
Abstract
Background:
Postpartum is a critical period to interrupt weight gain across the lifespan, decrease weight-related risk in future pregnancies, promote healthy behaviors that are often adopted during pregnancy, and improve long-term health. Because the postpartum period is marked by unique challenges to a person’s ability to prioritize healthy behaviors, a multi-level/domain approach to intervention beyond the individual-level factors of diet and activity is needed.
Objectives:
The purpose of this study was to understand postpartum people’s perceptions about the relationship between their social networks and support, and their health behaviors and weight.
Design:
We used a qualitative descriptive approach and in-depth interviews.
Methods:
Participants (aged 18+, 12–15 months postpartum, who had a pre-pregnancy body mass index ⩾25) engaged in one-on-one, in-depth interviews conducted via Zoom (n = 28). Additional qualitative data came from open-ended responses to an online survey (n = 84) and a personal social-network survey (n = 84). Qualitative analysis used content and thematic analysis in stages of deductive coding applying codes derived from social-network and support theories, followed by inductive coding.
Results:
Thirty-eight participants (38.4%) returned to or weighed less than pre-pregnancy weight. We identified two overarching themes grounded in social-network and support theories. They were: (1) normative influence impacts health behaviors, body image, and experiences of weight stigma, and (2) network social support is related to health goals and overall postpartum health. Postpartum networks/support hindered and supported participants’ goals. Partners provided an important source of accountability but were often associated with barriers to healthier behaviors.
Conclusion:
Our findings reinforce the importance of the social context when considering how to support healthy behaviors and weight during the postpartum period. Healthcare providers should focus on health indicators other than maternal weight, and those wishing to support healthy postpartum behaviors could focus on child and family health, rather than solely on maternal weight and health behaviors.
Plain language summary
Why was this study done?
Pregnancy weight that is retained postpartum is common, and it’s associated with increased risk for diseases such as cardiovascular disease and type 2 diabetes. Research targeting postpartum weight has usually focused on postpartum people’s diet and physical-activity behaviors. However, the postpartum period is marked by unique challenges that impact a postpartum person’s ability to engage in healthy behaviors. Therefore, exploration of how the postpartum social context impacts health behaviors and weight is needed.
What did the researchers do?
We conducted one-on-one, in-depth interviews and collected open-ended responses during surveys with postpartum women. We did this to learn about their experiences of their social networks and social support, and how these aspects of the social environment impacted their healthy behaviors and weight during the postpartum period.
What did the researchers find?
We learned that postpartum women’s social networks both hindered and supported their diet and level of physical activity. For example, women’s partners could provide an important source of accountability for healthy behaviors. Partners could also make it more difficult for participants to maintain dietary goals through partners’ preferences for convenience and snack foods. Additionally, partners were often participants’ primary source of social support for physical activity. When partners’ schedules made it difficult for participants to have time away from children for exercise, participants were often less active as a result. We learned a variety of types of social support contributed to participants’ ability to eat a healthy diet and be more physically active. Social support was also essential for supporting participants’ mental health and wellbeing during the postpartum period.
What do the findings mean?
Our findings shed light on how social networks and social support impact postpartum health behaviors and weight. Additionally, our findings indicate that interventions could benefit from harnessing social-network strengths. Interventions could help participants to identify mutually shared goals for healthy behaviors among their networks while also accounting for identified network barriers to healthy behaviors.
Keywords
Introduction
The postpartum year is an important period to focus on long-term health. It is a critical time to interrupt weight gain across the lifespan, 1 thereby reducing weight-related risks in future pregnancies,2,3 as well as long-term health risks.4 –10 It is also an advantageous time to intervene, supporting motivation for behaviors such as healthy eating and physical activity, which are often established during pregnancy.11 –13 However, the postpartum year is characterized by unique challenges that make it difficult to focus on healthy behaviors. These challenges include reduced personal time, caregiving responsibilities, and professional adjustments as a result of motherhood.14 –17 These challenges impact childbearing people’s ability to prioritize healthy diet and physical activity.18 –20 While a focus on postpartum diet and physical activity is justified in our efforts to support healthy weight postpartum, 21 the complexity of the postpartum context requires a more responsive approach to intervention that also takes into account the impact of the social environment.
The postpartum year is associated with changing social networks. For example, parents’ social-network size has been shown to shrink, and parents are less satisfied with their family relationships postpartum. 15 These social-network changes may be compounded for childbearing people from racially and ethnically diverse backgrounds for whom the opinions and health beliefs of network members may be particularly salient.20,22 An example of this relates to the cuarentena practices of some women of Hispanic/Latino ethnicity, where family members may provide dietary and physical-activity guidance for their postpartum family members. 22 An understanding of these processes is needed for culturally relevant intervention that aims to support healthy behaviors and weight postpartum.
A person’s social network is the web of people with whom they have relationships, such as family, friends, neighbors, and community members. 15 Evidence is strong that social networks can support or hinder healthy diet and physical activity through several mechanisms. Social ties can be a source of normative influence, where their “typical” behavior influences what one thinks is normative and acceptable. An example of functional features of social networks is illustrated in a study focused on Mexican-origin family networks, where encouragement to eat more fruits and vegetables and engage in physical activity was associated with motivation to adopt these behaviors. 23 In addition to these functional social-network processes, structural characteristics of social networks may also impact diet and physical activity. For example, densely connected social networks—that is, networks with a greater number of social ties among its members—have been associated with less loneliness among pregnant women. 24
Relationship ties can also provide sources of social support.23,25 –28 The role of social support in postpartum weight retention has received little attention in the literature, but a few studies demonstrate the potential importance of social relationships to postpartum health behaviors and weight. These studies point to potentially important sources of social support, and they indicate ways these sources may be influential in health behaviors and postpartum weight. For example, support from a significant other is associated with postpartum people’s engagement in more walking and lower odds of retained weight postpartum. 29 Support from family and friends is associated with increased light-to-moderate levels of physical activity 29 and vigorous physical activity. 30 Additionally, connecting with family once a week or less (versus more frequently) during pregnancy is associated with greater postpartum weight retention. 31 Among the limited qualitative work, social support has emerged as an important factor with respect to postpartum people’s ability to engage in and sustain healthy-behavior change during the postpartum period.22,32 –34
When considering effective ways to support long-term health among the childbearing population, understanding the role of social networks and social support is needed to expand the current primary intervention focus on individual-level postpartum diet and activity to also include multilevel and domain considerations of the postpartum social context. To address this gap, this study sought additional understanding about postpartum people’s perceptions of the relationship between their social networks and support, and their health behaviors and weight.
