
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) often coexists with various systemic diseases, forming a comorbid condition. The causal evidence from Mendelian randomization (MR) studies on the impact of comorbidities on COPD is accumulating, yet information for comprehensive summary is limited.
Objectives:
This study aimed to systematically summarize the evidence from MR studies on the impact of comorbidities on COPD.
Design:
Systematic review and meta-analysis of MR studies.
Data sources and methods:
Eight electronic databases were searched to identify relevant MR studies about comorbidities associated with COPD from inception to June 3, 2024. Strengthening the Reporting of Observational Studies in Epidemiology—Mendelian Randomization (STROBE-MR) guidelines were used for reporting quality assessment. We used either a random-effects model or a fixed-effects model to estimate pooled causal evidence from MR studies of comorbidities and COPD.
Results:
A total of 26 studies were included, of which 8, 4, and 3 studies summarized the causal effects of GERD, depression, obesity on the risk of COPD, respectively. Overall, the studies included had high reporting quality. Our meta-analysis using inverse variance weighted (IVW) of main MR analyses revealed positive causal effects of GERD (OR: 1.64; 95% CI: 1.47–1.84), depression (OR: 1.31, 95% CI: 1.01–1.71), and obesity (OR: 1.51; 95% CI: 1.25–1.83) on COPD. Our qualitative analysis also identified multisystem diseases such as asthma, bronchiectasis, peptic ulcers, heart failure, hypertension, rheumatoid arthritis, and osteoarthritis, as well as systemic conditions like anemia and frailty, were related to the risk of COPD.
Conclusions:
This study revealed the causal effects of comorbidities on COPD, providing new scientific evidence for the prevention and treatment of COPD, and aiding in the guidance of effective clinical strategies.
Registration:
This systematic review and meta-analysis protocol was prospectively registered with PROSPERO (No CRD42024575341).
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by chronic respiratory symptoms, including dyspnea, cough, and expectoration. 1 With its high prevalence, high disability rates, and substantial disease burden, COPD has emerged as a major concern in public health. 2 In 2019, COPD became the third leading cause of death worldwide. 3 The World Health Organization estimates that by 2030, more than 4.5 million people globally will die from COPD and its related diseases annually. 4 The China Pulmonary Health study 5 conducted in 2018 revealed that the prevalence of COPD among individuals aged 20 years and older was 8.6%, rising to 13.7% for those over 40. With an estimated 100 million affected individuals, COPD has become one of the most common chronic diseases, comparable to hypertension and diabetes.
As a chronic inflammatory disease, the impact of COPD is not confined to the lungs and often forms complex comorbidities with a variety of systemic diseases. Cardiovascular disease exacerbates the pathological process of COPD, caused by systemic inflammation and oxidative stress, significantly impacting disease progression, clinical outcomes, and mortality.6 –8 Gastroesophageal reflux disease (GERD) is a precipitating factor for the development of COPD, which may trigger airway inflammation through false aspiration of gastric contents, thereby worsening the airflow limitation and exacerbation of symptoms, and negatively affecting the overall prognosis of COPD patients.9,10 Emerging evidence suggests that low-grade chronic inflammation, in part, mediates the association between depressive symptoms and impaired pulmonary function. Increased levels of inflammatory markers have been noted in both late-life depression and COPD.11,12 In a recent study of a population sample of older adults, elevated levels of the inflammatory biomarkers interleukin-6 and C-reactive protein contributed to explaining the association between depressive symptoms and pulmonary obstruction. 13 Additionally, the high prevalence of anxiety and depression among COPD patients is closely related to the pathophysiological processes of COPD and the reduction in quality of life. 14 This undoubtedly emphasizes the importance of psychological health support. These comorbidities exacerbate the pathological course of COPD, increase the risk of mortality, and complicate treatment management. Moreover, they significantly increase the medical burden, severely affecting both their prognosis and quality of life. Therefore, identifying and managing comorbidities in COPD is crucial for improving symptoms, reducing acute exacerbations, enhancing both treatment outcomes, and quality of life.
Mendelian randomization (MR) is an epidemiological method that uses genetic variant as instrumental variables to assess causal relationships. Based on Mendelian laws of inheritance, MR assumes that genotypes are randomly assigned at birth, independent of environmental factors and lifestyle influences, to evaluate the causal association between exposures and clinical outcomes. 15 The strength of MR lies in providing an unbiased approach for causal inference, particularly when randomized controlled trials are not feasible, and observational studies yield biased associations due to confounding or reverse causality. These issues are addressed by using genetic variants as instrumental variables for testing exposures. The alleles of these exposure-related genetic variants are randomly assigned and not affected by reverse causality. 16 Using genetic variants as tools, MR studies provide a powerful means to identify and assess potential causal associations between comorbidities and COPD. They also reveal the impact of genetic susceptibility on the onset and progression of COPD, thereby establishing a solid scientific basis for the development of personalized prevention and treatment strategies.
Although the causal evidence from MR studies on the impact of comorbidities on COPD is accumulating, there is currently no systematic review and meta-analysis to comprehensively evaluate this evidence. Our study aimed to synthesize and assess the evidence from MR studies on the impact of comorbidities on COPD, in order to precisely quantify the impact of genetic variations on COPD risk. It seeks to offer scientific support for COPD prevention, diagnosis, and treatment, guiding future research and policy to improve health and quality of life for those with COPD.
