
Abstract
Objectives
We aimed to evaluate the effectiveness of our vascular risk reduction clinic for women who had preeclampsia, in improving patients’ cardiovascular outcomes, self-reported healthy behaviors, and knowledge about their long-term cardiovascular health.
Study Design
Retrospective case-control study where 470 surveys were mailed: half were patients seen in Postpartum Preeclampsia Clinic 2010–2019, and controls were patients who did not attend a scheduled clinic appointment or were seen in Obstetric Medicine clinic postpartum for preeclampsia. Primary outcome was a lack of postpartum weight gain. Secondary outcomes included new vascular diseases, smoking, exercise, and physician follow-up.
Results
Ninety-four (43.3%) of clinic attendees returned survey and 30.3% of controls. Fewer clinic attendees gained weight postpartum, and attendees had fewer hypertension and followed up more with family physicians. Most attendees found the clinic helpful.
Conclusions
Postpartum Preeclampsia Clinic was effective in affecting some vascular outcomes and in improving knowledge and follow-up behaviors.
Introduction
Hypertensive disorders of pregnancy, particularly preeclampsia, have been increasingly recognized as an independent risk factor for cardiovascular disease (CVD). Many national and international organizations have now recommended that women with a history of preeclampsia be followed more closely in the postpartum months and years in order to screen for risk factors to reduce their risk for future CVD.1–4 It is unique in that an index event such as preeclampsia occurs relatively early in a woman's lifetime, before most traditional cardiovascular risk factors are present, which offers an early window for intervention. In addition, pregnancy and postpartum have been identified as a time when women are especially motivated to engage in positive lifestyle changes. 5
The Postpartum Preeclampsia Clinic (PPPC) at the Royal Alexandra Hospital in Edmonton, Canada, was founded in 2010 to identify women at high risk of future CVD based on adverse pregnancy outcomes, screen them for existing cardiovascular conditions requiring pharmacological treatment, and empower them to make lifestyle changes that will reduce their risk of developing CVD in the future. 6 This clinic utilizes a multidisciplinary approach whereby women with a history of preeclampsia diagnosed prior to 34 weeks gestational age are followed in their first postpartum year and are seen by an obstetric internist, a dietician, and/or a pharmacist and/or nurse practitioner. At the clinic, patients are provided with an individualized action plan in order to modify their cardiovascular risk factors, such as blood pressure (BP) control, ruling out dyslipidemia and diabetes, counseling on the heart healthy diet and optimal body mass index, and developing a plan for exercise. However, this clinic is unable to reach all women who have been affected by preeclampsia due to resource limitations, and it is unclear whether women who do not attend the clinic are also provided with education regarding their increased cardiovascular risk. To date, there are very limited data regarding whether this information is communicated to patients effectively and in turn whether these patients feel they have sufficient support and guidance from the medical community to make positive health-related changes. In a focus group carried out in Boston, USA, with 20 patients who had a history of preeclampsia, most participants were unaware of any link between preeclampsia and future CVD. 7 Comparable research has not been conducted in a Canadian population.
We sought to gather information from patients to understand whether their experience at the PPPC led to improved outcomes including maintaining postpartum weight, increased exercise, and ultimately a reduction in cardiovascular morbidity. Additionally, we hoped to compare the perspectives of patients who had the opportunity to attend the PPPC and those who did not, to assess whether the clinic had achieved the intended effect of enhancing patient knowledge and improving outcomes. Lastly, we aimed through this survey to identify barriers in knowledge translation and risk factor modification.
Methods
This was a retrospective case-control study using mailed-out surveys. Patients with preterm preeclampsia (diagnosed before 34 weeks), seen from 2010 to 2019, were identified as cases. Patients with preeclampsia developing prior to 34 weeks were chosen because they are at highest risk of developing long-term vascular sequelae. Control patients were patients who either missed referrals or declined referral to PPPC or had preeclampsia at any gestational age and were seen in the Obstetric Medicine (OB Med) clinic. For control group patients who were not referred to the PPPC, they were searched by using the term “preeclampsia” in the OB Med clinic database to make up the same number of controls as cases for the years. Patients with preeclampsia who were seen in the OB Med clinic were somehow not referred to the PPPC due to not meeting gestational age criterion or due to provider not aware or remembering. Each case and control only appeared once in their respective cohort. The participant with more than one pregnancy complicated by preeclampsia was only counted once. All participants were delivered in the Royal Alexandra Hospital in Edmonton, Alberta, Canada, a tertiary obstetric center with over 7000 births a year.
Both cases and controls were contacted by mail with a letter providing information about the study and inviting their participation, as well as a self-addressed stamped envelope for responses to be mailed back to the research team. Participants were offered a $15 gift card for responding to the survey, which was mailed to an address that the participant provided. This study was approved by the University of Alberta Ethics Board.