Methods
In this report, we detail the qualitative findings of our cross-sectional, explanatory-sequential mixed-methods study that investigated associations between social network characteristics and postpartum diet, physical activity, and weight change. The study was conducted between December 2022 and December 2023. Qualitative data were collected during in-depth interviews and from open-ended responses to the individual-factors and personal social-network surveys.
Theoretical foundation and study design
We used the theories of normative influence and social support. Foundational to the theory of normative influence through diffusion are social norms, where behaviors that are perceived to be common within a social network may be adopted by members of that network. 35 The impact of social support has been shown to have both direct and buffering effects on health.36,37 Direct effects in this study were related to the health behaviors of people within the networks (e.g., a partner’s eating habits aligning with a participant’s goals). Buffering effects were related to the network members’ ability to help buffer stress, and in this way these effects provided an opportunity to support healthy behaviors and well-being (e.g., a network member providing childcare so a participant can exercise).
We used qualitative descriptive methodology. 38 We selected this approach because few studies have attempted to qualitatively understand this study’s topic, despite strong evidence that relationships influence weight-related health behaviors. This methodology is useful for gaining a comprehensive and straightforward description of the research topic, which is not well understood. 39 This approach assisted with our objective, which was to gain a rich understanding of how postpartum people perceive their social relationships impacting (1) their dietary choices, (2) their ability to engage in physical activity, (3) their personal goals to lose weight gained during pregnancy, and (4) their beliefs about their networks’ social norms on the topics of health behaviors and weight. Qualitative description is a lower-inference approach, prioritizing the presentation of qualitative results that are neutral in description, and that use plain language closely reflecting the participants’ perspectives and their own language. 40 This approach was suitable for and supported the study’s mixed-methods aim, which was to identify factors of participants’ experiences that help to explain the impact of social networks on postpartum health behaviors and weight.
Last, we collaborated with a community advisory board (CAB) before the initiation of each phase of our mixed-methods study. The CAB was composed of two postpartum women, a community health worker, and a Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) nutrition coordinator. For the qualitative portion of our study, the CAB reviewed our sampling strategy and interview guide. The CAB provided feedback to refine the appropriateness and applicability of the guide’s questions. Additionally, de-identified results of the qualitative analysis were shared during a participant talk-back session to learn participants’ insights about the study’s findings.
To support the trustworthiness of data collection within this study, credibility criteria were addressed prior to the initiation of each phase of the study. The study’s materials and procedures were reviewed for appropriateness and applicability by the study’s CAB. Additionally, for the qualitative coding, the primary investigator (a PhD and registered nurse) who was formally trained in qualitative methods and has led qualitative research teams collaborated with two research assistants (undergraduate nursing students) of Hispanic/Latino ethnicity who were able to provide insight during the qualitative analysis. We believe these measures, combined with the primary investigator’s commitment to self-reflection and awareness of their privilege as a White woman, have helped to minimize the limitation of research led by a researcher of the predominant race in the United States.
Purposive sampling strategy
As this was an explanatory-sequential mixed-methods study, we created a sampling strategy that would connect the quantitative arm of the study to the qualitative arm. The purpose of this design is to leverage the qualitative phase to help explain results of the quantitative phase. 41 We created a correlation matrix after collecting 50% of the quantitative data in order to identify a focal quantitative result for our qualitative sample strategy. The correlation matrix assessed correlations between network norms and support (please see Supplemental Material, Correlation Matrix Variables for details) and the binary outcome of postpartum weight retention (yes or no). A moderate positive correlation was found between weight retained postpartum and network difficulty (i.e., network difficulty was defined as the presence of one or more network members who made it difficult for participants to achieve their healthy-lifestyle goals). Therefore, we sampled participants who did and did not report network difficulty, stratified by weight status (i.e., participants who weighed more than their pre-pregnancy weight, and those who returned to their pre-pregnancy weight or lost additional weight). Additionally, in order to ensure a racially and ethnically balanced sample, a goal was set for sampling by race and ethnicity within each sampling category. This goal was to interview, per weight-status category: approximately three participants of Hispanic/Latino ethnicity; two participants who were non-White, non-Hispanic (including participants who identified as having a racial background of American Indian/Alaska Native, Black or African American, South or Southeast Asian, Native Hawaiian or Pacific Islander, and non-Hispanic participants who identified as having more than one racial background); and two participants who were White, non-Hispanic.
Eligibility criteria and recruitment
Study inclusion criteria were: (1) aged 18 or older; (2) 12- to 15-month postpartum after giving birth to a live infant; (3) pre-pregnancy weight in the overweight (body mass index (BMI) 25–30) or obese (BMI >30) category; (4) read and understood English; and (5) received care at UUHealth. Study exclusion criteria were: (1) did not speak English, and (2) did not have access to the internet and web-based technology.
We recruited participants in collaboration with partner sites of the Obstetrics and Gynecology Research Network (OGRN). OGRN is the research infrastructure for the Department of Obstetrics and Gynecology at the University of Utah Health. We included a subsample of the participants from the quantitative arm of our study for the in-depth interviews. We continued purposeful sampling and data collection until data saturation and sampling according to the sampling frame had been met.
Interview guide
The one-on-one interviews built upon the quantitative arm of our study in three ways. First, we created a sampling frame based on results from the quantitative phase of the study. Second, we generated social-network visualizations to help facilitate interviews. And third, we tailored the interview guide to follow up on the quantitative feature of network difficulty.
We developed the semi-structured guide following principles of qualitative description and using frameworks provided by Rubin and Rubin 42 and Krueger and Casey. 43 Interview questions were open-ended. We aimed to develop questions that were neutral in nature and that did not assume a particular perspective or contain forms of bias. With that aim in mind, the interview guide was refined by all members of the research team and the CAB. Additionally, prior to qualitative data collection, we refined the interview guide to help explain quantitative results that required further inquiry, allowing for the qualitative results to provide an extended explanation of the quantitative results. 41 Specifically, a section on network difficulty was created in order to learn about the presence or absence of network difficulty. Additional questions about network difficulty were developed to prompt responses about the difference in difficulty coming from people of different relationship roles, such as difficulty the participant’s mother might cause versus their partner. Questions about network difficulty also explored how differing degrees of closeness, differing frequencies of contact, and differing distances in living may have impacted participant experiences of network difficulty. For example, how does living with the person who causes network difficulty impact health behaviors versus living in a different state? To view the semi-structured interview guide, see Table 1.
Semi-structured interview guide.