Methods
Search strategy
This study adhered to the guidelines of the Meta-analysis of Observational Studies in Epidemiology (MOOSE). 17 The process is outlined in Supplemental Table 1. We conducted a systematic search on eight databases, including PubMed, Embase, the Cochrane Library, Web of Science, China National Knowledge Infrastructure (CNKI), Chongqing VIP (CQVIP), WANFANG Data, and China Biology Medicine (CBM), to identify eligible studies published up to June 3, 2024. We employed a strategic blend of Medical Subject Headings (MeSH) and free words, customizing specific search strategies for each database. The search terms were appropriately tailored to different databases to identify all eligible studies. The search strategies were associated with “chronic obstructive pulmonary disease,” and “Mendelian randomization.” The search strategies are provided in Supplemental Table 2.
Inclusion and exclusion criteria
We included studies that met the following criteria:
Any study using MR to investigate the causal relationship between comorbidities and the risk of COPD, regardless of negative or positive results.
We excluded studies that met the following criteria:
No relation to the risk of COPD, including magnetic resonance imaging and other imaging studies.
Exposure factors are not comorbidities.
Only reverse causality.
Non-English.
Duplicate publications, conference abstracts, and studies with incomplete or inaccessible data.
Study selection
All identified studies were imported into Endnote X8 software, where duplicates were initially eliminated. Two researchers independently screened potential eligible studies by examining titles and abstracts. The appropriate studies were then determined by obtaining and reviewing the full-text articles. A third researcher served as an arbitrator to resolve any discrepancies through consensus.
Quality assessment
Given the absence of an assessment tool specifically for the risk of bias in MR studies, we used the Strengthening the Reporting of Observational Studies in Epidemiology—Mendelian Randomization (STROBE-MR) guidelines to evaluate the reporting quality of included studies. 18 Two researchers evaluated the reporting quality of each study, across six sections: title and abstract, introduction, methods, results, discussion, and other information, with a total of 20 items. Each item will be defined “yes” or “no” depending on whether the author explicitly stated or not, counting as “1” or “0” point, respectively. The quality assessment score was converted into a percentage, with scores below 75%, between 75% and 85%, and above 85% indicating high, moderate, and low reporting quality, respectively. 19 We addressed any disagreement through collaborative consensus. The detailed description of checklist items is presented in Supplemental Table 3.
Data extraction
Two investigators independently extracted the necessary information using a preset data extraction form. The information includes the title, first author, publication year, ethnic origin, exposure factors, publicly available Genome-Wide Association Studies (GWAS) databases, design of the MR study, sample size, single nucleotide polymorphisms (SNPs), MR analysis method, and other relevant details. Disputes were resolved by an impartial third-party reviewer to reach consensus or through team discussions.
Statistical analysis
To assess the causality of comorbidities on COPD, we conducted a meta-analysis using the metan command in STATA 15.1. 20 When we identified at least three independent studies reporting a causal effect of exposure factors or genetic tools on COPD, this analysis was performed. In cases with two or fewer studies, a systematic review was conducted. Additionally, we performed individual meta-analyses for various MR analysis methods, including inverse variance weighted (IVW), weighted median (WM), and MR-Egger. The primary objective was defined as the impact of genetic variation on the risk of COPD, reported as an odds ratio (OR) with 95% confidence intervals (CIs).
Heterogeneity among studies was evaluated using Cochran’s Q test and I2 test statistic. I2 > 50% was considered substantial heterogeneity. In the presence of substantial heterogeneity, a random-effects model was employed; otherwise, a fixed-effects model was utilized. Sensitivity analysis was conducted by sequentially excluding one study at a time to assess the impact on the causal association and to determine the robustness of our findings. Publication bias was assessed by Begg’s test. In this study, a statistically significant result was considered to be when p < 0.05.
Results
Study search and selection
Initially, we retrieved 2732 studies from 8 databases. Nine hundred twenty-one duplicate studies were firstly excluded. After reviewing titles and abstracts, an additional 1730 studies were excluded. Upon reviewing the full-text articles, we further excluded 55 articles. Consequently, 26 studies were included for qualitative synthesis, and 13 studies for quantitative synthesis. The detailed screening process is illustrated in Figure 1.