The survey captured patients’ understanding of their previous diagnosis of preeclampsia and the implications of this on their long-term cardiovascular health. Information collected included the number of pregnancies complicated by preeclampsia, pregnancy outcomes, current medical diagnoses and medications, and lifestyle and socioeconomic factors. Lifestyle and health behavior data included whether the participants exercised, gained/maintained/lost weight since the pregnancy with preeclampsia, and smoked. Women were asked whether they followed up with their family physician to review BP or cholesterol as instructed by PPPC. For women who attended the PPPC, information on whether they found the clinic to be helpful as well as free text comments were collected. Women who did not attend the PPPC were asked whether they were given information on the future cardiovascular risk, screened for CVD, and who, if anyone, provided them with this information and screening. The survey was written at 6–8 grade reading level, per ethics requirement, and it was edited by a non-research team reviewer.
We chose the primary outcome in assessing the effectiveness of PPPC to be maintenance of postpartum weight, i.e., lack of postpartum weight gain. Although the most interested clinical outcome is the long-term CVD development, a surrogate outcome had to be chosen because the women were surveyed at 1–10 years from their pregnancy with preeclampsia, and so it was unlikely that a significant number of them will have developed clinically significant CVD in this time frame. Since overweight and obesity are well-established risk factors for cardiovascular morbidity, 8 weight gain after pregnancy indicates significant CVD risk, so a lack of postpartum weight gain is felt to be a