In addition to in-depth interviews conducted by the lead author, the qualitative analysis also included open-ended responses of the complete study sample from the online cross-sectional individual-factors survey (n = 84) and personal social-network survey (n = 84). Open-ended responses from the individual-factors survey came from the following prompt: “I’m interested to learn your thoughts about how your social relationships impact your postpartum weight, diet, and level of activity.” Open-ended responses from the personal social-network survey came from the following prompt about each member of participants’ networks: “If relevant, tell me briefly about how this person impacts your goals for a healthy lifestyle.”
Data collection
We conducted interviews via Zoom at a time selected by participants. Privacy and participant comfort were prioritized, as discussing the topic of weight can be difficult. 19 Data collection continued beyond saturation so that the sample could be balanced by the presence or absence of network difficulty, by participant weight status, and by race and ethnicity.
Data analysis
We coded transcriptions of audio-recorded participant interviews in the web-based software Dedoose version 9.0.107, Los Angeles, CA. 45 We imported participants’ demographic information and measurement scores from the individual-factors survey as descriptors that were linked with interview data.
We began data analysis by reading and familiarizing ourselves with the transcripts. The analysis team created notes (referred to as memos) during this familiarization process. Memos were recorded as comments on the interview transcripts, and they included three types of memos: (1) reflexive (e.g., reflections on the analysis process and personal insights), (2) analytical (i.e., connections to the research domain, including where data aligned with the literature and where it diverged, and reflections about how the qualitative data might connect to the study’s quantitative findings), and (3) methodological (i.e., notes about how the research procedures worked and could be refined).
We analyzed data using thematic and content analysis46,47 and deductive and inductive coding. Our deductive analysis used a priori codes based on the social-support and norms literature. This allowed us to align our coding definitions with the literature and to identify concepts related to the theories on which our study is based. Specifically, we coded for: (1) types of social support; (2) the presence of social influence and (3) norms; and (4) participants’ use of social selection. Because the inductive analysis process was grounded in the qualitative data, it helped us to gain a comprehensive understanding of the impact of social networks on diet, physical activity, and weight and yielded a broader conceptualization of postpartum behaviors than the deductive coding alone. 47 The combination of inductive and deductive coding allowed the theoretical concepts of network support and normative influence to be grounded in the data through deductive identification of these concepts, while also allowing for participants’ insights to contribute new understandings of these phenomena through inductive inspection of the data. After an initial coding session of 10 interview-transcript segments, interrater reliability was assessed by calculating a Cohen’s kappa. 48 The coding team then completed the deductive coding process. The kappa score for the social-support coding session was k = 0.95, and the kappa score for the social-influence and health-behavior coding was k = 0.935.
We measured thematic saturation as a function of theme production using the approach outlined by Guest et al. 49 We used their definition of saturation, which is the point at which interviews produced few or no new themes (i.e., ⩽5% new information). See Table 2 for coding categories, codes, and definitions.
Qualitative codebook.

The COnsolidated criteria for REporting Qualitative research (COREQ) checklist was referenced for guidance on reporting the study’s findings. 50
Ethical considerations
Due to the low-risk nature of this study, the University of Utah Institutional Review Board (IRB) determined the study to be exempt and granted a waiver-of-consent documentation (IRB_00151195). The first element of the study’s individual-factors questionnaire was a consent cover letter that contained information about the voluntary nature of the study, the purpose of the research, and potential risks associated with study participation. After reading this cover letter and before beginning the survey, participants were prompted to acknowledge their understanding of the research purpose and voluntary nature of the study by electronically signing and dating the letter.
Results
In-depth interviews lasting between 30 and 60 min were conducted with 28 participants who had completed both the online cross-sectional individual-factors survey and the personal social-network survey from the quantitative arm of the study. Additional qualitative data came from 84 open-ended responses to an individual-factors survey question, and from another 84 responses to the personal social-network survey open-ended questions. Please note that participants were included in the qualitative analysis if they contributed to at least one of these and were free to contribute to all three. Table 3 outlines the participant demographics. More than half were White (n = 61, 61.6%). The majority were of non-Hispanic/Latino ethnicity (n = 55, 55.6%). Thirty-eight participants (38.4%) returned to or weighed less than pre-pregnancy weight.
Qualitative participant demographics (n = 99).

SD: standard deviation; BMI: body mass index.
n = 92.
n = 97.
The main themes identified through the analysis were: (1) normative influence impacts health behaviors, body image, and experiences of weight stigma, and (2) network-social support is related to health goals and overall postpartum health.
Theme 1: normative influence impacts health behaviors, body image, and experiences of weight stigma
This theme helps to elucidate the ways in which normative influence was relevant to the participants’ dietary habits, level of activity, and weight. Normative influence was also a feature of women’s experiences of body image and weight stigma.
Normative influence and diet
While participants often associated social engagement with an increase in their physical activity, they also identified social engagement with the shared consumption of food. The sharing of food was viewed as associated with both poorer and healthier eating habits. Two participants provided comments that help to illustrate this contrast. The first participant said, “I feel like it depends on who I’m hanging out with whether it’s going to be a good choice or it’s going to be like, I’m gonna feel really bloated” (Participant 7; retained postpartum weight; Hispanic/Latino, Black; in-depth interview response); and the second described the contrasting eating norms of her family with those of her in-laws:
My immediate family, my parents, my sisters, I wouldn’t say they’re supporters. In fact, I would say the complete opposite. I would say that they inhibit my goals and what I try to do and so, being around them is a struggle and not that it’s malicious, or on purpose. But because they don’t have the same goals as I do, it makes it really hard for me to stay on track with those goals because I lack willpower and self-control. When they, you know, get junk food or they want to order out, I’m all too happy to indulge. Versus my in-laws are the complete opposite. They eat very healthy; they encourage us to eat healthy. And if anything, I worry about judgment there so I am even more strict or diligent in trying to keep my goals. So, it’s a very interesting, kind of, contrast of these two ends of the spectrum. (Participant 62; returned to pre-pregnancy weight; non-Hispanic/Latino; White, AI/AN; in-depth interview response)
In this second case contrasting social-network influence on diet, the participant said that, for the most part, she has been successful in creating boundaries with her family and felt that her in-laws, despite feeling some judgment, provided a safe resource for dietary guidance.
Within the household, partners were often identified as central to both healthier and unhealthier dietary norms. Partners could help support healthier dietary norms through their preference for healthier ingredients. They could also support unhealthier norms through preferences for treats, snacks and convenience foods, and the facilitation of social eating, despite a lack of hunger.