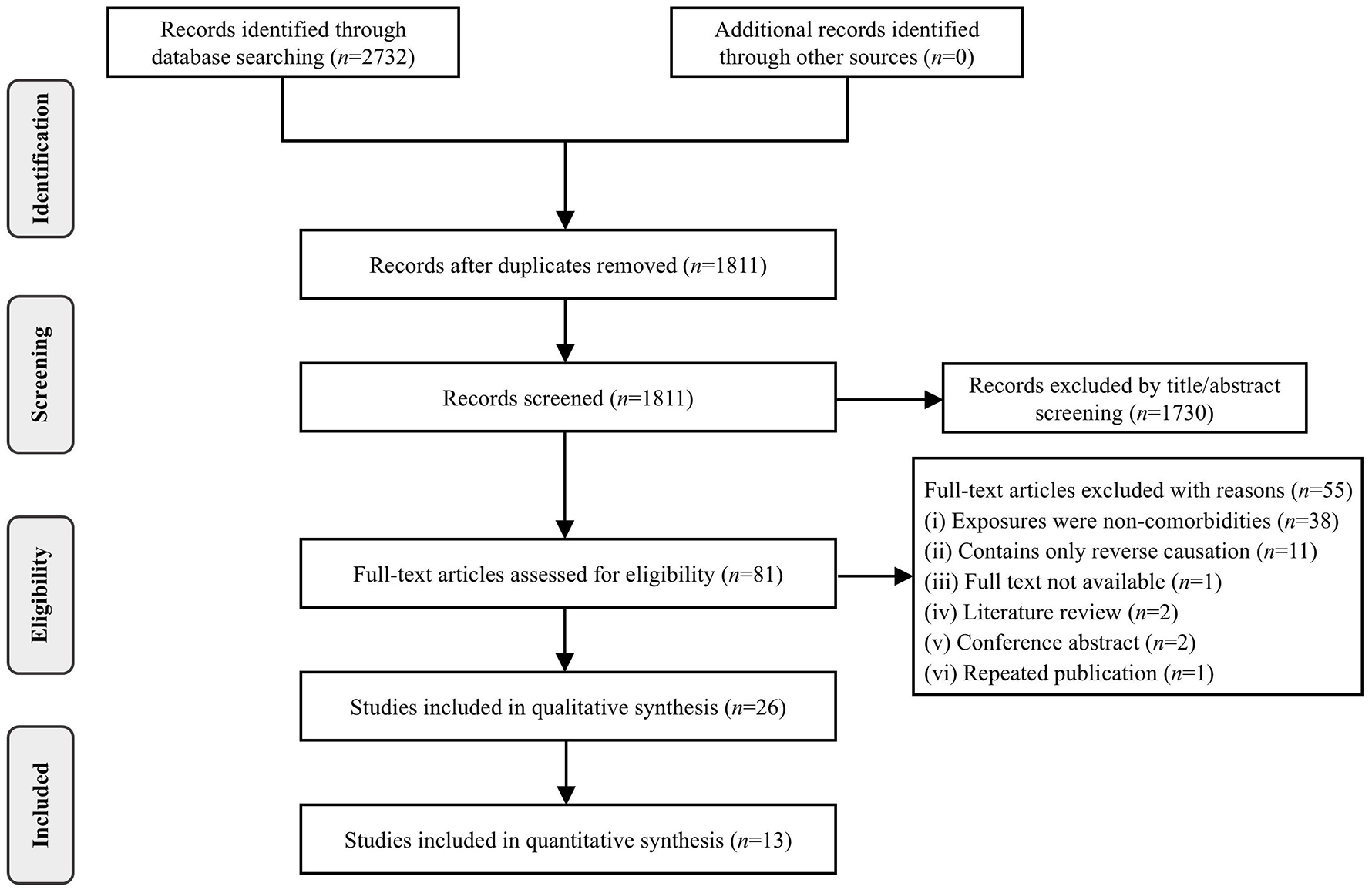
Flow diagram of study selection.
Characteristics of included studies
A total of 26 studies21 –46 were included and published in 2023 and 2024. Among these, 13 studies were eligible for quantitative synthesis. Eight studies21,24,27,28,33,34,40,43 reported the causal effect between GERD and COPD, with five showing a bidirectional effect and three showing a unidirectional effect. Four studies25,28,36,46 reported on depression, all of which were bidirectional. Three studies30,37,46 described on obesity, with two showing a bidirectional relationship and one a unidirectional relationship. In addition to the exposure factors mentioned for meta-analysis, our study covered a range of systemic diseases, including asthma, rheumatoid arthritis, peptic ulcer, heart failure, anemia, frailty, and others. The datasets for COPD in this study are derived from several sources, including 22 studies from FinnGen, 2 from the UK Biobank, and 2 from GWAS data. All 26 studies involved European populations, with one study 27 including both European and East Asian populations. The included studies assessed multiple comorbidities, with the number of SNPs varying from 4 42 to 422. 30 The sample size ranged from 186,176 to 635,172. The basic characteristics are shown in Table 1. The list of excluded studies and with reasons for exclusion can be found in Supplemental Table 4.
Characteristics of included studies.

COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease.
Quality assessment of included studies
Using the STROBE-MR guidelines to assess the reporting quality of studies, we found that the overall quality was medium to high. Specifically, 21 studies met the high-quality standards, with reporting quality percentages all exceeding 90%, while 5 studies were rated as medium quality, ranging from 80% to 85%. All included studies mentioned MR in titles and abstracts. Specifically, in the Introduction section, they described the scientific background and theoretical knowledge, including the potential relationship between exposure and outcome, clarifying the purpose of the study. In the Methods section, they detailed the research design, data sources, three core assumptions, the assessment of statistical power, sensitivity analysis, and other analyses. In the Results section, they presented the main findings, significant results, and limitations. Results of the reporting quality assessment for the included studies are detailed in Table 1.
Meta-analysis of causal evidence for comorbidities and COPD
A total of eight studies for GERD, four for depression, and three for obesity were selected for quantitative analysis due to common exposure factors among the studies.