reasonable surrogate outcome that is independent of prepregnancy weight. All patients who attend the PPPC were provided with an action plan that includes exercise-related goals and optimal weight-setting goal. A 2015 short-term evaluation of our PPPC demonstrated a significant increase in uptake of exercise in the immediate postpartum period at 6 months with a nonsignificant improvement in weight. 5
Our study's secondary outcomes included new diagnoses of vascular events or risk factors that occurred following the pregnancy complicated by preeclampsia.
All responses were anonymous. The responses were entered into REDCap database for statistical analysis. Descriptive statistics were calculated as frequency and percent for categorical variables and median and interquartile range (IQR) for continuous variables. Comparisons of long-term health outcomes between clinic and control groups were done using either chi-squared tests or Fisher’s exact tests where appropriate. For the primary outcome of weight maintenance which was calculated on weight gain since the beginning of the pregnancy with preeclampsia to the survey time, logistic regression was used to estimate the odds of weight gain in clinic versus control groups. An adjusted analysis was built to control for age, employment status, marital status, diabetes diagnosis, current exercise status, number of pregnancies with preeclampsia, and the presence of severe preterm birth. For the purpose of this study, severe preterm birth was defined as any patient with preeclampsia and preterm birth occurring at or before 30 weeks. A descriptive analysis was done using participant comments from an open text box in the survey. All statistical analyses were performed by biostatistician in Women and Children's Health Institute, University of Alberta, using SAS Ver 9.4 (SAS Institute, Cary, NC, USA).