Similarly, friends, family, community members, and coworkers were identified as broader network members who influenced both healthier and unhealthier dietary norms. Participants described the role-modeling of healthier behaviors by their network members, such as providing an example for eating smaller portions, and witnessing the benefits of prioritizing fruits and vegetables and limiting meat. Several participants talked about friends, family, and community members who shared healthy, balanced meals with them on a regular basis. A few participants had family and friends who grew vegetable gardens and who shared their harvests with participants. Several women also mentioned friends who shared healthy snacks with them and their children during playdates. In contrast, some participants also described playdates as an opportunity to indulge with other moms in snack foods and higher fat-content foods. Other unhealthier dietary behaviors participants described included network members’ preference to eat out at fast-food restaurants and locations with fewer healthy options. Often, participants described feeling pressure or a desire to make less healthy selections when at these venues.
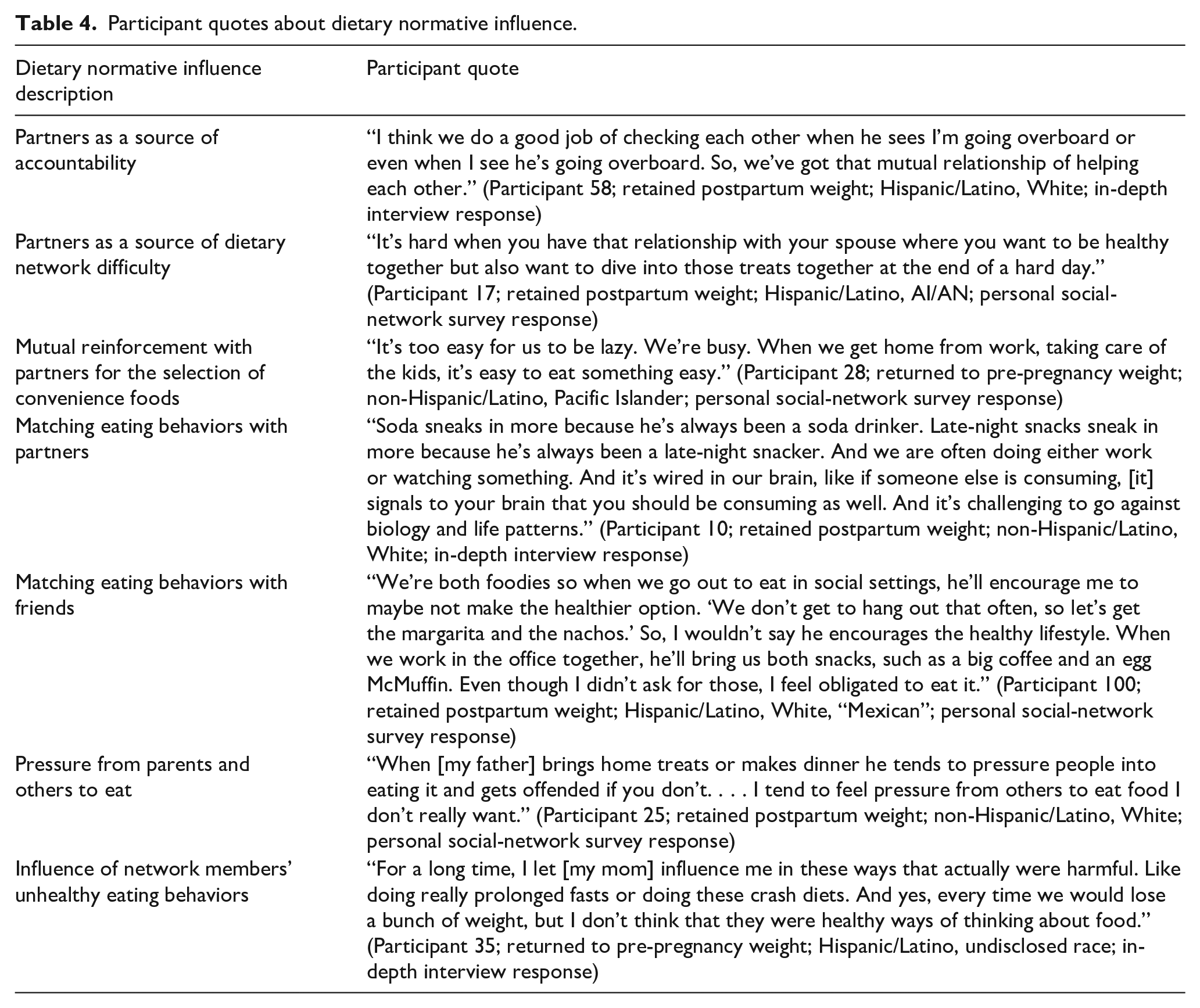
Additionally, the mothers of participants were sometimes identified as negatively influencing dietary behaviors through encouragement to join them in “crash diets” aimed at weight loss. Dietary norms that were embedded in the family, cultural, and societal environments also impacted participants’ dietary behaviors. Early family experiences with dietary norms set the foundation for healthy and freshly prepared foods for some women, while others said they did not learn to meal-plan or cook because their family’s diet mostly consisted of convenience and fast foods. Societal food norms present in the United States were also discussed, such as the norm of over-eating, too-large portion sizes, unhealthier options and ingredients, and proximity to fast food and take-out in urban areas. For additional quotes relating to dietary normative influence, please see Table 4.
Participant quotes about dietary normative influence.
Normative influence and physical activity
Just as shared eating was viewed as a social activity, participants’ increased physical activity was often attributed to social engagement. Participants said they matched their level of physical activity to network members, which sometimes resulted in participants pushing themselves physically in order to keep up with their network members. An increase in physical activity was reinforced for participants who used social selection of network members for those network members’ higher level of physical activity. Again, partners were identified as central to physical activity, where partners could help with participants’ increased or decreased levels of activity, depending on the partners’ physical-activity norms. The participants’ children were seen as both motivators and barriers to physical-activity engagement. Physical-activity norms related to the social and natural environments were important to participants’ level of activity. Several women connected their commitment to an active lifestyle with their family upbringing, which was rooted in shared support for physical activity. Additionally, several women said they believed Utah’s outdoor culture facilitated their active lifestyles. See Table 5 for additional quotes about the impact of normative influence on physical activity.
Participant quotes about physical-activity normative influence.