When we assessed the causal effect of GERD on the risk of COPD using the IVW method, a positive causal effect was found (OR: 1.64; 95% CI: 1.47–1.84; I2: 68.7%; Figure 2). Subsequently, further analysis using the WM method was conducted to evaluate whether these results support the IVW results. The positive correlation was again confirmed to be significant (OR: 1.56; 95% CI: 1.36–1.78; I2: 56.8%; Figure 3). However, the analysis employing the MR-Egger method did not show a significant effect of GERD on the risk of COPD (OR: 1.13; 95% CI: 0.81–1.58; I2: 0.0%; Figure 4).

Forest plot of studies that evaluated the causal effect of GERD on COPD using values obtained by the IVW method.

Forest plot of studies that evaluated the causal effect of GERD on COPD using values obtained by the WM method.
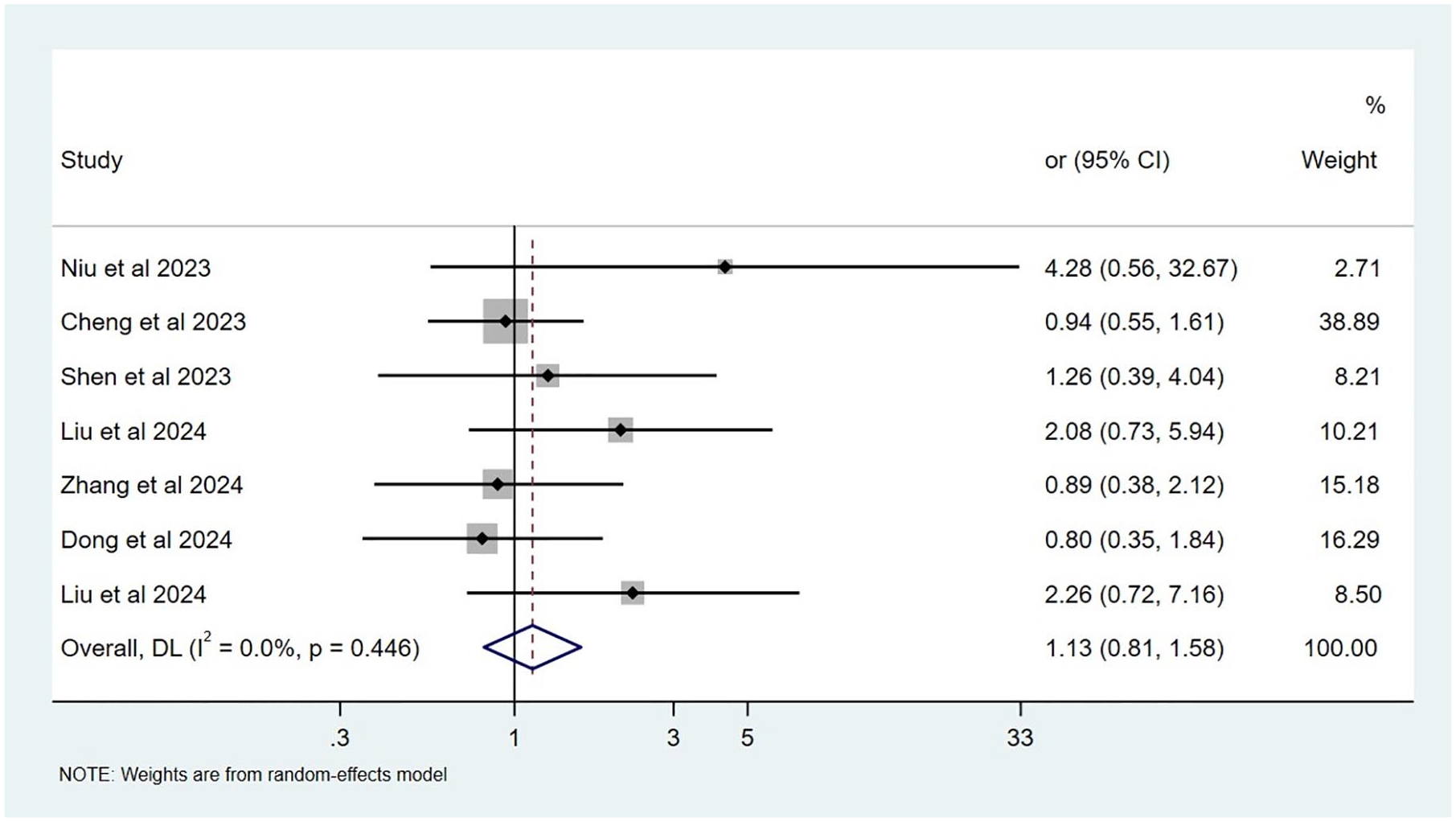
Forest plot of studies that evaluated the causal effect of GERD on COPD using values obtained by the MR-Egger method.
When examining the potential causality of depression on the risk of COPD using the IVW method, we found a positive association between the two (OR: 1.31, 95% CI: 1.01–1.71; I2: 96.6%; Figure 5). This association was corroborated by the WM method, which substantiated the results of the IVW analysis (OR: 1.31; 95% CI: 1.01–1.69; I2: 95.1; Figure 6). Nevertheless, the MR-Egger analysis failed to demonstrate that depression had a significant effect on COPD (OR: 0.96; 95% CI: 0.81–1.14; I2: 9.9%; Figure 7).

Forest plot of studies that evaluated the causal effect of depression on COPD using values obtained by the IVW method.