Results
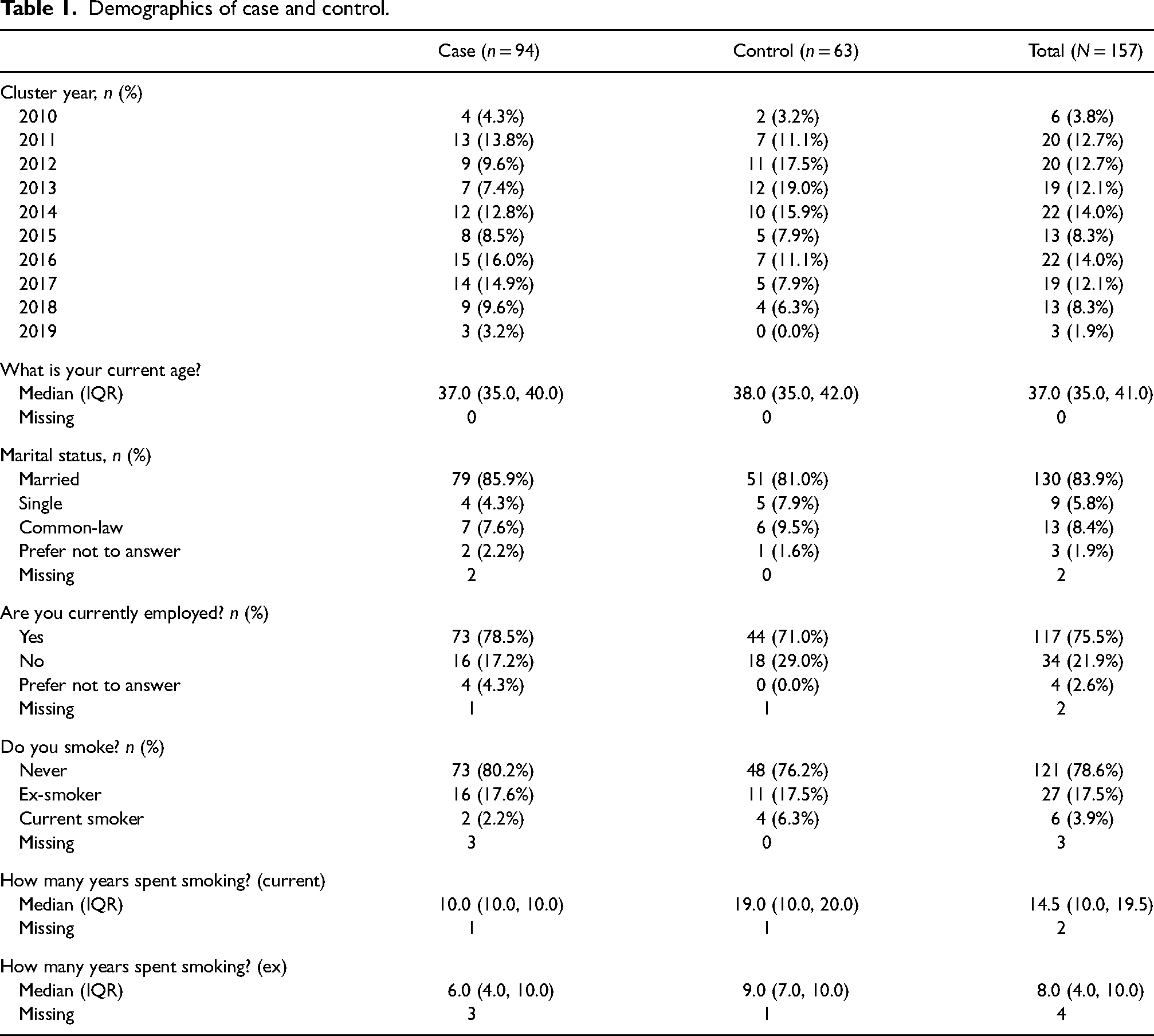
A total of 470 surveys were distributed, with 235 mailed to cases and 235 to controls (Figure 1). Eighteen surveys to cases were “returned to sender,” and 27 to controls were returned. Ninety-four of the clinic attendees returned the delivered surveys, whereas 63 of the controls did. The median age of cases was 37.0 years (IQR 35.0, 40.0) and for controls was 38.0 years (IQR 35, 42.0). More cases were married and employed and were nonsmokers, compared to controls (Table 1).
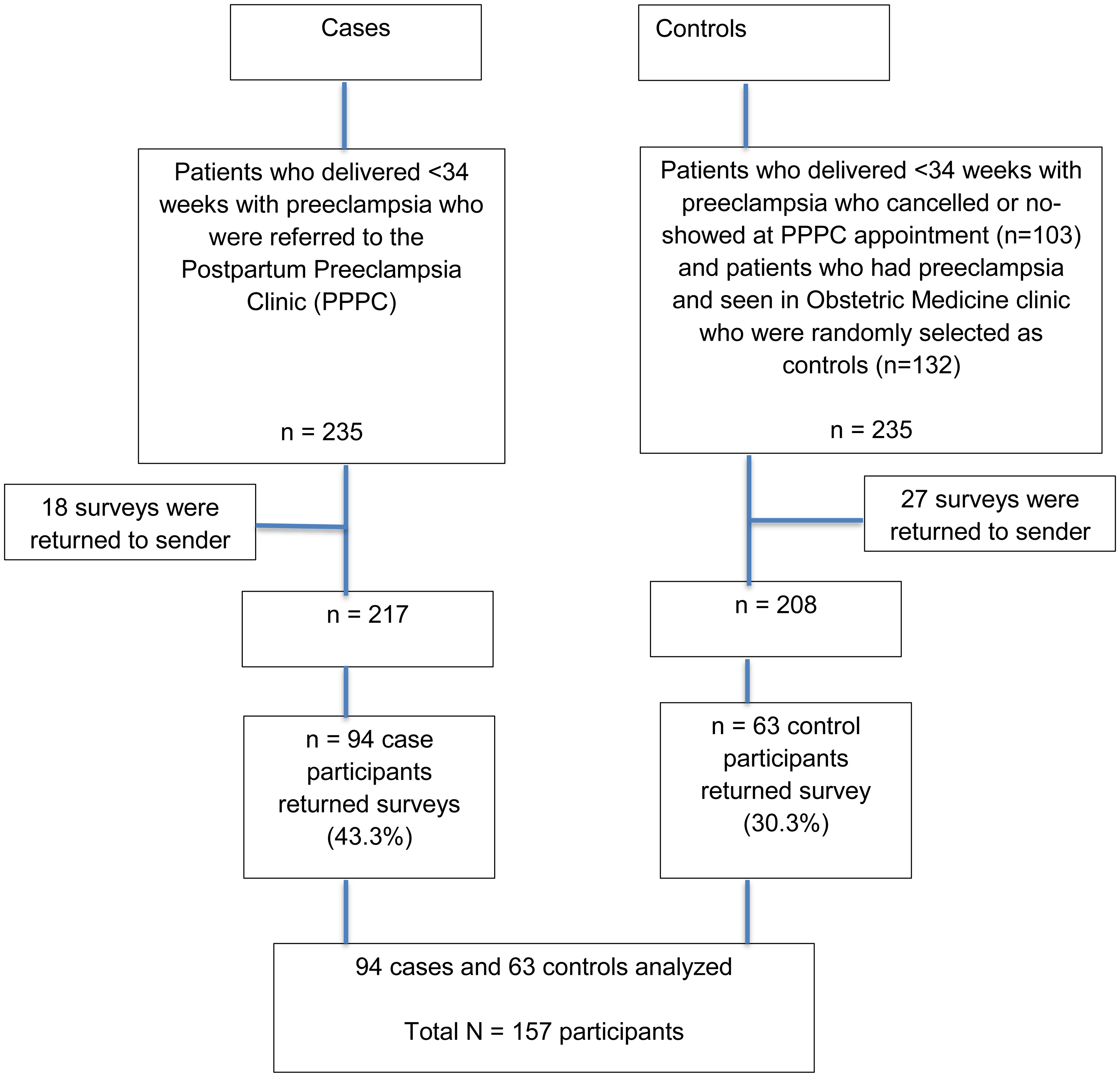
Study flow chart.
Demographics of case and control.
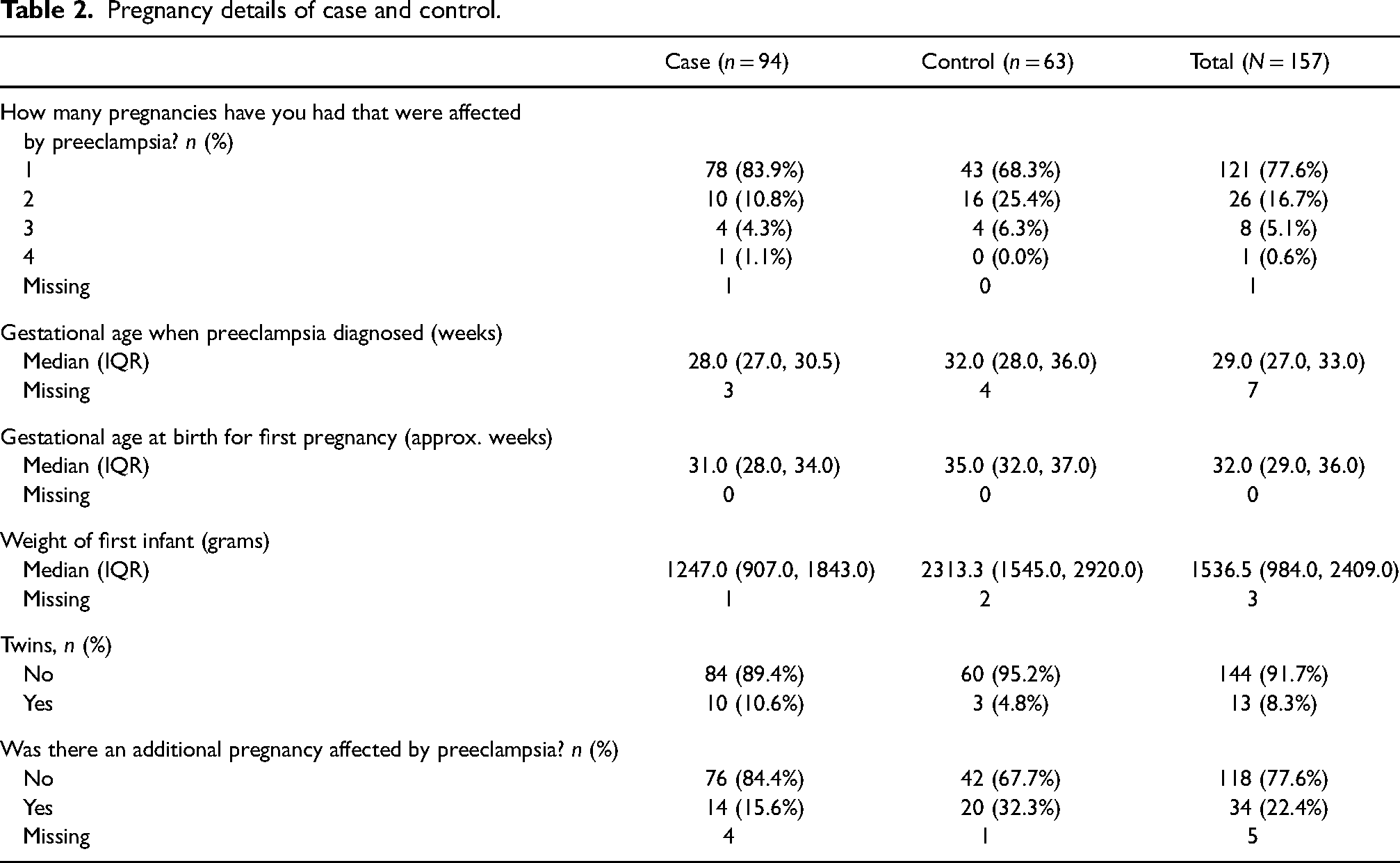
The median gestational age of preeclampsia diagnosis was 28 weeks (IQR 27.0, 30.5) for cases and 32 weeks (IQR 28.0, 36.0) for controls (Table 2). More controls had additional pregnancies complicated by preeclampsia. The median infant birthweight was lower for cases than controls in their first pregnancy affected by preeclampsia, which corresponded to the earlier diagnosis of preeclampsia in these case pregnancies.
Pregnancy details of case and control.
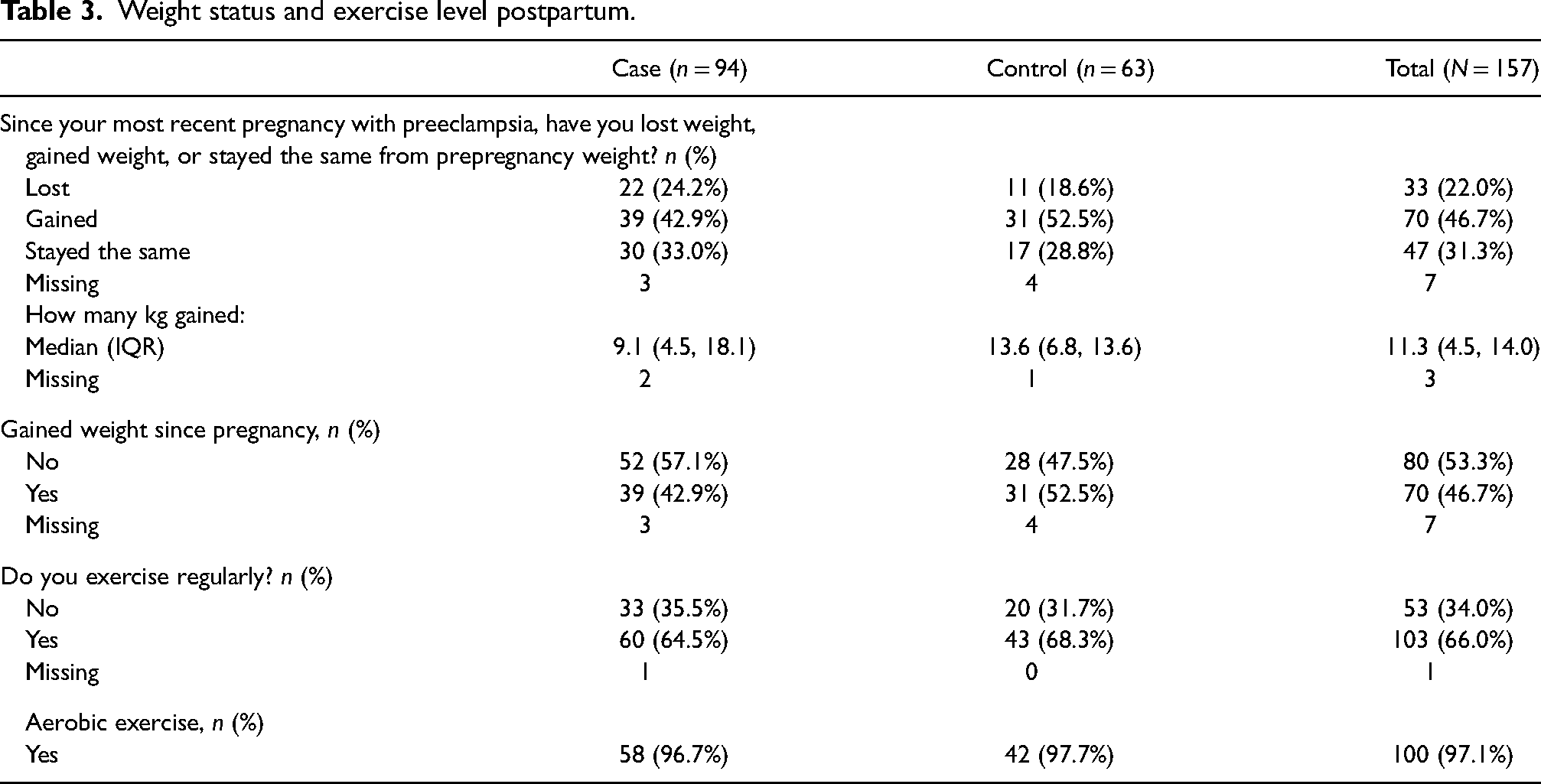
With respect to the primary outcome of weight maintenance in the form of weight gain post-pregnancy with preeclampsia, 42.9% of cases and 52.5% of controls reported that they had gained weight postpartum. Although there were fewer clinic attendees gaining weight versus controls, this did not reach statistical significance (Table 3). When a multivariable model was used to adjust for potential confounding factors, the odds ratio of postpartum weight gain from the clinic attendees was 0.73 (95% CI 0.35, 1.51) with a p value of 0.39 (Table 4).
