
Abstract
Background
Preeclampsia is an independent risk factor for vascular diseases. The Postpartum Preeclampsia Clinic (PPPC) intervenes in the first year postpartum to address these risks. This study aims to characterize physicians’ understanding and management of the cardiovascular risk associated with preeclampsia and whether this differs in physicians who had a patient attend the PPPC.
Methods
Family physicians, obstetricians, internists, obstetric internists, and cardiologists in Edmonton were anonymously surveyed. Results were analyzed using SPSS.
Results
Sixty-four surveys were returned, with physicians correctly identifying preeclampsia as a vascular risk factor 73% of the time. Physicians who had a patient attend the PPPC were more likely to counsel patients on their increased cardiovascular risk, although increased knowledge did not reach statistical significance.
Conclusion
Vascular risk reduction clinics may benefit the long-term management of patients with a history of preeclampsia by improving counseling by physicians, which may reduce the disproportionate vascular morbidity these patients face.
Background
Cardiovascular disease (CVD) is the leading cause of death globally. 1 Recently, hypertensive disorders of pregnancy (HDP), such as preeclampsia, have been established as an independent risk factor for CVD.2–14 HDPs occur in approximately 10% of pregnancies and are a leading cause of maternal mortality.4,15 Preeclampsia and CVD share many common risk factors, including obesity, dyslipidemia, and hypertension.4,5,13 However, preeclampsia further increases the risk of CVD beyond these existing factors. 16 Preeclampsia has been shown to increase the risk of heart failure by 4-fold, ischemic heart disease by 2-fold, and chronic hypertension by 3.7-fold.6,7 This risk is further increased in patients with recurrent or early onset preeclampsia.8,9,14 Strikingly, a Canadian study found that patients with a history of preeclampsia have double the risk of premature cardiovascular disease. 10 Further, they have their first cardiac event at a mean of 38 years old, an average of 10 years after the diagnosis of preeclampsia.
Pregnancy should be considered a stress test for future CVD, where the development of preeclampsia should prompt postpartum intervention.2,9,12,14 Lifestyle changes, such as diet, exercise, smoking cessation, and weight loss, have been shown to be effective for postpartum CVD risk reduction.16,17 However, current national and international guidelines on the long-term management of preeclampsia lack concrete recommendations.4,5,18–21 This makes the application of these guidelines highly dependent on individual clinician interpretation. Currently, some patients with a history of pre-term preeclampsia are managed in specialist clinics, such as the Postpartum Preeclampsia Clinic (PPPC), which was established in 2010 and was one of the first clinical vascular interventional clinics of its kind, at the Royal Alexandra Hospital in Edmonton, Canada. The PPPC led by an obstetric internist educates patients about their vascular risks, with a focus on cardiovascular risks, which share many of the same factors as cerebrovascular and renovascular diseases. CVDs are also generally more easily understood by patients, and their association with HDPs is better studied. The PPPC manages the patients’ blood pressure and cholesterol and empowers them to make lifestyle changes, such as weight reduction, dietary changes, and increasing exercise. Patients also measure hemoglobin A1C and are assessed for resolution of proteinuria or any abnormal labs, such as liver enzymes or renal function. Early data of the PPPC intervention showed significant improvement in exercise uptake. 22 Following clinic attendance, patients are discharged to their primary care providers, who are provided letters outlining the recommended type and frequency of screening and management of vascular risk factors, including checking blood pressure and diabetes every year, checking lipids every 1–3 years, encouraging a heart-healthy diet, aerobic exercise of moderate intensity, not smoking, and repeating proteinuria assessment if not normalized. Notably, our patient-reported study showed that patients who attended the PPPC were more likely to follow-up with their family physicians for vascular risk reduction. 23
Specialized clinics, such as the PPPC, do not have the capacity to see all patients with a history of preeclampsia. A recent provincial database study reported preeclampsia rate at 2.5%, with a rising trend in the last two decades. In our zone that has over 12,000 births a year, our twice a month half-day PPPC cannot accommodate the volume of patients. Further, preeclampsia has a higher incidence in certain ethnic populations. A Canadian study demonstrated that patients who immigrated from the Caribbean, Sub-Saharan Africa, and Hispanic America are particularly at risk, 24 making services that enhance access to care for these populations critical, not just in Canada, but in the global majority. Given the limited capacity of specialized clinics, in our region, patients may see obstetricians, obstetric internists, or family physicians in the immediate postpartum period and family physicians or general internists for long-term follow-up. However, it is not clear how much physicians know about the elevated CVD risk following preeclampsia and how they manage these patients clinically. The aim of this study is to evaluate the knowledge and clinical management of physicians related to the long-term health risks of preeclampsia, with the primary objective to examine whether these differed in physicians who had a patient attend the PPPC.
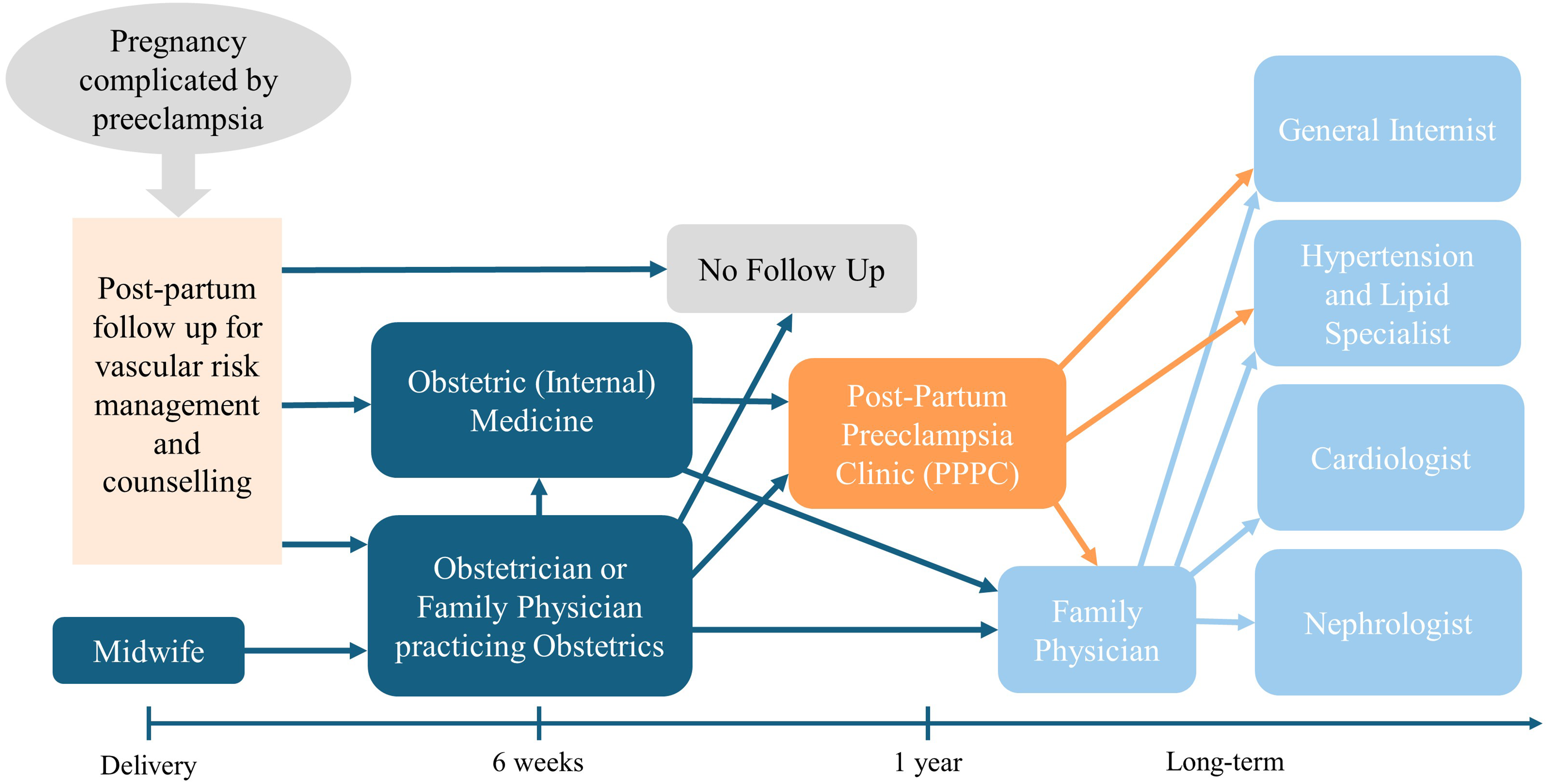
Regional referral pathways for post-partum follow-up for vascular risk reduction and counseling after a pregnancy complicated by preeclampsia.