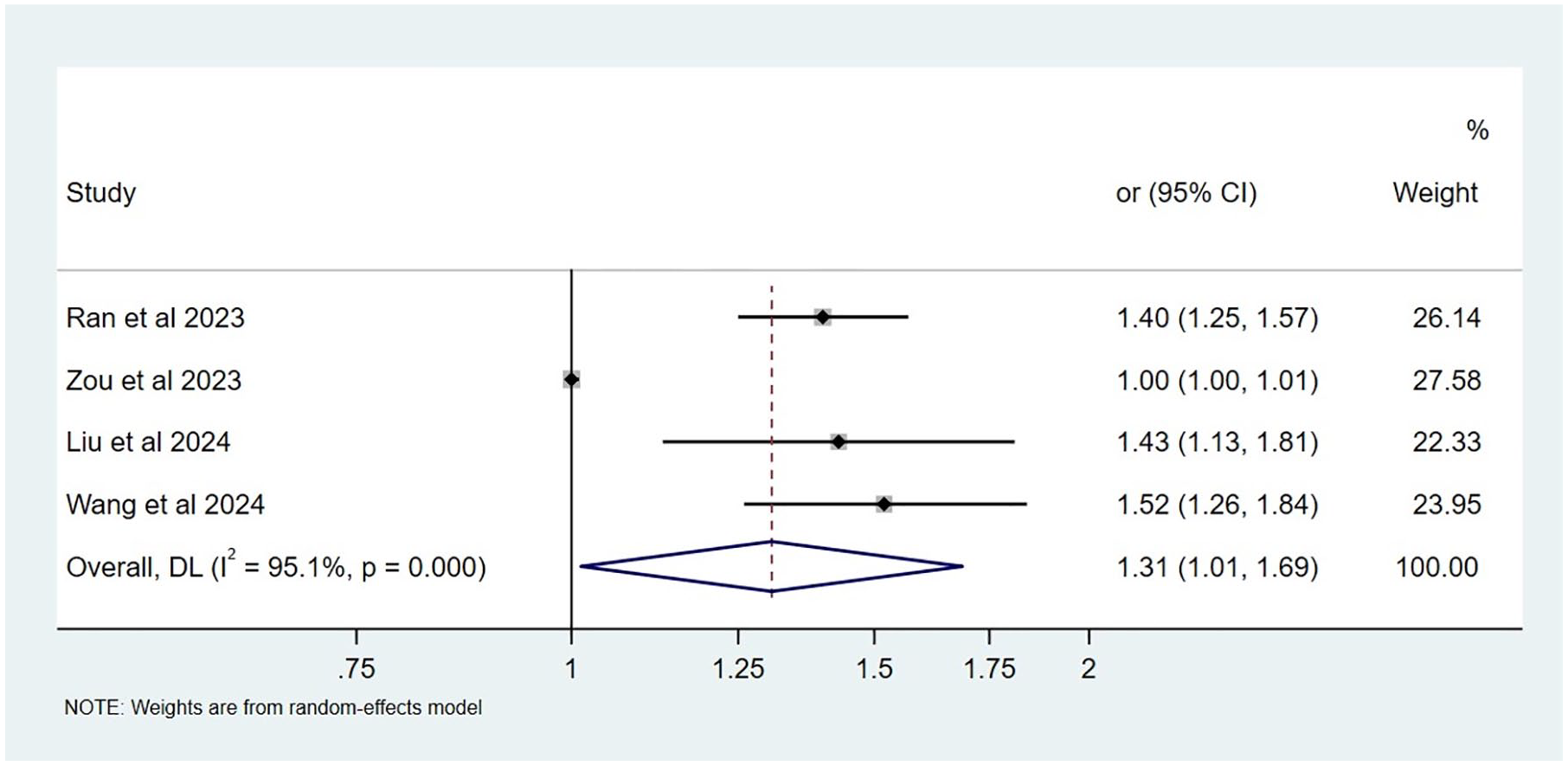
Forest plot of studies that evaluated the causal effect of depression on COPD using values obtained by the WM method.

Forest plot of studies that evaluated the causal effect of depression on COPD using values obtained by the MR-Egger method.
Using only the IVW method to evaluate the causal effect of obesity on COPD, a positive correlation was observed (OR: 1.51, 95% CI: 1.25–1.83; I2: 90.6%; Figure 8). Further analysis with the WM method confirmed the initial findings, indicating a significant positive correlation (OR: 1.45, 95% CI: 1.15–1.84; I2: 89.3%; Figure 9). In contrast, the MR-Egger analysis yielded no significant effect (OR: 1.33; 95% CI: 0.98–1.80; I2: 70.9%; Figure 10).