Weight status and exercise level postpartum.
Adjusted and unadjusted OR (odds radio): weight gain postpartum.

Adjusted for: age, employment status, marital status, diabetes diagnosis, exercise status, number of pregnancies with preeclampsia, and the presence of severe preterm birth (defined in the study as preeclampsia <30 weeks).
In terms of secondary outcomes, clinic attendees had fewer diagnosis of hypertension (7.5% vs. 22.6% of controls, p = 0.007). Fewer clinic participants had diabetes (1.1% vs. 6.7% of controls, p = 0.08) although this did not reach statistical significance (Table 5). Similar proportions of patients in each group reported a diagnosis of high cholesterol (8.9% cases vs. 10.0% controls) and depression (16.5% cases vs. 15.3% controls). Cases were more likely to follow up with their family physician for their vascular risk factor management at 90.2%, compared to 68.3% in controls. In terms of health behaviors, clinic attendees were less likely to be current smokers (2.2% vs. 6.3% of controls). Comparable numbers between groups reported regular exercise, with 64.5% of cases and 68.3% controls responding that they engaged in exercise regularly. Aerobic exercise was the most commonly reported physical activity among respondents.
Long-term health outcomes in case and control.
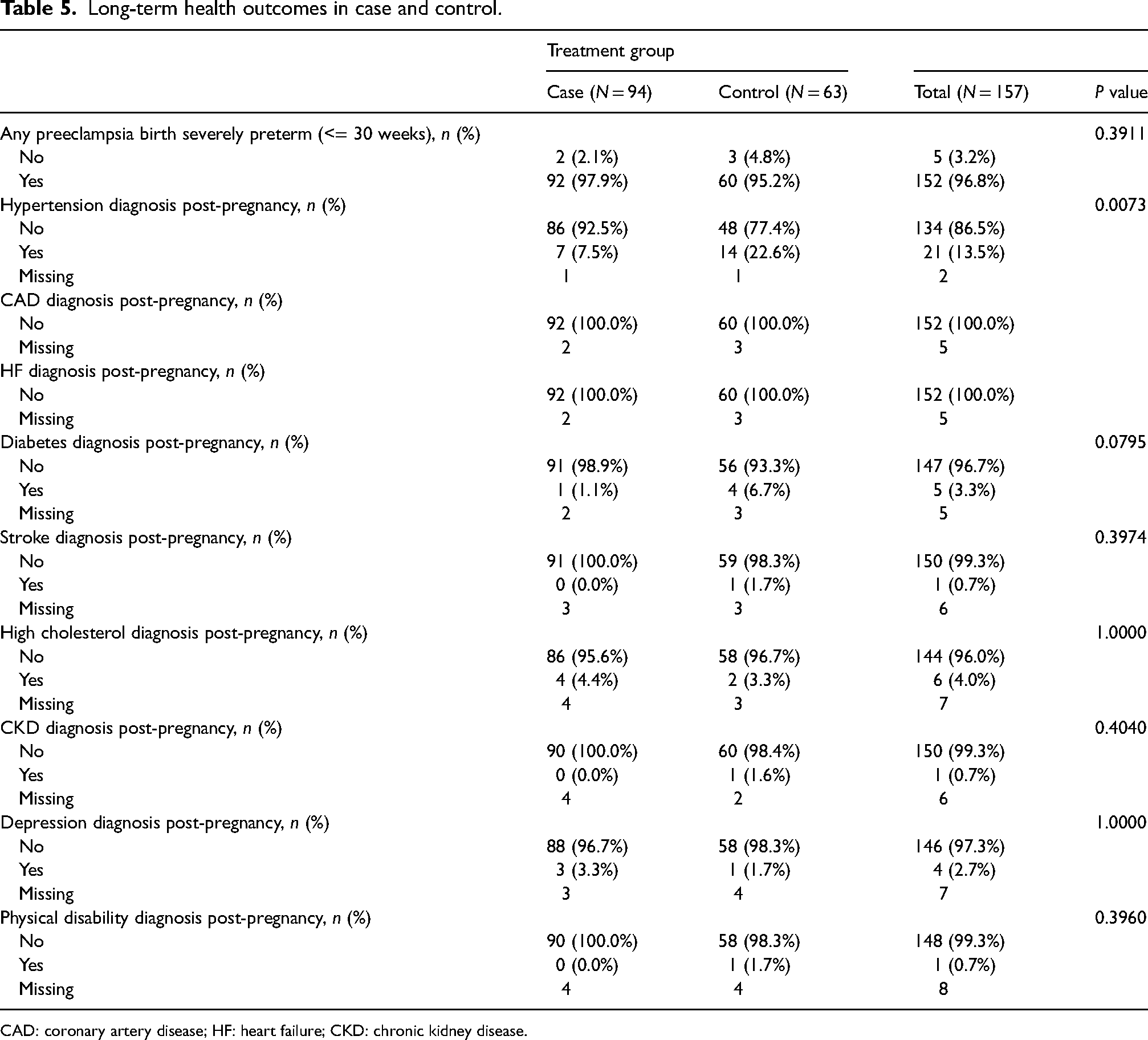
CAD: coronary artery disease; HF: heart failure; CKD: chronic kidney disease.
Among the PPPC clinic attendees, 60.9% found the clinic experience helpful in terms of improving health and maintaining positive lifestyle changes. In contrast, 66.1% of the control participants indicated that they did not recall any health professional discussing the impact of preeclampsia as a cardiovascular risk factor with