Methods
Participant selection
Survey responders included physicians in Edmonton, Alberta who may refer to the PPPC, might have received consultation letters, or may be referred to from the PPPC clinic. Selected family physicians were identified and faxed using the PPPC (n = 181) and obstetric medicine (n = 178) clinic letter databases. Obstetricians (n = 76) whose clinic fax addresses were listed on the College of Physicians & Surgeons of Alberta website were faxed the survey. Internists, including obstetric internists and hypertension and lipid specialists (n = 141), and family physicians with a hospital-based practice, including those who practice obstetrics (n = 100), were emailed through the Edmonton Zone physician leads. Given that CVD is the main vascular risk counseled in the PPPC, cardiologists (n = 80) were also surveyed via clinic fax numbers listed on the College of Physicians & Surgeons of Alberta website. It was unclear how many physicians would have received the survey request as physicians might have retired or relocated; there were multiple physicians per office, and the faxes may been screened by reception staff; and the study took place during the summer months when many physicians take vacation. Hence, the exact sample size for this study cannot be determined a priori.
Survey
A survey was created on the REDCap Database to assess knowledge and management of patients with a history of preeclampsia (Appendix A). The survey included demographic, knowledge, and management questions. Because there is no validated survey for this topic, our survey used a question matrix based on the studies of Young et al. 25 and Roth et al. 26 The survey required respondents to identify preeclampsia as a risk factor for lower life expectancy, hypertension, stroke, ischemic cardiovascular disease, and renal disease. Respondents were also asked to identify that preeclampsia has not been implicated as a risk factor for liver disease and malignancy at this time. The management section of the survey required respondents to rank how often they ask about pregnancy complications on general history, counsel patients with a history of preeclampsia on their increased CVD risk, how to reduce this risk, and follow-up with these patients. Management practices were ranked on a four-point Likert scale of rarely, less than half the time, more than half the time, and almost all the time. Unique to our survey were questions exploring the utility and learning from discharge letters sent by the PPPC to physicians who had a patient attend the clinic. The survey was tested in a small sample of physicians and researchers who provided feedback on the accuracy of content, clarity of questions, and organization of the survey prior to the start of the study. The survey was then distributed as a QR code using the abovementioned fax and email lists from June to September 2022. Responses were collected anonymously on the REDCap Database. Consent was implied when participants submitted their response. Two reminders to complete the survey were sent by fax, and one reminder was sent to internists by email. Ethics approval for the study was obtained from the University of Alberta (Pro00092260).
Data analysis
Data from the REDCap database were used for statistical analysis. Descriptive statistics were calculated as frequency and percent for categorical variables. For the primary analysis, the knowledge and management of physicians who had a patient attend the PPPC were compared to those of physicians who did not. Responses to knowledge questions were expressed as correct scores (out of 8 questions) and converted to a percentage. Mann–Whitney tests were then used to compare knowledge between groups of physicians. For management questions, a four-point Likert scale was used as a measure of frequency. The four-point Likert scales were converted into binary categories of performing a practice more than half the time versus less than half the time. Binary logistic regression was then used to estimate the odds of performing a management strategy more than half the time between providers who had a patient attend the PPPC and those who did not. Physicians who responded “rarely, if ever” to whether they ask about preeclampsia on history were assumed to perform management practices less than half the time.
For the secondary analysis, knowledge and management were compared between physician specialties, practice type (hospital versus community-based), and familiarity of managing patients with preeclampsia. For frequency of managing patients with a history of preeclampsia, responses were collected on a five-point Likert scale, which was converted into a binary scale of “frequently” and “infrequently” for analysis. Responses of “often” and “sometimes” were combined in the “frequently” category, while “every once in a while,” “rarely,” and “never” were combined in the “infrequently category.” Mann–Whitney tests were used to compare knowledge scores as described above. Fisher–Freeman–Halton tests were used to compare the management of the different groups of physicians using four-point Likert scales. Binary logistic regression was also used to calculate if knowledge scores predicted a physician performing a management practice more than half the time. P-value < 0.05 was considered significant. All statistical analyses were performed using REDCap and IBM SPSS Statistics for MacOS, version 29.0.1.0 (IBM Corp., Armonk, NY, USA).
Results
Demographics
Sixty-four survey responses were received. The demographic information of respondents is shown in Table 1. More than half the respondents were family physicians, and more than half identified as female. Most family physicians who responded to the survey were community-based, while most specialists had a hospital-based practice. Of the five family physicians in a hospital-based practice, three (60%) identified being in a primarily medical practice, while two (40%) identified being in a primarily obstetric practice. Of the 14 physicians who recalled having a patient attend the PPPC, four of these physicians were family physicians; five were obstetricians; two were general internists; and three were obstetric internists. Eleven of these physicians recalled receiving a discharge letter from the clinic. Five physicians found the letter very useful, and five found it somewhat useful. One respondent was neutral on the utility of the letter. Thirty-six physicians (56.3%) either have not had a patient attend the PPPC or do not manage patients with preeclampsia. Forty-two physicians (65.6%) reported having a patient that attended an obstetric medicine clinic.