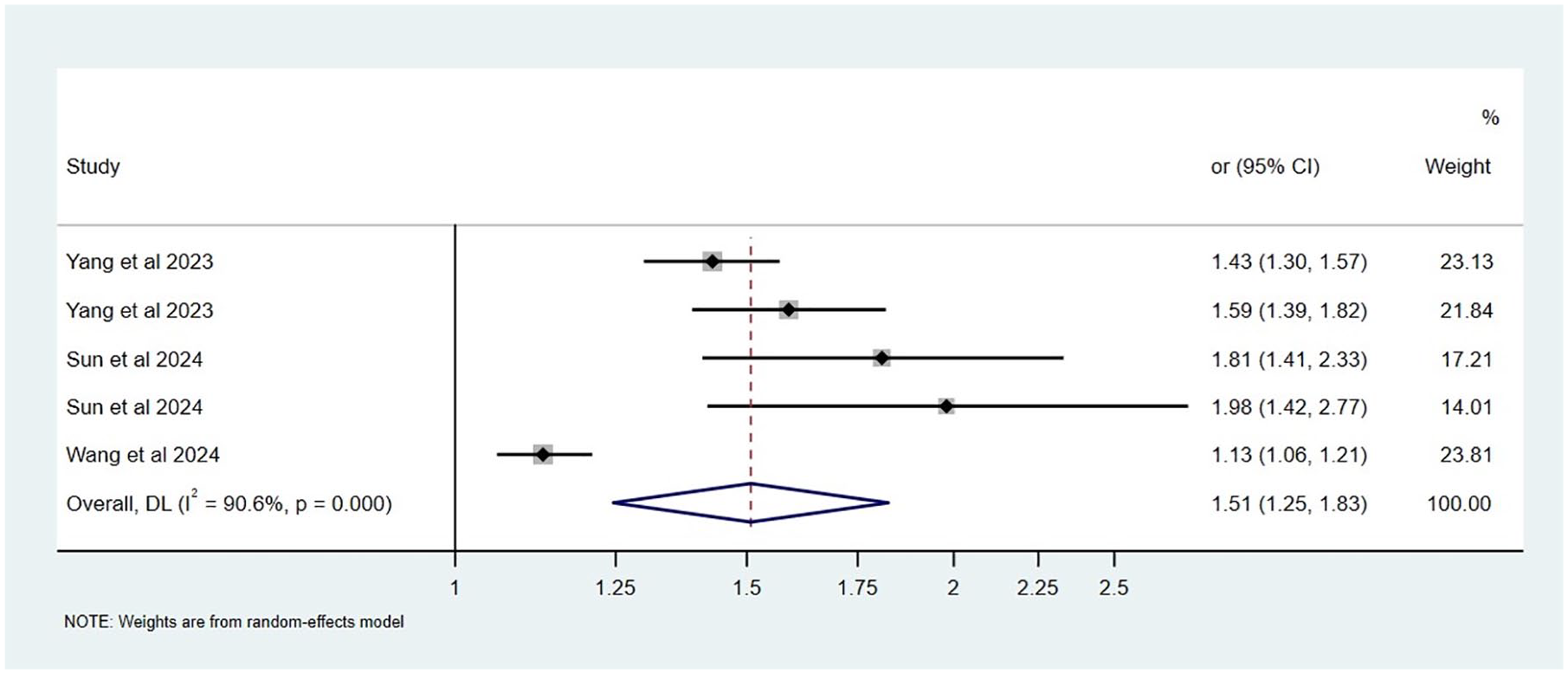
Forest plot of studies that evaluated the causal effect of obesity on COPD using values obtained by the IVW method.

Forest plot of studies that evaluated the causal effect of obesity on COPD using values obtained by the WM method.

Forest plot of studies that evaluated the causal effect of obesity on COPD using values obtained by the MR-Egger method.
Qualitative analysis of causal evidence for comorbidities and COPD
A total of 14 studies were selected for qualitative analysis.22,23,26,27,29,31,32,35,38,41,42,44 -46 Among them, comorbidities that have a positive causal effect on COPD include chronic sinusitis, asthma, sleep apnea syndrome, bronchiectasis, hypertension, heart failure, osteoarthritis, rheumatoid arthritis, peptic ulcer disease, frailty, anemia, periodontitis, and psoriasis. Conversely, a study found a negative causal relationship between ischemic heart disease and COPD. 46 Furthermore, no causal relationship was identified for conditions such as allergic rhinitis, acute sinusitis, nasal polyps, irritable bowel syndrome, Crohn’s disease, ulcerative colitis, functional dyspepsia, non-infectious gastroenteritis, constipation, systemic lupus erythematosus, and inflammatory bowel disease with regard to COPD. The detailed results are presented in Table 1.
Sensitivity analysis
The sensitivity analysis indicated no outliers for the causal effects of GERD, depression, and obesity on the risk of COPD after excluding one study at a time, confirming the stability of our results (Supplemental Figures 1–3).
Publication bias
The Begg’s test did not reveal significant publication bias in the causal effects of GERD, depression, and obesity on the risk of COPD (p = 0.902, p = 1.000, and p = 0.462) (Supplemental Figures 4–6).
Discussion
This is the first systematic review and meta-analysis of MR studies examining the causal effect of comorbidities on COPD. Our pooled results reveal that GERD, depression, and obesity have a positive causal effect on the risk of COPD. The results of our comprehensive analysis not only coincide with the prior MR studies, but the qualitative analysis also found that asthma, bronchiectasis, peptic ulcers, heart failure, rheumatoid arthritis, osteoarthritis, anemia, and others affect COPD. These findings further corroborate those reported in recent studies,47 –50 offering new scientific evidence for the prevention and treatment of COPD. Overall, the studies included in this systematic review are of high reporting quality and do not reveal significant publication bias, providing a solid foundation for our conclusions.