them. There were many comments from PPPC attendees who felt the clinic was an excellent resource that provided information and support for patients to improve their cardiovascular health. One patient reported that “the clinic did give me information that was helpful for my 2nd, 3rd, and 4th pregnancy where I did not develop preeclampsia.”
Barriers to clinic attendance included distance to travel for women living outside the city and the need to arrange child care in order to attend appointments. “Edmonton is quite far for one to attend the clinic” and “It is asking a lot from a new mom to bring their babies to a hospital to discuss how the need to set health goals from themselves.”
For patients who did not attend the PPPC, they commonly expressed a desire for more information: “If I would have known about the clinic I would have attended!”
There was especially noted to be a lack of clarity with respect to preeclampsia prevention in future pregnancies. One respondent wrote, “My family doctor said he doesn’t do pregnancy stuff and did not say anything except that I should probably try not to have more kids.” Of note, participants were offered to be mailed handouts on preeclampsia and heart disease information: 85% of controls and 79% of cases requested and hence were mailed the relevant clinic and Preeclampsia Foundation handouts.
Discussion
In our study, fewer participants who attended the PPPC over 10 years’ time gained weight postpartum compared to participants who did not attend clinic, although this did not reach statistical significance. Interestingly, about half of the participants gained weight since their pregnancy and less than a quarter lost weight long term. For long-term vascular outcomes, fewer clinic attendees developed hypertension compared