Normative influence and weight, body image, and weight stigma
Participants of this study were divided in their experiences with network discussions about postpartum weight. Some participants said it was not the norm to talk about postpartum weight and it was even a topic to be avoided. Others said it was normal for family members to raise the issue without solicitation or consent by the participants. Participants were aware of a dichotomy related to postpartum weight. On one hand, there was familial, cultural, and societal pressure to “bounce back.” On the other hand, sometimes family members would discourage participants from being concerned about their weight and encourage them to take it easy, even after participants felt ready to increase their physical activity and lose weight. Participants said there were conflicting and often confusing social-media messages about weight, body image, and body positivity. Additionally, participants’ mothers could sometimes be overly preoccupied with weight. In these instances, participants often said this preoccupation of their mothers could negatively impact their diets and levels of activity. For this reason, one participant made clear her belief that not all social intervention is positive, even if it results in weight loss, as it might also cause poorer mental health and a damaged relationship with one’s body.
Familial norms of weight impacted participants’ beliefs about weight and their health behaviors. This was discussed in relation to a process of healing damaged ideals about body image, food, and physical activity. It was also described as participants’ processes of realization about family norms for overweight, which then motivated the participants’ commitment to health through healthier behaviors than those that had characterized their childhood family environments.
Several participants talked about how social support could help buffer the unhealthier network norms related to weight. This support was in the form of friends and partners who helped to buffer pressures from societal norms and the participants’ mothers’ unhealthier dietary and weight beliefs. The result of this support was improved body image and acceptance of changes in participants’ bodies as a result of childbearing.
Last, several women described experiences of weight stigma within the healthcare setting that impacted their mental well-being. These participants believed discussions of postpartum weight should be addressed with sensitivity. One woman said that after being weighed prior to a doctor’s visit, a registered nurse commented that she hadn’t lost as much weight as other postpartum patients. She said that the comment “killed [her] a little bit” (Participant 39; returned to pre-pregnancy weight; non-Hispanic/Latino, White; in-depth interview response). A second participant said she switched obstetrician-gynecologist (OBGYN) providers in the last 3 weeks of her pregnancy because of insensitive comments about third-trimester weight gain made by her male OBGYN: “That was stressful, but I really felt like someone who could perpetuate that weight stigma and place so much emphasis on a pregnant woman’s weight, didn’t need to be with me postpartum” (Participant 50; returned to pre-pregnancy weight; non-Hispanic/Latino, White, AI/AN; in-depth interview response). See Table 6 for additional quotes about the impact of normative influence on issues relating to postpartum weight.
Participant quotes about postpartum weight and normative influence.

Theme 2: network social support is related to health goals and overall postpartum health
The theme Network social support is related to health goals and overall postpartum health helps to elucidate the different types of social support participants received, as well as the ways in which the support contributed to overall health. Social-support types were organized into (1) appraisal support, (2) companionship support, (3) emotional support, (4) informational support, and (5) instrumental support.
Appraisal social support
Appraisal support was defined as information or actions provided by a network member that were used by a participant for self-evaluation and perspective. For qualitative-coding purposes, appraisal support was illustrated as a network member helping the participant to realize something or helping the participant to talk through something in order to find a solution. Through qualitative coding, participants’ appraisal support was found to be supportive of health behaviors, mental health and well-being, and parenting. The following quote provides an example of the intersection of these three support areas:
[My coworker] sets a good example of self-care and self-compassion. She’s very good at managing her day. That provides a sense of hope for me. Her kid is a little older and so that’s reassuring, that although I may not be hitting my goals right now, I probably will be able to in a couple of years. (Participant 81; returned to pre-pregnancy weight; non-Hispanic/Latino, White; personal social-network survey response)
Appraisal social support for health behaviors
Participants engaged in conversation with network members (i.e., other mothers, siblings, partners, parents, friends, and a personal trainer) about their health goals in order to support long-term health and avoid illness. Together, they made decisions about how lifestyle changes could be made and how they could support mutual accountability. Appraisal support also helped participants to feel reassured when realizing they were not alone in their weight struggles, consumption of convenience foods, and periods of inactivity. Eight participants talked about appraisal support for physical activity. Network members helped participants realize, for example, that gym attendance was possible despite full-time work and motherhood responsibilities. They also helped participants to mentally shift the desired outcome of gym attendance from weight loss to gaining strength. Additionally, network members helped participants to problem-solve barriers to physical activity, such as unfamiliarity with a neighborhood and ways in which to be active with children. Dietary appraisal support facilitated participants’ self-reflection and insight. For example, network members helped participants to reconsider healthy portion size and nutritional changes to diet. They also helped participants gain perspective on poorer dietary habits that were learned earlier in life.
Appraisal social support for mental health and well-being
Network members (i.e., friends, therapists, partners, and siblings) helped participants to gain perspective on this stage of their lives. They provided reminders for actions participants could take to support their mental well-being (e.g., breathing, yoga, visiting a therapist). They also helped participants to evaluate previous mental-health struggles (e.g., postpartum depression) and provided suggestions that would support mental health during participants’ current postpartum period.
Appraisal social support for parenting
Network members (i.e., friends and family members who were mothers) helped participants to gain perspective on their concerns for their children (e.g., raising an only child, developmental delays) and postpartum experiences. They also provided reassurance that participants were good mothers despite the turbulent nature of raising children. See Table 7 for additional appraisal support quotes.
Appraisal support participant quotes.

Companionship social support
Companionship support was defined as time spent engaging with others. For qualitative-coding purposes, an example of companionship social support was co-engagement in group activities that would contribute to the participant’s sense of belonging. Participants’ companionship support, identified through qualitative coding of interview data, included shared physical activity, eating together, and companionship generally.
Companionship social support for health behaviors
When talking about physical activity in general, women talked about the active lifestyles of their partners, friends, siblings, and parents. Engaging with these network members motivated the participants to want to “keep up” and provided them with additional opportunities to be active. Examples of workouts and gym attendance included co-engagement in fitness, martial arts, and yoga classes; attending the gym together; lifting weights together; and working out at home together. Participants said co-engagement in workouts with their friends, partners, and siblings helped them to remain motivated, especially when considering that they had an accountability partner. Last, examples of outdoor activities included hiking, walking, running, biking, skiing, snowshoeing, and playing sports (e.g., pickleball, softball, soccer). Participants said engaging in shared outdoor activities with family and friends was more fun than doing it alone, and that it was enjoyable to “get fresh air.”