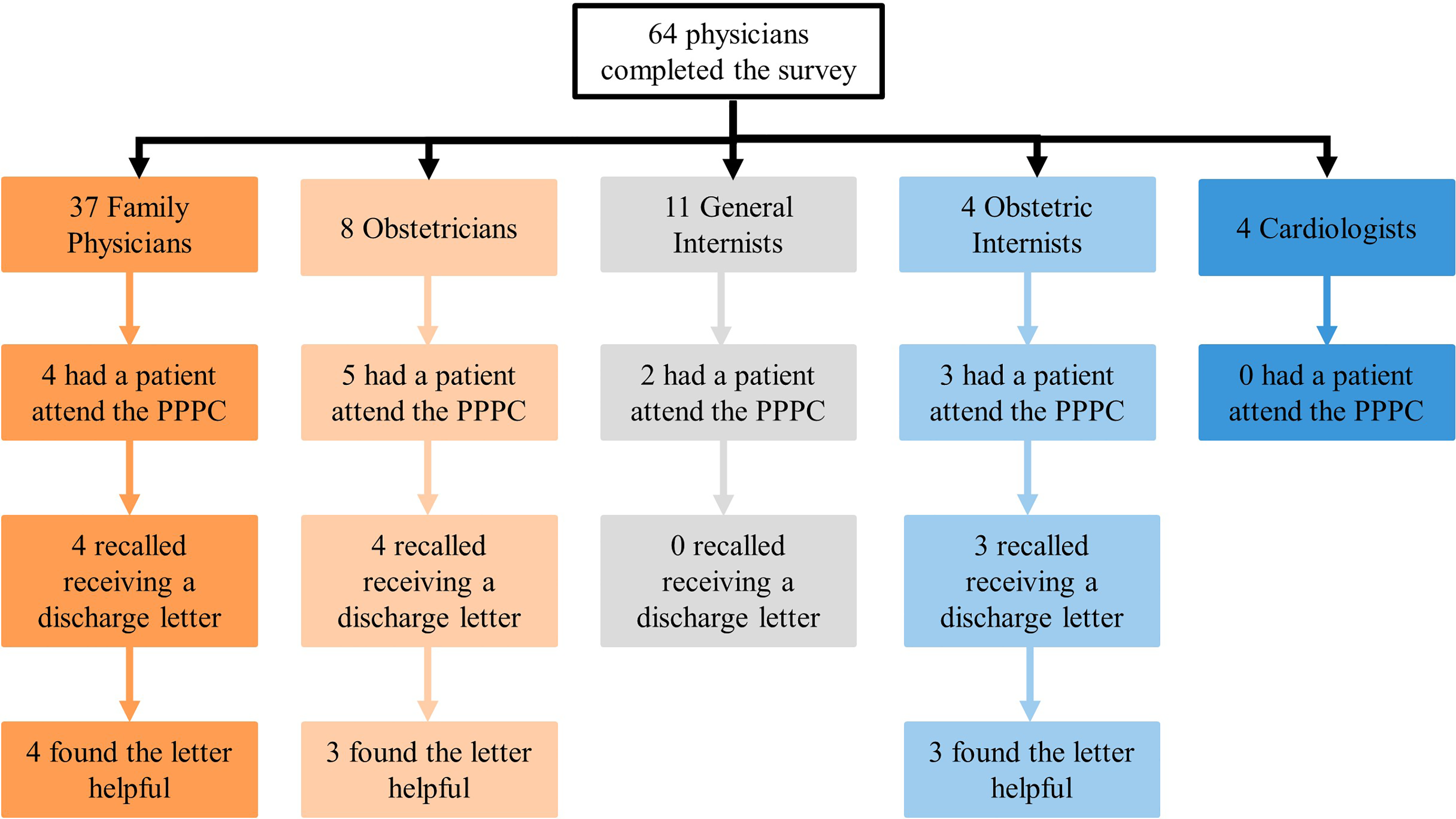
Physician referral to the Postpartum Preeclampsia Clinic (PPPC) and perceived utility of clinic discharge letters based on physician specialty.
Self-reported demographics and knowledge of physician survey respondents.
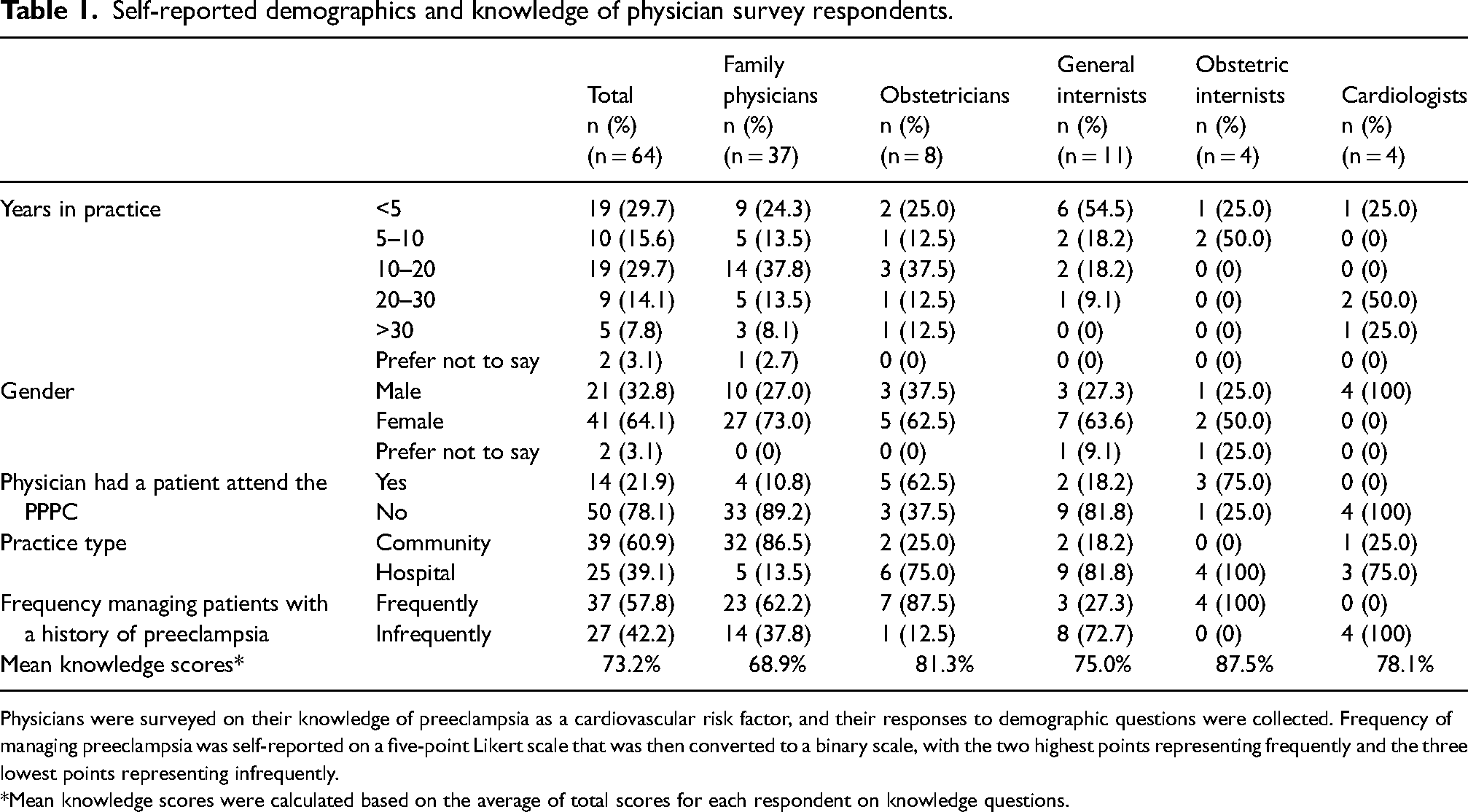
Physicians were surveyed on their knowledge of preeclampsia as a cardiovascular risk factor, and their responses to demographic questions were collected. Frequency of managing preeclampsia was self-reported on a five-point Likert scale that was then converted to a binary scale, with the two highest points representing frequently and the three lowest points representing infrequently.