to controls. More clinic attendees had follow-up with their family physicians for vascular risk factor management. Most attendees found the clinic helpful regarding education and management of cardiovascular risk factors. In contrast, most control participants did not receive counseling on the impact of preeclampsia as a cardiovascular risk factor. Hence, our study supported that the PPPC was effective in affecting some vascular outcomes and in improving knowledge and follow-up behaviors for this group of high-risk patients.
There is very little evidence to date with respect to patient understanding of preeclampsia as a risk factor for CVD. Previous literature suggests that the majority of women with a history of preeclampsia do not understand its significance as a cardiovascular risk factor. 7 Although the association between adverse pregnancy outcomes including preeclampsia, preterm birth, and fetal growth restriction, and future CVD are well established,1,8 it is not clear whether most of these women are effectively counseled and appropriately treated to reduce their risk. Our data suggested that patients with a history of preeclampsia who did not attend the PPPC had a very limited understanding of this risk, with approximately two-thirds of this group having responded that they were not made aware of the implications of their diagnosis on future CVD. This would suggest that there is a significant room for improvement in terms of targeting this group of patients for education and risk-reduction interventions such as the PPPC. In fact, most respondents to this study, clinic attendees or not, requested further information on preeclampsia and heart disease to be mailed to them, confirming that education on this topic was highly desired by patients.