Companionship support for eating and dietary behaviors included supporting each other’s healthy dietary choices, sharing healthy meals together, meal planning, and recipe sharing. Participants said this support helped them to make healthier choices. Additionally, one participant said the support enabled her continuing engagement in healthy eating:
If I have a good group of similar people, such as parents with small children, that can . . . [support] healthy-lifestyle choices, such as meal-prepping, recipe-sharing, etc., I am more willing and able to do those things. If I have to do it alone, I find it a bit overwhelming and stressful, and sometimes put it off completely. (Participant 27; retained postpartum weight; non-Hispanic/Latino, White; individual-factors survey response)
Companionship social support for companionship in general
Companionship support in general included regularly spending time together, attending family gatherings, talking with other moms about “mom life,” having playdates for children, spending time with friends, and talking with friends and family by audio or video calls, or through social media. Participants said being around other people supported their mental health and helped strengthen social bonds. One woman said that family gatherings not only provided company but also supported physical activity:
And as far as health, we have a very active heritage, meaning that at parties, there’s music, there’s dancing. And the dancing isn’t just for 30 minutes. It’s for a while. So that’s nice. When there’s get-togethers and I’m able to be with my family, I can always expect, you know, to have parties and dancing. (Participant 58; retained postpartum weight; Hispanic/Latino, White; in-depth interview response)
Please see Table 8 for additional companionship support quotes.
Companionship support participant quotes.

Emotional social support
Emotional support was defined as expressions of empathy, love, trust, and caring. For qualitative-coding purposes, examples of emotional social support were, “I talked and they listened,” “they were there for me,” “they encourage me to exercise,” and “they encourage me to eat well.” Emotional support provided by network members was operationalized through means such as aligning on goals, being a “cheerleader,” helping the participant to “stay on track” with their goals, pushing the participant to “go farther,” complimenting and recognizing progress made toward goals, checking in on or reaching out to the participant, offering a listening ear, allowing the participant to talk and vent, relating to one another, and being a constant presence on whom the participant could lean. Participants’ emotional support was for the purpose of supporting health behaviors and weight, the perinatal period, and mental health and well-being.
Emotional social support for health behaviors and weight
Participants said they appreciated network members who both encouraged health behaviors and supported their suspension of health-behavior goals when they were too tired or overwhelmed by motherhood responsibilities. Some participants talked about the motivational benefit of mutual engagement in health goals. Participants and their network members (i.e., partners, siblings, friends, and a cousin) would check in with each other (via phone, linked smart watch, or in person) to update goals and track their progress. They also talked about physical activity, diet, and meal planning, as well as the importance of finding balance. A few participants said their healthcare providers approached the topic of weight sensitively and provided reassurance that the participants’ efforts were recognized. For physical activity, participants said they were encouraged to engage in physical activity with their network members (i.e., partners, siblings, friends, parents, and a trainer) and felt motivated even on days they did not feel like being physically active. Last, when providing emotional support for diet, some participants said they were encouraged to eat a balanced diet and increase their vegetable and water intake. Parents, siblings, partners, and friends provided this dietary support.
Emotional social support for the perinatal period
Some participants talked about the emotional support provided by their partners, such as a mutual appreciation for co-parenting which had brought them closer together. Usually, participants talked about friends or family members who were also mothers. Participants felt safe talking about motherhood with these network members and expressed the relief they felt to have someone with whom they related. A couple of participants said their friends who were mothers provided emotional support for role-modeling of healthy behaviors for their children and also for setting goals so as to be healthier for their children.
Emotional social support for mental health and well-being
Participants said they felt safe going to network members (i.e., parents, a grandmother, friends, therapists, a doctor, a cousin, siblings) when they were stressed or struggling, and that network members routinely checked in with them to see how they were doing. These network members helped to motivate participants to engage in activities that would support their mental health (e.g., getting rest, seeing a therapist, meditating). See Table 9 for quotes about emotional support.
Emotional support participant quotes.

Informational social support
Informational support was defined as advice, suggestions, and information provided by network members, such as the provision of health advice. Participants’ informational support, identified through qualitative coding, included information for parenting, health, health behaviors, and weight and body image.
Informational social support for parenting
Informational support was provided by friends, family, and community members who were also mothers. These network members provided suggestions for helping children to sleep, childhood development, caring for sick children, breastfeeding, and postpartum recovery.
Informational social support for health
Network members (i.e., doctors, nurses, friends, and parents) provided information to educate participants about the importance of tending to personal health, and reminding participants that they should maintain their health in order to enable them to care for their child(ren). Network members talked about routine check-ups, how to maintain and improve health, and how to avoid illnesses that network members were struggling with.
Informational social support for health behaviors
For physical activity, network members (i.e., friends, siblings, doctors, parents, a cousin, and a personal trainer) provided resources such as written exercise routines or links to exercises. They also gave advice for physical activity frequency and duration, and information about engaging in physical activity during pregnancy and the postpartum period. For dietary informational support, a wide range of network members (i.e., doctors, partners, siblings, cousins, parents, friends, neighbors, a WIC nutrition coordinator, a niece, and a nephew) offered nutritional advice, including nutritional support for breastfeeding and children’s diets. They also made recommendations to eat less sugar, eat more vegetables, and drink more water. Network members were a resource to participants for cooking advice, recipes and meal plans, and for the tailoring of meals participants found appealing so that they included healthier ingredients. Last, in addition to talking with participants, network members shared these dietary resources through TikTok, YouTube, and email.
Informational social support for weight and body image
Healthcare providers educated two participants about how weight factored into health conditions (i.e., back pain, gestational diabetes). Both women thought this information was appropriate, helpful, and non-offensive. Several more participants discussed suggestions their network members had provided for weight loss (e.g., “eat better,” a weight-loss app) and for body image (i.e., the book More Than a Body 51 ). This last participant said her sister-in-law shared information through blog posts and conversations that would help her to accept the childbearing-related changes to her body. See Table 10 for quotes about informational support.
Informational support participant quotes.

Instrumental social support
Instrumental support was defined as the tangible, practical aid and services that were provided by network members, such as childcare or food. Participants’ instrumental support, identified through qualitative coding, was for physical activity and the postpartum period.
Instrumental social support for physical activity
A majority of participants said they primarily relied on their partners to watch their child(ren) so that they could be active. Often participants said they and their partners were dependent on each other in order to have time away to engage in physical activity. This was not always easy to coordinate, as partners and the participants had multiple responsibilities that often took priority over physical activity. Parents and in-laws were also named as people who provided childcare so that participants could be active. Other forms of instrumental support for physical activity included network members paying for participants’ gym memberships and allowing participants to use their home workout equipment.