Mean knowledge scores were calculated based on the average of total scores for each respondent on knowledge questions.
Knowledge assessment
Responses to knowledge questions are summarized in Appendix B. Overall, physicians answered 73.2% of questions correctly. Survey respondents were most aware of the association between preeclampsia and the risk of hypertension and least aware that preeclampsia is associated with a decreased life expectancy. Many respondents thought that preeclampsia increases the risk of liver disease or malignancy, but no such association has been demonstrated at this time.
Physicians who had a patient attend the PPPC scored higher on the knowledge questions than physicians who did not have a patient attend the PPPC; however, this difference was not statistically significant (Table 2). Obstetric internists scored the highest on knowledge questions, followed by obstetricians, cardiologists, general internists, and then family physicians. Altogether, specialists scored higher on the knowledge questions than family physicians, reaching statistical significance. Hospital and community-based physicians scored similarly, as did physicians who identified as managing patients with a history of preeclampsia frequently vs infrequently.
Comparison of the knowledge of preeclampsia as a CVD risk factor between different groups of physicians.
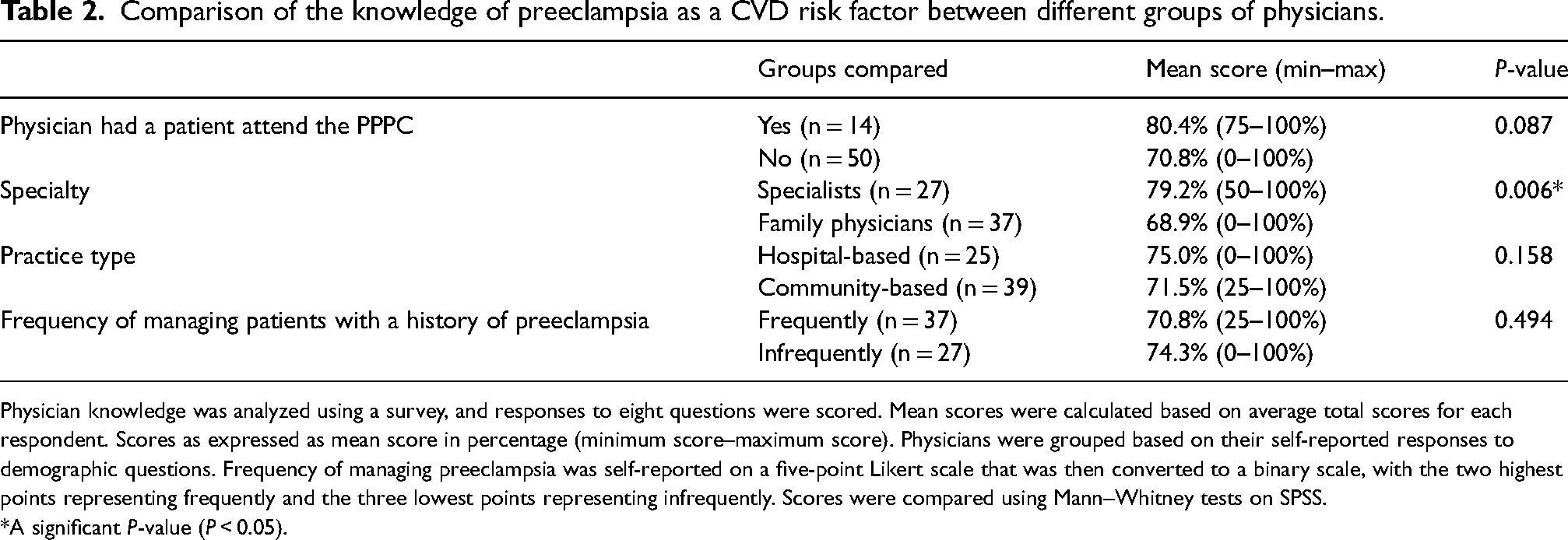
Physician knowledge was analyzed using a survey, and responses to eight questions were scored. Mean scores were calculated based on average total scores for each respondent. Scores as expressed as mean score in percentage (minimum score–maximum score). Physicians were grouped based on their self-reported responses to demographic questions. Frequency of managing preeclampsia was self-reported on a five-point Likert scale that was then converted to a binary scale, with the two highest points representing frequently and the three lowest points representing infrequently. Scores were compared using Mann–Whitney tests on SPSS.
A significant P-value (P < 0.05).