GERD is a common comorbidity of COPD and is associated with an increased risk of acute exacerbations, hospitalization, emergency department visits, higher costs, and impairment of quality of life. 51 A systematic review and meta-analysis revealed that GERD is clearly identified as a risk factor for COPD exacerbations (RR: 7.57; 95% CI: 3.84–14.94). The prevalence of GERD in patients with COPD is significantly higher than in those without COPD (RR: 13.06; 95% CI: 3.64–46.87). 52 Given the potential for GERD to aggravate the clinical status of COPD and for the mechanical changes associated with COPD to intensify GERD, it is crucial to understand the relationship and potential consequences of their co-occurrence. 53 Despite the bidirectional association between GERD and COPD, a causal relationship remained ambiguous. Nonetheless, our findings confirm a direct causal effect of GERD on COPD, consistent with the findings of the MR studies we included.
Although the specific mechanisms underlying the association between GERD and COPD have not yet been fully illustrated, possible mechanisms include the airway inflammation induced by the inhalation of gastric acid and digestive enzymes, 10 and neural reflexes. 54 These factors may lead to airway constriction, decreased lung function, and chronic inflammatory responses, exacerbating the symptoms and COPD prognosis. Furthermore, immune responses and systemic inflammation 55 may also contribute to the comorbidity mechanism of the two conditions. However, Zou et al. 28 did not find a causal effect of GERD on COPD. We preliminarily believe this may be related to the selection of data and population, and further research is needed to verify this. By summarizing MR studies, we have provided further evidence to support the hypothesis that GERD may increase the risk of COPD. Effective control of GERD can not only improve the quality of life but may also slow down the progression of COPD. Consequently, clinicians should consider including GERD management in the treatment plan for COPD to achieve more comprehensive disease control.
Depression is frequently reported in association with COPD. A meta-analysis and systematic review 56 revealed that patients with COPD exhibit a significantly higher incidence of depression (27.1% vs 10.0%) compared to control group. Furthermore, depression is a significant risk factor for frequent exacerbations of COPD, shortening the time between exacerbations. 57 A bidirectional association between depression and COPD has been reported in previous studies, whether this association is causal remains to be further clarified. A study utilizing the two-sample MR method to explore the bidirectional relationship found that COPD did not affect the incidence of depression (OR: 0.989, p = 0.824), whereas depression may promote the development of COPD (OR: 1.421, p = 0.001). These findings suggest that depression may be a risk factor for COPD. 36 This insight highlights the importance of strengthening prevention and screening for COPD in patients with depression.
A study utilizing NHANES data from 2013–2018 discovered a significant association between depression and COPD, further supporting the critical role of depression in the management of COPD. 25 Our meta-analysis further validates the findings, offering evidence for the causal effect of depression on COPD. However, due to inadequate recognition of depression as a comorbidity, this psychological disorder is often neglected and underdiagnosed, which results in a lack of prompt diagnosis and effective treatment. Patients with untreated COPD-related depression have a poorer quality of life, lower adherence to COPD treatment plans, along with more severe disease progression, higher hospitalization rates, and increased medical costs.58,59 MR studies use genetic variations to explore the biological connections between depression and COPD. A study 60 indicates that the activation of inflammatory pathways may be the biological basis for their interaction. Our findings help us understand how depression increases the risk of COPD and provide scientific evidence for the formulation of prevention strategies, treatment plans, and prognostic assessments.
Obesity is considered a risk factor for various chronic diseases. The impact of obesity on the development, severity, and prognosis of asthma and COPD is attracting growing attention. The effects of obesity on the respiratory system range from a decline in total lung capacity to humoral alterations. Adipose tissue significantly contributes to the establishment of an inflammatory state, serving as a vital source of adipokines. 61 A prospective cohort study on chronic diseases with a 10-year follow-up in China provides evidence of the relationship between obesity metrics and COPD risk in Chinese adults, emphasizing the potential importance of maintaining an appropriate body weight and waist circumference in the prevention of COPD. 62 MR methods have been widely applied to explore the causal relationship between obesity and various chronic diseases,63,64 due to their advantages in reducing confounding factors and reverse causality issues in conventional observational studies. Our meta-analysis further corroborates the research conclusions drawn from systematic reviews, providing a more solid evidence base that obesity is a risk factor for the development of COPD. Decreasing the prevalence of overweight and obesity is a major public health goal.
Regarding the various analysis methods of MR, using IVW and WM, our meta-analysis showed that GERD, depression, and obesity may increase the risk of COPD. However, the MR-Egger analysis did not find a significant causal effect of these comorbidities on COPD, with similar negative findings also observed in the original studies. Despite the MR-Egger analysis failing to support this causal relationship, some scholars65 –67 believe that when the main results of the MR analysis are positive, and the direction of the effect of exposures on the outcome aligns with the main results from other methods, the overall results can still be considered positive. This perspective, by considering various analytical methods, helps to better understand MR study results. Even if significance is not observed in some methods, the possibility of causal association should not be easily dismissed. Instead, conclusions drawn from different methods should be thoroughly assessed.
