is, in most cases, a preventable disorder often triggered by the fissure or rupture of an atheromatous plaque in the coronary arterial wall due to some modifiable risk factors (diabetes, smoking, hypertension, dyslipidemia, obesity, sedentary lifestyle, psychosocial factors, etc.) and nonmodifiable risk factors such as advanced age and genetic history. 7 The incidence of mechanical complications of AMI has gone down since the advent of percutaneous coronary intervention, underscoring the importance of early and appropriate care for these patients. Cardiogenic shock (CS) is the most common mechanical complication and cause of death following an AMI. The most common aetiology of CS is left ventricular dysfunction secondary to extensive infarction. This is a state of inadequate tissue perfusion due to low cardiac output defined by persistent hypotension (systolic blood pressure <80 or 90 mm Hg or mean arterial pressure <30 mm Hg below normal) with a severe reduction in cardiac index of less than 1.8 L/min per m² unassisted or less than 2.2 L/min per m² assisted and adequate or high filling pressure. 8 Inadequate tissue perfusion is the result of reduced cardiac output brought on by left ventricular dysfunction or another mechanical complication. Catecholamines are released in response to hypoperfusion, and while this may raise mean arterial pressure through peripheral vasoconstriction and/or enhanced cardiac contractility, it also increases myocardial demand and raises the possibility of arrhythmias. Reducing blood pressure causes a decrease in cardiac output and coronary perfusion, which further compromises tissue perfusion. 9 Right ventricle (RV) dysfunction can cause or contribute to CS, and predominant RV shock accounts for only 5% of cases of ACS complicating myocardial infarction (MI). 8 Right ventricle myocardial infarction (RVMI) occurs in one-third to one-half of patients with inferior MI and contributes significantly to clinical and hemodynamic instability, increasing in-hospital morbidity and mortality. 10 Early recognition of RV involvement in a patient with acute infarction is very important, not only in terms of prognosis but also for the selection of appropriate therapy, including aggressive primary percutaneous coronary intervention with a special focus on revascularization of the RV branches, in order to avoid any adverse complications associated with this diagnosis. 11 Compared to “simple” left ventricle MIs with an anterior or inferior wall, RVMIs are more frequently complicated by all forms of arrhythmias. In a prospective study conducted by Mehta et al. 12 in order to determine the prognostic impact of RV myocardial involvement in patients with inferior MI, serious arrhythmias, including sustained ventricular tachycardia, ventricular fibrillation, and conduction disorder, were significantly more common in patients with RVMI. Acute RVMI occurs often when there is occlusion of the right coronary artery, especially in its proximal segment. The RV has unique physiological and structural characteristics compared to the left ventricle, thus explaining the low rate and rapidity of recovery after MI. This is due to a number of mechanisms, namely: the RV has thin walls that require less oxygen extraction; because of this, low-pressure perfusion occurs during both systole and diastole; the RV can have rich collaterals from the left coronary artery; and the RV is supplied with blood directly from the RV cavity via the thebesian veins.11,13 Diabetes is often associated with a poor prognosis in patients with AMI, as patients with these comorbidities often have atypical symptoms, therefore leading to delayed treatment. There are already theories regarding the mechanisms underlying atypical symptoms in diabetics. Diabetic patients had a high prevalence of neuropathy, resulting in atypical symptoms. Multivessel disease and complex lesions are more frequent in diabetics, leading to more frequent angina pectoris and preconditioning phenomenon. In addition, diabetic patients often present with symptoms associated with hypoglycemia. As a result, when diabetic patients experience a heart attack, it is difficult for them to promptly recognize whether these symptoms are of cardiac origin or not. 5
Conclusion
Despite advances in therapeutics, AMI remains a burden with a high morbidity and mortality rate. The best way to prevent its complications is to diagnose and manage it early by recognizing the different clinical presentations. Although chest pain is the typical presenting symptom, some patients, especially diabetics, often exhibit atypical symptoms. This case is a good illustration of these atypical symptoms and incites all clinicians to perform a standard ECG in front of atypical presentations in patients at risk.
Footnotes
Acknowledgements
None.
Author contributions
T.H.D. Study concept, Data collection, Data analysis, Writing the paper; R.D.B. Study concept, Data collection, Data analysis, Writing the paper; F.N.Y. Data collection, Data analysis; F.E.A. Data collection, Data analysis; F.M.A. Data collection, Data analysis; N.B. Supervision and data validation; R.F. Supervision and data validation.
Availability of data and materials
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient’s wife for the anonymized publication of this case report.
Research registration
None.
Provenance and peer review
Not commissioned, externally peer-reviewed.