Management assessment
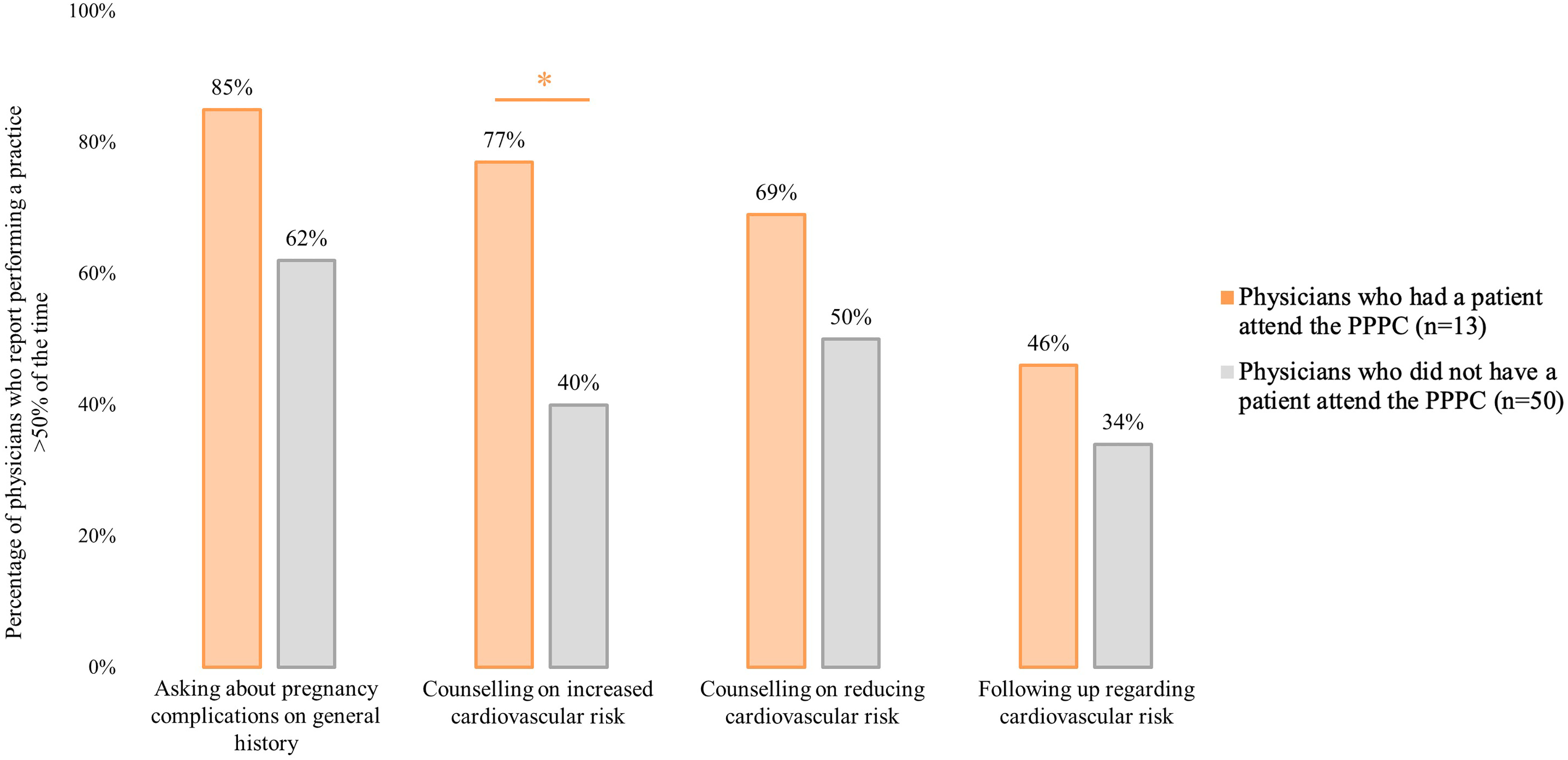
Sixty-three respondents completed the management section of the survey. A summary of the responses to the management questions by these physicians is shown in Appendix C. Physicians who had a patient attend the PPPC reported a higher frequency of counseling on the increased cardiovascular risk associated with preeclampsia (P = 0.025). However, they were not more likely to report asking about pregnancy complications on history (P = 0.139), counseling on reducing the associated risk (P = 0.222), or following-up with patients regarding their risk (P = 0.420).
Management practices of physicians who had a patient attend the Postpartum Preeclampsia Clinic (PPPC) versus those who did not.
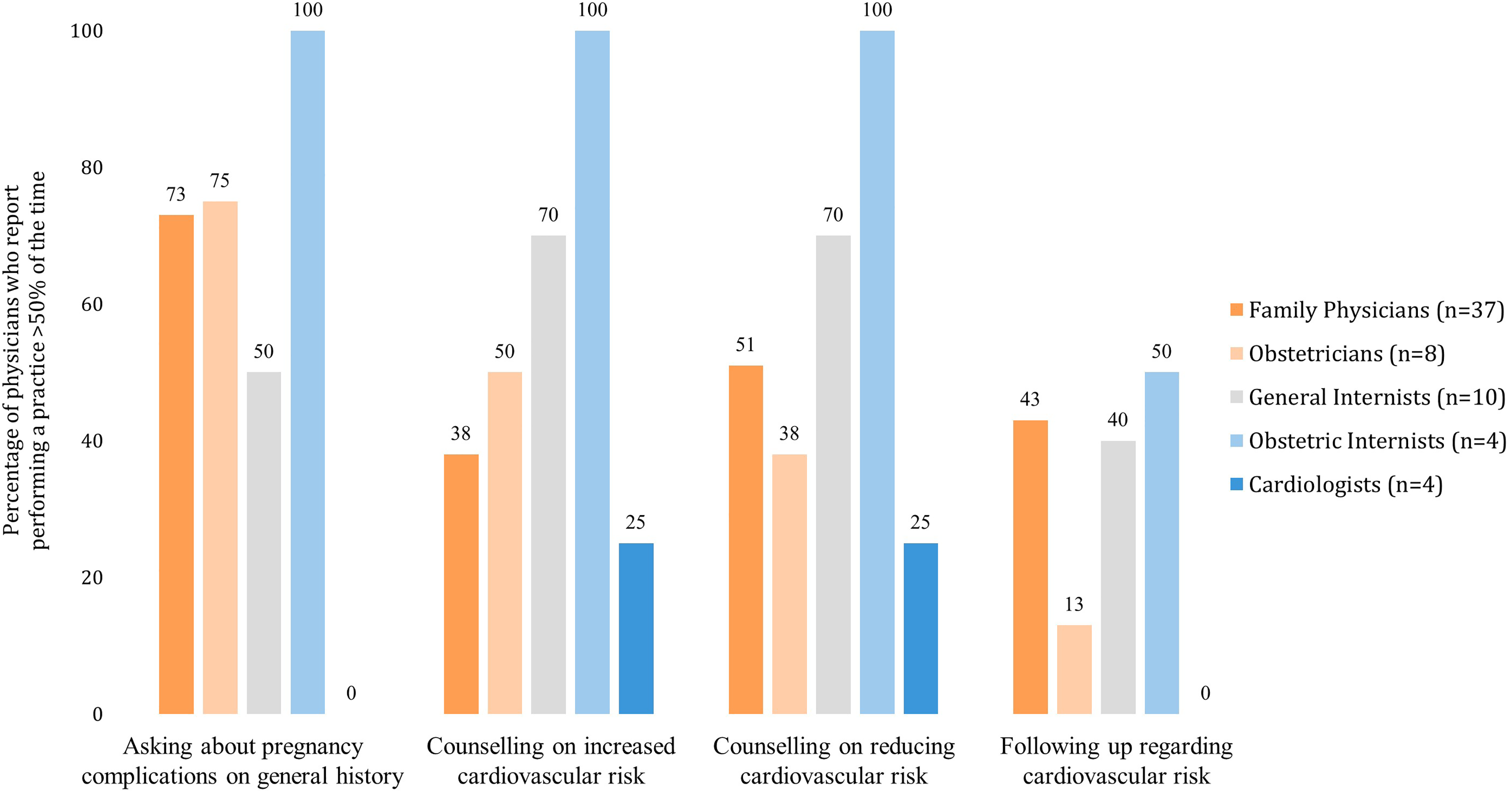
The clinical practices of different groups of physicians are compared in Table 3. Community-based physicians and physicians who manage preeclampsia frequently were more likely to report engaging in risk reducing practices with patients, while physician specialty was only related to likelihood of counseling patients. Obstetric internists were most likely to report that they ask about pregnancy complications when taking a general history, counsel on the increased risk of CVD and strategies to reduce it, and follow up with patients regarding their CVD risk. Family physicians reported one of the highest rates of follow-up with patients, but were less likely to report counseling on CVD. Overall, physicians reported low rates of following-up with patients regarding their risk of CVD. Ten (15.9%) respondents reported never asking about pregnancy-associated risk factors when taking a general history (10.8% of family physicians, 12.5% of obstetricians, 20.0% of general internists, 0.0% of obstetric internists, and 75.0% of cardiologists).