This study explored the multi-system comorbidities of COPD and summarized the evidence of causal associations between these comorbidities and COPD from MR studies. Studies have shown that COPD is not only affected by respiratory diseases such as chronic sinusitis, nasal polyps, asthma, bronchiectasis and sleep apnea syndrome but is widely associated with multiple system diseases. Gastrointestinal system diseases like peptic ulcers, cardiovascular system diseases such as heart failure, ischemic heart disease, hypertension, and rheumatic system diseases including rheumatoid arthritis and osteoarthritis are all related to the progression of COPD. In addition, systemic conditions like anemia and frailty also play a key role in the course of COPD. These findings emphasize the importance of considering the impact of multisystem diseases on the overall health of patients in the prevention, screening, and treatment strategies for COPD. By implementing targeted interventions, we expect to reduce the risk of disease progression and enhance their quality of life. Freund et al. 68 have found that higher smoking pack-years was an independent risk factor for coronary microvascular disease. This finding indirectly suggests that smoking may be a potential confounder not fully assessed in most MR studies. Smoking may act as a key confounding variable affecting the causal inference between comorbidities and COPD. Therefore, after controlling for the confounding effect of smoking, it is worth further exploring and verifying whether there is a real causal association between them.
COPD is a complex disease that often coexists with various comorbidities. Research confirms that COPD patients exhibit a chronic low-grade systemic inflammatory state even during stable periods. 69 This inflammation is suggested to be a key pathophysiological link between COPD and multiple comorbidities. Specific inflammatory markers, such as the monocyte to lymphocyte ratio (MLR), red cell distribution width (RDW), and interleukin-6 (IL-6) are closely associated with pulmonary heart disease and depression in patients with COPD. 70 A large population-based study demonstrated that elevated levels of C-reactive protein (CRP), fibrinogen, and white blood cell count are associated with an increased risk of diabetes, cardiovascular diseases, and lung cancer in patients with COPD. 71 As a key trigger, smoking exacerbates this process through multiple pathways. Huang et al. 72 used MR to confirm that former smoking increases both the prevalence and hospitalization risk of COPD. The genetic susceptibility to smoking is significantly associated with multiple systemic diseases. A study summarized evidence from MR studies to assess the causal role of smoking in various diseases, revealing that smoking is linked to increased risks of circulatory diseases, digestive disorders, epilepsy, musculoskeletal conditions, endocrine, metabolic diseases, ocular disorders, and cancers. One possible mechanism through which smoking increases the risk of these diseases is systemic inflammation. The reactive oxygen species in cigarettes activate the signaling cascades in epithelial cells, leading to the activation of inflammatory genes. 73 Clearly, chronic inflammation may serve as a common pathological basis that simultaneously promotes the progression of both COPD and multiple comorbidities.
Limitations
Although our systematic review and meta-analysis have provided valuable insights, there are several limitations to consider. Firstly, MR studies depend on the strength of the association between genetic variants and exposure factors, a weak association may result in inaccurate results. Secondly, the GWAS data from the studies primarily involving European populations may limit the generalizability of the results to other ethnic groups. Additionally, the MR studies included were all non-prospective and non-randomized in design and often originated from two separate databases for COPD and comorbidities. It is difficult to assert that these studies do not have a high risk of bias. Moreover, many studies lack clinical data support and rely solely on International Classification of Diseases (ICD) coding, without strictly verifying unreported confounding factors in the databases. Therefore, it is essential to fully account for these limitations when interpreting the results to ensure the accuracy and scientific validity of the research conclusions. While the MR studies have reduced the effects of reverse causality and confounding factors, the complexity of causal inference implies that results should be interpreted with caution.
Conclusion
COPD represents a major global public health problem. In order to address this challenge, it is crucial to employ reliable research methods to determine the causal effect between risk factors and COPD, providing more valuable insights than the correlational information obtained from traditional observational studies.
Our study is the first to provide a pooled estimate of the causal impact of comorbidities on the risk of COPD. Despite differences in the design and outcomes of independent MR studies on the causal relationship between comorbidities and COPD, our analysis provides causal evidence for GERD, depression, and obesity affecting COPD. We have also identified that a variety of multisystem diseases, including chronic sinusitis, asthma, bronchiectasis, peptic ulcers, heart failure, rheumatoid arthritis, anemia, frailty, and others, exert an influence on the risk of COPD. In addition, this study demonstrates high reporting quality, demonstrating the robustness of the pooled estimate and providing a basis for the reliability of the conclusion. Although the complexity of MR research may make it difficult to fully elucidate the relevant biological mechanisms, this does not weaken its importance in disease causal association studies. Through these high-quality studies, we can more accurately understand the potential impact of comorbidities on COPD, emphasizing the importance of considering multisystem diseases in the integrated management of COPD. Our findings provide a scientific basis for the prevention and treatment of COPD, contributing to the development of effective public health strategies and clinical interventions.
Supplemental Material
sj-docx-1-tar-10.1177_17534666251348393 – Supplemental material for Association between comorbidity and chronic obstructive pulmonary disease: a systematic review and meta-analysis of Mendelian randomization studies
Supplemental material, sj-docx-1-tar-10.1177_17534666251348393 for Association between comorbidity and chronic obstructive pulmonary disease: a systematic review and meta-analysis of Mendelian randomization studies by Huanrong Ruan, Siyuan Lei, Hulei Zhao, Hailong Zhang, Xuezhong Zhou and Jiansheng Li in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.