There have been few published studies to date that assess the efficacy of postpartum interventions aimed at reducing the cardiovascular risk of women with a history of hypertensive disorders of pregnancy. One systematic review identified two RCTs on this topic. 9 One RCT compared calcium supplementation to placebo, and the intervention was found to have a nonsignificant trend toward reducing patients’ BP. 10 The second RCT developed an online intervention including information modules, access to a community forum, and lifestyle coach and found that women who accessed this online tool after a pregnancy affected by preeclampsia had higher self-reported knowledge about their own CVD risk factors but no difference in adherence to the dietary approaches to stop hypertension diet, increase in exercise, weight change, or hypertension compared to a control group. 11 Our intervention, PPPC attendance, involves one-to-one individualized treatment by multidisciplinary team, for example, adjusting BP medications, starting low-density lipoprotein reduction therapies, developing an exercise plan, etc. However, due to the limitations of in-person attendance, it is unlikely to reach as many patients as a virtual intervention has the potential to reach, addressing the barriers of travel and child care that were identified. During the COVID-19 pandemic, the PPPC has transitioned to a virtual platform, using an institutionalized approved Zoom for virtual appointment, which is well-received by the patients and seems to have increased the attendance rate.
Limitations of this study include a small sample size and convenience sample. The total number of patients who have attended the PPPC dictated the number of surveys that were able to be distributed. There was a low response rate, which is typical in postpartum surveys, and this was also contributed by no reminders sent to patients, as the anonymous surveys did not allow identification of those who did not respond to have a reminder. These factors may limit our ability to find any small effect sizes that may actually exist. There is also a risk of recall bias given the data collected was based on information provided by patients. However, the benefit of using a survey to collect this data is that it allowed for the collection of patient perspectives and experiences that would not necessarily be captured by looking solely at medical records. It would have been great to capture prepregnancy BMI; however, due to perceived sensitivities around reporting specific weight, it was decided to ask for a self-reported weight difference.
Another limitation is the risk of selection bias, given half of the control group was selected from also a specialized clinic, namely, the OB Med clinic. The patients who had preeclampsia may have received cardiovascular risk education counseling by the obstetric internist, which would underestimate the difference between the case and control findings of the study. These characteristics may also limit the generalizability of the data collected. Selection bias is also an inherent risk of survey data in general, also because the patients who are motivated to complete the survey may not be reflective of the entire population being studied. Finally, due to the fact that the PPPC is only able to see patients who have had preeclampsia prior to 34 weeks, our case group inherently had more severe risk factors compared to controls. But because the surveys were anonymous, it was not possible to ascertain whether the control respondents were from the PPPC-referred patients or non-referred patients with possibly different medical risk profile. The median age of preeclampsia diagnosis in the case group was 28 weeks, compared to 32 weeks in the control group, which may have led to an underestimation of the clinic's effect. Despite this, the patients who attended the clinic still reported fewer long-term hypertension and weight gain.
Conclusion
This study was one of the first studies to use patient-reported data on patient's perspectives, clinical outcomes, and follow-up behaviors over 10 years’ clinic time to examine the effectiveness of a postpartum vascular risk reduction clinic, which showed some promising results. There is more room to improve the care of these patients, as it is unfortunately only the minority of women with preeclampsia who are currently able to access the PPPC or similar clinics. This can be prioritized both at the level of the individual clinician providing postpartum counseling and at the institutional level by allocating more resources to develop and support similar care models for this population.
Future research is required to determine the proportion of women who have pregnancy-associated cardiovascular risk factors that are currently being counseled and offered interventions to modify their risk. A needs assessment should to be performed to establish the content of this education.
Footnotes
Acknowledgments
We would like to acknowledge Dr Sue Ross (University of Alberta) for her assistance in development of the survey that was used for this study and Sarah Rathwell in Biostatistics in Women and Children's Health Research Institute (WCHRI) for performing the statistical analyses.
Contributorship
WWS and AP contributed to the design, analysis, and manuscript of the study. LS contributed to the data entry, analysis, and manuscript. GP contributed to the design and manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the University of Alberta Ethics Board number Pro00092260.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Women and Children's Health Research Institute's Resident/Clinical Fellow Trainee Research Grant at the University of Alberta, and the Royal Alexandra Hospital Foundation.
Guarantor
Winnie Sia guarantees this manuscript's accuracy and the contributorship of all co-authors.
Informed consent
All participants provided consent when they returned the survey in the provided envelopes.