Percentage of survey respondents who reported performing a practice more than half the time.
Comparison of management practices of different groups of physicians.
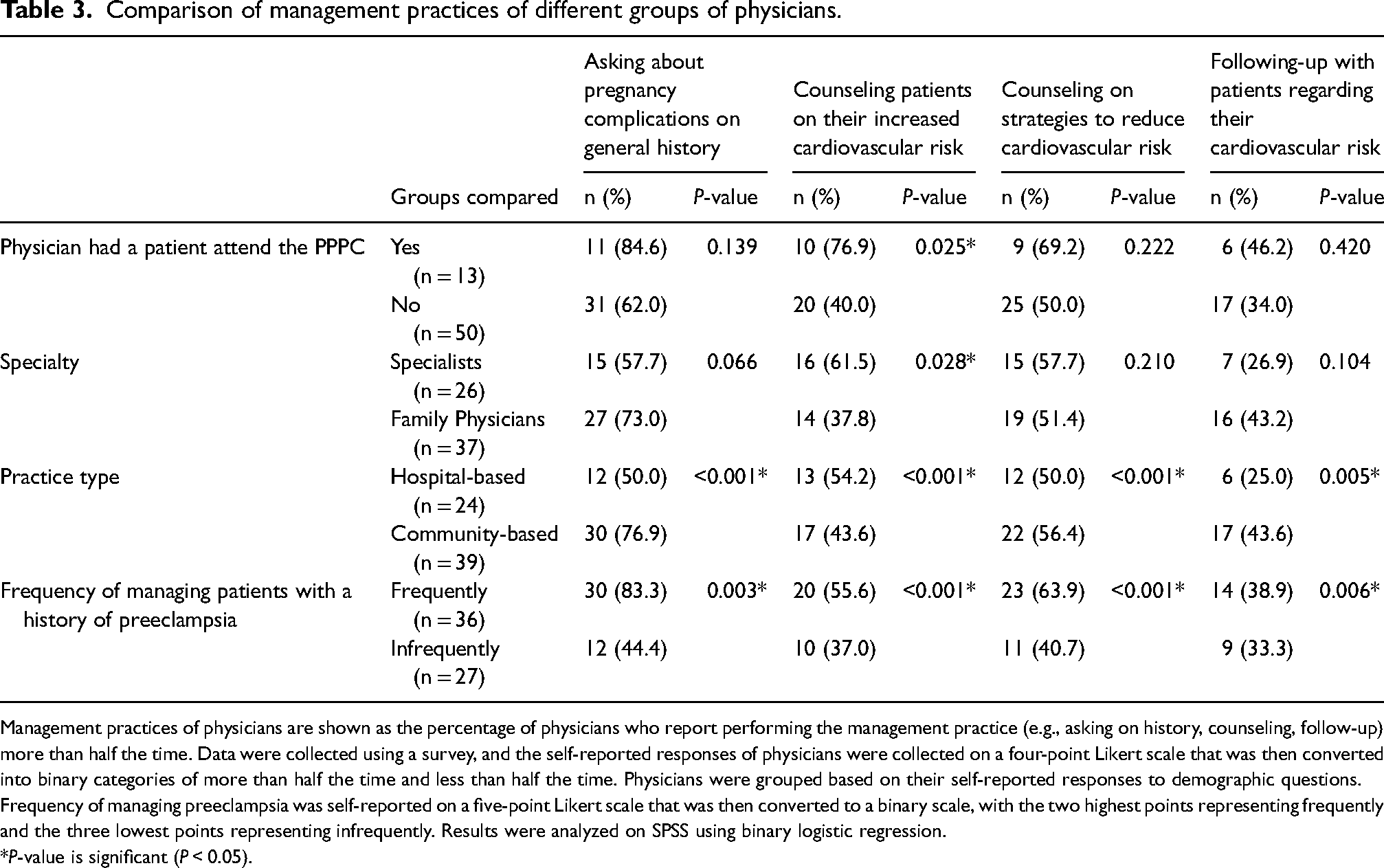
Management practices of physicians are shown as the percentage of physicians who report performing the management practice (e.g., asking on history, counseling, follow-up) more than half the time. Data were collected using a survey, and the self-reported responses of physicians were collected on a four-point Likert scale that was then converted into binary categories of more than half the time and less than half the time. Physicians were grouped based on their self-reported responses to demographic questions. Frequency of managing preeclampsia was self-reported on a five-point Likert scale that was then converted to a binary scale, with the two highest points representing frequently and the three lowest points representing infrequently. Results were analyzed on SPSS using binary logistic regression.
P-value is significant (P < 0.05).
Physicians who scored higher on the knowledge section of the survey were more likely to counsel patients on how to reduce the risk of CVD associated with preeclampsia (P = 0.030). More knowledgeable physicians tended to counsel more on cardiovascular risk, but this difference did not reach statistical significance (P = 0.054). Asking about pregnancy complications on history or following-up with these patients was not associated with knowledge (P = 0.413 and P = 0.707, respectively).