Instrumental social support for the postpartum period
While a couple of participants said meals were provided by friends and family in the early postpartum weeks, several participants talked about the supportive nature of the more thorough instrumental aid they received in the early weeks and months of the postpartum period. The participants’ parents provided this support in the form of preparing meals, household cleaning, and assistance with child-care needs. One participant illustrated the comprehensive nature of the instrumental support she received from her mother postpartum:
The first few months postpartum were amazing because, as hard of a time that it is, my mom made me a new super-healthy meal every day. And an example is in the morning she had fresh-squeezed orange juice. For lunch, chicken salad with arugula, walnuts, like just the whole nine yards. Dinner, you know, a nice dinner for my husband and I. And I felt so well fed, I felt so nourished. And that is part of our culture, because we really respect those first 90 days after postpartum. You know, making sure the house was clean. I don’t know how she took care of the baby, made dinner, and the house was clean. And took care of me because I would sleep a lot since the baby’s awake at night. You know, with their hours mixed up. I would sleep a lot during the day and just not get any notion of when she did any of this, but it was like a fairy came to my house. (Participant 58; retained postpartum weight; Hispanic/Latino, White; in-depth interview response)
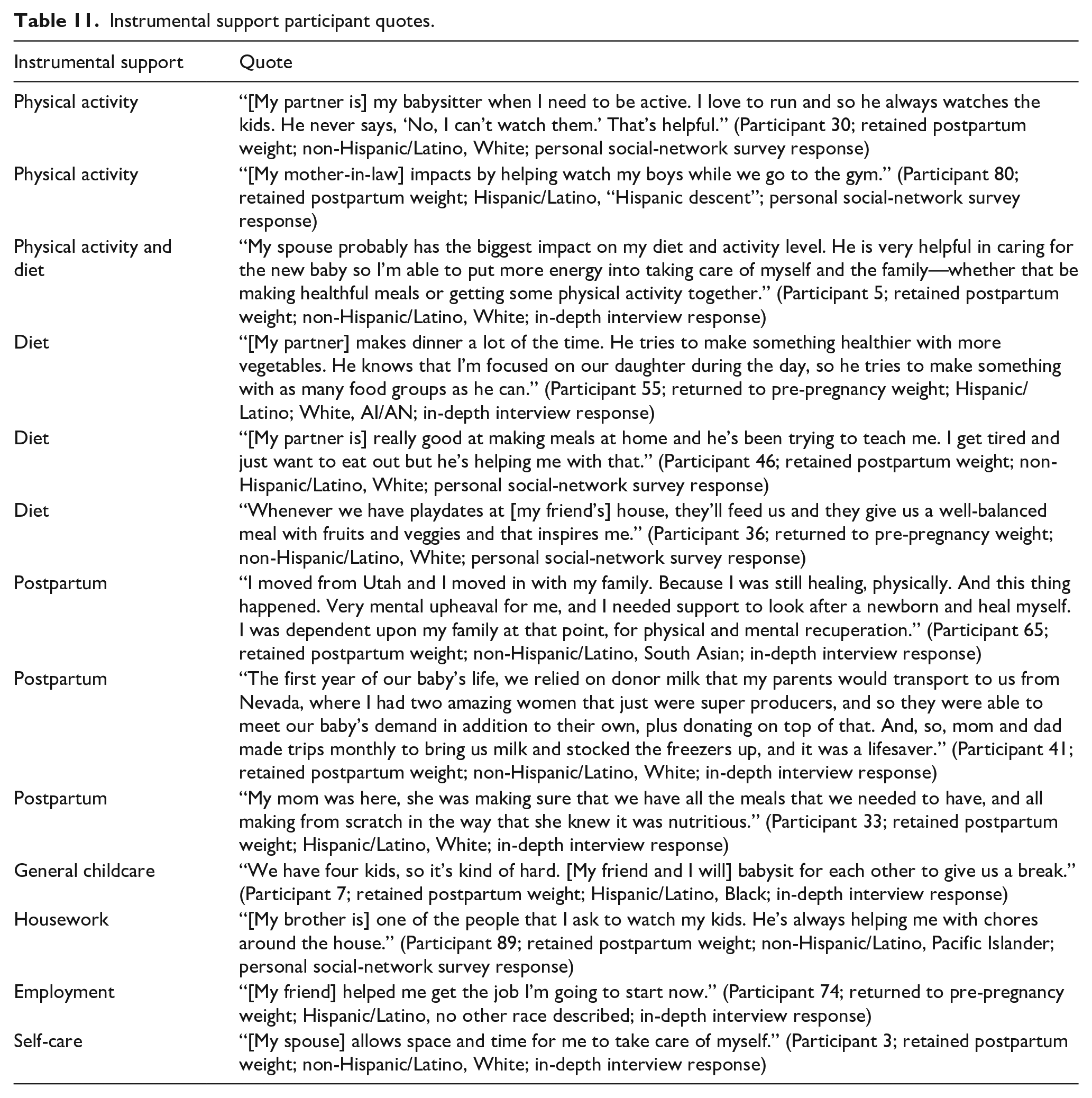
Please see Table 11 for additional participant quotes about instrumental support.
Instrumental support participant quotes.
Discussion
Our aim was to gain additional understanding about postpartum people’s perceptions of the relationship between their social networks and support, and their health behaviors and weight. The postpartum year is a window of opportunity to help support postpartum people in their healthy-behavior efforts and to disrupt the weight gain across the lifespan that is associated with childbearing. As was found among this sample of postpartum women, there is interest in making improvements to dietary behaviors so as to support their families’ long-term health. There is also interest in increasing physical activity and achieving a healthy weight in order to keep up with children’s active lifestyles and to support long-term health so that they can be active participants in their families’ lives well into the future.