Respondent feedback
Survey respondents were asked about their perception of vascular risk reduction clinics such as the PPPC. Overall, many specialists and Family Physicians alike expressed that cardiovascular risk following a pregnancy with preeclampsia would be better managed in a primary care setting. One family doctor wrote that “for patients who are not attached to a family doctor, [a vascular risk reduction clinic] would be a great idea, otherwise, they should follow up in their medical home.” One general internist noted that they “do not often discuss pre-eclampsia unless relevant to referral question,” but they “do a brief counsel to ensure [the patient is] aware [of the increased cardiovascular risk], and recommend they follow up with their GP [General Practitioner] for screening.” Similarly, an obstetric internist expressed that “a vascular risk reduction clinic is great, but ideally this knowledge and education should be more widely disseminated so that this is offered in primary care since these vascular risk reduction strategies should be lifelong.” Several physicians echoed this need for improved education. One family physician wrote that they “suspect that the increased long-term risks involved with preeclampsia are often missed as both patients and, at times, physicians are unlikely to consider the potential impact decades after the pregnancy.” Another physician noted that a vascular risk reduction clinic “might be good from an education perspective for my patients and particularly for a resource to the community to improve awareness of the significance of the preeclampsia [history] among physicians and patients.”
Discussion
Our study aimed to evaluate whether a physician who had a patient attend a vascular risk reduction clinic, such as the PPPC, had increased knowledge and improved management of the long-term risks of preeclampsia. We found that physicians who had a patient attend the PPPC were more likely to report counseling patients on their increased risk of CVD. They had more knowledge than physicians who did not have a patient attend the PPPC, but this difference did not reach statistical significance. It is possible that this difference is related to referring physicians receiving discharge letters that outline the long-term vascular risks of preeclampsia; however, this should be further evaluated in future studies. Our study also found that specialists had more knowledge than family physicians. Further, community-based physicians reported a higher frequency of performing all the assessed management practices compared to hospital-based physicians. Physicians who were more familiar with managing preeclampsia also reported that they performed the assessed management practices more often. Importantly, our study demonstrated that physicians who had more knowledge about preeclampsia being a CVD risk factor were also more likely to report counseling patients on how to reduce the risk of CVD.
This study demonstrates a critical gap in the knowledge of Edmonton physicians. Many notable long-term effects of preeclampsia, such as decreased life expectancy, were overlooked by survey respondents. This is an important finding because traditional CVD risk calculators do not consider obstetric factors and, thus, may underestimate risk in these patients. 27 It is, therefore, vital that physicians know to account for preeclampsia as an additional risk factor. In light of this study's finding that physicians with more knowledge were more likely to report counseling their patients on the risk of CVD, efforts to educate physicians on the long-term risks of preeclampsia are warranted. This may also be achieved through teaching both at the undergraduate and post-graduate medical education levels, continuing medical education through rounds and conferences, and the development of concrete guidelines.
Community-based physicians, despite having similar knowledge as hospital-based physicians, reported better management practices. This may result from seeing patients in a lower acuity setting or having a greater ability to book follow-up appointments. Physicians who reported managing these patients more frequently also reported better management practices, which is likely due to a higher degree of familiarity.
In the literature, the results of similar studies have been varied. An Australian study reported a similar level of knowledge as was found in this study, with 85% of respondents being aware of the risk of CVD. 26 The participants in this study were mainly midwives and obstetricians, while our study comprised a higher proportion of family physicians. Further, this study did not assess management practices. A German study also corroborated our results that 78–86% of obstetricians knew of preeclampsia's association with various long-term complications, but only 65% counseled on this risk. 28 A Nigerian study of primary care providers found similar knowledge, but with less than of half of respondents counseling on the CVD risk. 29 Several other studies reported fewer physicians asking about preeclampsia on general history, less overall knowledge, and more infrequent counseling.25,29,30 This may be related to the timing of emerging guidelines, as preeclampsia was only officially recognized as an independent CVD risk factor by the American Heart Association in 2011 (Table 4). To that end, a study by Heidrich et al. found that physicians who knew about guidelines related to the long-term risks of preeclampsia were more likely to counsel. 28
Summary of guidelines for the management and screening of the long-term cardiovascular risk of preeclampsia.
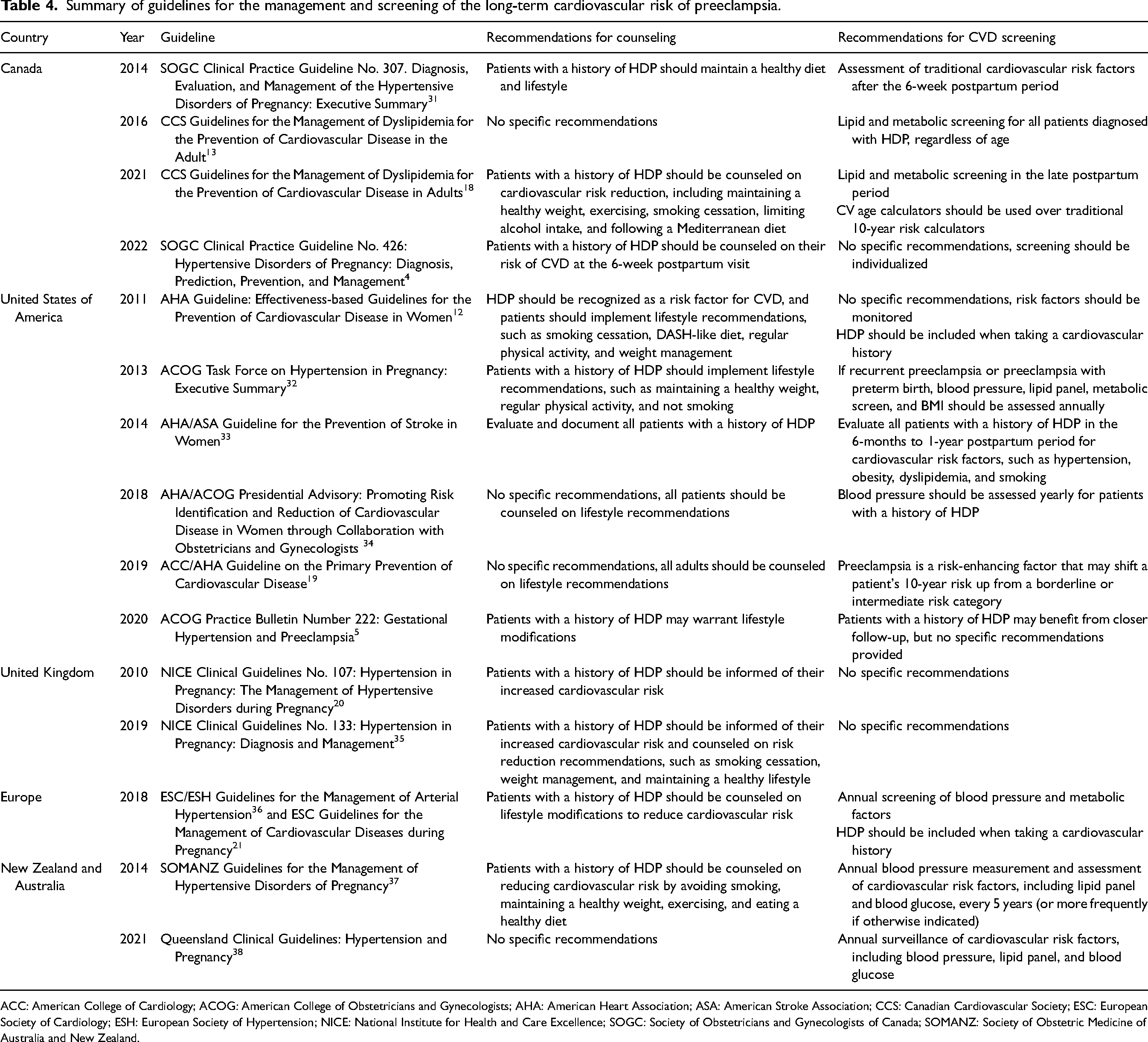
ACC: American College of Cardiology; ACOG: American College of Obstetricians and Gynecologists; AHA: American Heart Association; ASA: American Stroke Association; CCS: Canadian Cardiovascular Society; ESC: European Society of Cardiology; ESH: European Society of Hypertension; NICE: National Institute for Health and Care Excellence; SOGC: Society of Obstetricians and Gynecologists of Canada; SOMANZ: Society of Obstetric Medicine of Australia and New Zealand.
While international agencies recognize preeclampsia as an important risk factor for CVD, they differ in their recommendations on the management of these patients (Table 4). There is currently no clear consensus on what postpartum screening should be performed, how often this screening should be repeated, and if thresholds and targets for treatment should be different in these patients. Future studies should address these gaps in order to inform consistent and specific guidelines. As patients are most likely to see their family physician in the postpartum period, 11 these guidelines should be targeted towards primary care providers.
One of the strengths of our study was evaluating whether recommendations given to physicians, inferred by their patients’ attendance in PPPC, improved physician knowledge and management of a high-risk patient population. Another strength was that our study assessed various important management practices, such as clinical follow-up. Further, we compared different groups of physicians, including many specialties and practice types, in an attempt to identify areas of focus for future education. This differs from other studies that tended to examine only obstetricians or family physicians.25,28,29 Lastly, few studies have evaluated the knowledge of Canadian physicians on the long-term risks of preeclampsia.
This study has several limitations, one of which being its sample size. The number of survey responses received was limited by the study being conducted over the summer, when many physicians may have been vacation, and by the use of fax to distribute the survey. It is possible that some clinics never received the faxed survey either because their fax address was not up to date, or the survey was screened by front office staff. Another limitation of this study is that there may exist a response bias. While this was attempted to be negated by emphasizing the anonymity of the study, it is possible that physicians may have over-reported performing a management strategy. There also may have been a selection bias if physicians were more likely to complete the survey if they felt they were more knowledgeable, which may overestimate both knowledge and management. A proportion of physicians who had a patient attend the PPPC were obstetric internists; hence, the higher reported frequency of counseling on CVD risk could have been attributed to the specialty itself; however, there was no significant increase in other clinical practices, suggesting the specialty of obstetric medicine was not enough to explain the difference. Further, over half of the physicians had a patient who attended an obstetric medicine clinic, where obstetric internists also generally provide counseling on CVD risks. This may underestimate the difference between physicians who had a patient attend the PPPC compared to those who did not. This study also did not survey other healthcare workers involved in pregnancy care, such as midwives, nurse practitioners, or nephrologists, whose knowledge and management would also impact the long-term health of patients with a history of preeclampsia.
Conclusion
The development of preeclampsia unveils an opportunity to intervene and reduce a patient's future risk of CVD and other vascular diseases. Importantly, physicians who had a patient attend a vascular risk reduction clinic reported higher frequencies of counseling patients with a history of preeclampsia on their CVD risk. While there are limitations to the study's generalizability, this study does show an interesting signal that postpartum vascular risk reduction clinics may have a positive impact on clinical practice. Further, a recent patient-reported study found that PPPC patients had more follow-up with their family physicians for vascular risk management. 23 This may reinforce the utility of such clinics, even if patients are discharged back to their primary care providers. Overall, physicians in our region had some knowledge of preeclampsia as a risk factor for CVD, but the reported clinical management warrants improvement. The results of this study call for increased education of physicians on the long-term risks of preeclampsia as well as clear guidelines to facilitate the effective long-term management of these patients in primary care. Specialized clinics can form a part of the strategy, but more concrete and specific national and international guidelines with knowledge translation strategies are needed to target the broader group of practitioners who care for these high risk patients long-term.
Following a pregnancy complicated by preeclampsia, patients may be followed by their obstetrician or family physician, who most often see them for a 6-week post-partum follow-up. Patients may also have been referred to obstetric (internal) medicine who often follow them until resolution of the hypertension. They may subsequently be referred to the PPPC typically seen at 3–6 months postpartum to be followed for 1 year post-partum for lifestyle counseling and ongoing risk screening and treatment. Patients are ultimately discharged back to family physicians. They may be referred to specialists, such as general internists (including hypertension and lipid specialists), cardiologists, and nephrologists on an as-needed basis (Figure 1).
Data were collected via physician survey, and self-reported responses were displayed above (Figure 2).
Reported management practices were evaluated via physician survey on the long-term cardiovascular risk associated with preeclampsia, including history taking, counseling, and follow-up. Data are reported as the percentage of physicians who report performing a practice more than half the time and compared based on whether the physician reporting having a patient attend the PPPC. Data were analyzed using binary logistic regression on SPSS. * indicates a significant P-value of <0.05 (Figure 3).
Reported management practices were evaluated via physician survey on the long-term cardiovascular risk associated with preeclampsia, including history taking, counseling, and follow-up. Data are reported as the percentage of physicians who report performing a practice more than half the time and compared based on physician specialty. Data were analyzed on SPSS (Figure 4).
Supplemental Material
sj-docx-1-obm-10.1177_1753495X241275847 - Supplemental material for Does having a patient attend a postpartum vascular risk reduction clinic improve physician knowledge and management of preeclampsia as a cardiovascular risk factor?
Supplemental material, sj-docx-1-obm-10.1177_1753495X241275847 for Does having a patient attend a postpartum vascular risk reduction clinic improve physician knowledge and management of preeclampsia as a cardiovascular risk factor? by Jaslyn Rasmuson and Winnie Sia in Obstetric Medicine
Footnotes
Contributorship
WS and JR contributed to the design, analysis, and manuscript of the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the University of Alberta Ethics board number Pro00092260.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Women and Children's Health Research Institute's Summer Research Scholarship for Undergraduate Student at the University of Alberta.
Guarantor
Winnie Sia guarantees this manuscript's accuracy and the contributorship of the co-author.
Informed consent
All participants provided implicit consent when they completed the online survey using the QR code.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.