Normative influence on health behaviors
To our knowledge, this is the first qualitative study that has sought to understand postpartum people’s experience of their social networks in relation to their health behaviors and weight. We learned that social engagement and the shared consumption of food often went hand in hand for this sample of women. Within the household, partners were often identified as central to both healthier and unhealthier dietary norms. Partners could help support healthier dietary norms through their preference for healthier ingredients. They could also support unhealthier norms through preferences for treats, snacks and convenience foods, and the facilitation of social eating, despite a lack of hunger. This latter finding is supported by a quantitative study by de Castro that investigated meal companionship and dietary intake over the course of a week; the presence of male eating companions was found to facilitate increased consumption among females. 52 Additionally, qualitative investigation has confirmed the barrier to healthy eating among postpartum women by their making treats and convenience foods available in the home in order to support partners’ food preferences.18,34
Just as shared eating was viewed as a social activity, participants’ increased level of physical activity was often attributed to social engagement. Participants said they matched their level of physical activity to network members, which sometimes resulted in participants pushing themselves physically in order to keep up with their network members. An increase in physical activity was reinforced for participants who used social selection of network members for those network members’ higher level of physical activity. As found in previous research by Sanderson et al., the participants’ children were seen as both motivators and barriers to physical-activity engagement. 53
Normative influence on weight
Participants were aware of a dichotomy related to postpartum weight. On one hand, there was familial, cultural, and societal pressure to “bounce back.” On the other hand, sometimes family members would discourage participants from being concerned about their weight and encourage them to take it easy, even after participants felt ready to increase their physical activity and lose weight. This type of network discouragement was also qualitatively identified by Hanley et al. among a sample of postpartum women who were overweight or obese. 54
Participants said there were conflicting and often confusing social-media messages about weight, body image, and body positivity. Additionally, participants’ mothers could sometimes be overly preoccupied with weight. In these instances, participants often said this preoccupation of their mothers could negatively impact their diets and levels of activity. For this reason, one participant made clear her belief that not all social intervention is positive, even if it results in weight loss, as it might also cause poorer mental health and a damaged relationship with one’s body.
Familial norms of weight also impacted participants’ beliefs about weight and their health behaviors. This was discussed in relation to a process of healing damaged ideals about body image, food, and physical activity. It was also described as participants’ processes of realization about family norms for overweight, which then motivated the participants’ commitment to health through healthier behaviors than those that had characterized their childhood family environments. Several participants talked about how social support could help buffer the unhealthier network norms related to weight. This support was in the form of friends and partners who helped to buffer pressures from societal norms and the participants’ mothers’ unhealthier dietary and weight beliefs. The result of this support was enhanced body image and acceptance of changes in participants’ bodies as a result of childbearing.
Last, several women of this study described experiences of weight stigma within the healthcare setting that impacted their mental well-being. These participants believed discussions of postpartum weight should be addressed with sensitivity. A qualitative study by Jensen et al. with a sample of postpartum women who were overweight and obese also identified healthcare providers as contributing to women’s experiences of weight stigma. 55 One participant of the Jensen et al.’s study described the sensitive approach of a nurse who helped to put the participant’s vulnerability toward her weight to rest by focusing on her as an individual and providing tailored education. Instead of focusing on the participant’s gestational weight gain, the nurse provided practical advice that addressed the participant’s individual needs. The finding of this former qualitative study provides helpful direction for sensitive postpartum healthcare. The importance of sensitive postpartum care is underscored by the results of a longitudinal correlational study that found that healthcare providers are influential in postpartum women’s health-behavior decision-making. 56 Ohlendorf et al. recommend that healthcare providers harness the postpartum period as an opportunity to assist women in healthy-behavior change. 56
Social support
This study contributes to the limited body of literature that has investigated postpartum social support and its impact on postpartum health behaviors. In this study, social support was organized by the following types: (1) appraisal support, (2) companionship support, (3) emotional support, (4) informational support, and (5) instrumental support. This is notable, because the delineation of social-support types contributes to our understanding of the ways in which functional social support contributes to postpartum people’s health behaviors. Delineation of social-support types has rarely been the focus of research among postpartum samples.
Research suggests that a particularly salient source of social support regarding postpartum weight issues seems to come from other postpartum people who have had similar experiences. Our study lends additional evidence to this premise. We found that network members who were also mothers provided emotional and informational support in safe ways that helped participants to gain acceptance of bodily changes due to motherhood. Literature reveals that support from those with shared experiences also helps postpartum people to recognize that they are not alone in their struggles with weight during the postpartum period.32,34
Study limitations
Study limitations include the primary investigator’s White race and non-Hispanic ethnicity. For the participants of this study who were not White or who were of Hispanic ethnicity, this may have limited their level of comfort with disclosure of personal responses to the study’s open-ended questions. This, in turn, may have restricted the qualitative findings of this study. Trustworthiness measures were addressed prior to the initiation of each phase of the study in an attempt to address this limitation.
Second, this study recruited only postpartum people who could speak English. This is a limitation of the study that limits generalizability. Future studies should investigate this topic through community-engaged approaches to understand unique needs of postpartum people from specific communities.
Future directions of study
The study’s findings contribute to knowledge about how social networks impact postpartum health behaviors and weight so that this information can be incorporated into future interventions. Understanding characteristics of postpartum people’s social networks and their association with their health behaviors and weight will provide foundational evidence to inform interventions. Such interventions could incorporate social-network components, for example, assisting postpartum people to identify resources for healthy behaviors within their networks, identifying network members who act as barriers to healthy behaviors, and identifying network limitations as opportunities to enhance support. This could help address issues relating to the social context in which people experience postpartum weight loss or retention and related health behaviors. 57
Conclusion
The complex problem of supporting postpartum health behaviors and healthy weight requires approaches that consider multiple levels and domains of health. Participants in this study reported numerous ways in which their social networks both supported and hindered their healthy-lifestyle efforts. The insights we identified suggest more research on the social context is warranted to develop effective programs and interventions that support postpartum and family health.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241309774 – Supplemental material for “Listening to understand,” exploring postpartum women’s perceptions of their social networks and social support in relation to their health behaviors and weight: A qualitative exploratory study
Supplemental material, sj-docx-1-whe-10.1177_17455057241309774 for “Listening to understand,” exploring postpartum women’s perceptions of their social networks and social support in relation to their health behaviors and weight: A qualitative exploratory study by Jacqueline Kent-Marvick, Kristin G Cloyes, Ana Clark, Monica Angulo, Kayla de la Haye, Michelle Precourt Debbink, Cristina Creal, Bob Wong and Sara E Simonsen in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241309774 – Supplemental material for “Listening to understand,” exploring postpartum women’s perceptions of their social networks and social support in relation to their health behaviors and weight: A qualitative exploratory study
Supplemental material, sj-docx-2-whe-10.1177_17455057241309774 for “Listening to understand,” exploring postpartum women’s perceptions of their social networks and social support in relation to their health behaviors and weight: A qualitative exploratory study by Jacqueline Kent-Marvick, Kristin G Cloyes, Ana Clark, Monica Angulo, Kayla de la Haye, Michelle Precourt Debbink, Cristina Creal, Bob Wong and Sara E Simonsen in Women’s Health
Footnotes
Acknowledgements
We are appreciative of our community advisory board members’ time, guidance, and their commitment to the health and well-being of the postpartum population. Last, we are thankful to our study’s participants for their collaboration on and interest in this research topic.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.