
Abstract
Background:
The readmission rate following hospitalization for chronic obstructive pulmonary disease (COPD) is surprisingly high, and frequent readmissions represent a higher risk of mortality and a heavy economic burden. However, information on all-cause readmissions in patients with COPD is limited.
Objective:
This study aimed to systematically summarize all-cause COPD readmission rates within 30 and 90 days after discharge and their underlying risk factors.
Methods:
Eight electronic databases were searched to identify relevant observational studies about COPD readmission from inception to 1 August 2022. Newcastle-Ottawa Scale was used for methodological quality assessment. We adopt a random effects model or a fixed effects model to estimate pooled all-cause COPD readmission rates and potential risk factors.
Results:
A total of 28 studies were included, of which 27 and 8 studies summarized 30- and 90-day all-cause readmissions, respectively. The pooled all-cause COPD readmission rates within 30 and 90 days were 18% and 31%, respectively. The World Health Organization region was initially considered to be the source of heterogeneity. We identified alcohol use, discharge destination, two or more hospitalizations in the previous year, and comorbidities such as heart failure, diabetes, chronic kidney disease, anemia, cancer, or tumor as potential risk factors for all-cause readmission, whereas female and obesity were protective factors.
Conclusions:
Patients with COPD had a high all-cause readmission rate, and we also identified some potential risk factors. Therefore, it is urgent to strengthen early follow-up and targeted interventions, and adjust or avoid risk factors after discharge, so as to reduce the major health economic burden caused by frequent readmissions.
Trial registration:
This systematic review and meta-analysis protocol was prospectively registered with PROSPERO (no. CRD42022369894).
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) represents a major public health problem and an increasingly significant cause of morbidity, disability, and death worldwide. The number of COPD deaths increased by 23% globally from 1990 to 2017. 1 It is also estimated that by 2060, more than 5.4 million people will die from COPD and related diseases annually. 2 COPD affects the physical and mental health and quality of life of patients and imposes a significant economic burden on society and families. A systematic review indicated that in the United States, annual per patient direct medical cost was $10,367, whereas in Asia, ranging from $1544 to $3077, and in Europe, ranging from $1889 to 11,787. 3 All-cause medical expenses increased more than twofold from $21,771 for patients with zero exacerbation to $47,061 for patients with ⩾3 exacerbations. 4
Previous studies indicated that patients with COPD have a high all-cause readmission rate,5–7 and COPD has become one of the diseases with a high readmission rate equivalent to pneumonia and heart failure. 8 There exist multiple reasons for readmission, and respiratory-related illnesses accounted for almost half of 30-day readmission. 9 A cohort study from the United States reported a 30-day readmission rate of 17.25%, with 7.69% for COPD and 9.56% for other diagnoses. Septicemia, heart failure, and respiratory tract infection were the most common non-COPD readmission diagnosis. 10 In a multicenter study from Malaysia, the 90-day COPD readmission rate was 40.74%. 11 Gender, history of frequent admissions, comorbidities, and length of stay (LOS) were relevant risk factors for 30- and 90-day readmissions.11,12 Readmitted patients mostly participate in Medicare and Medicaid and suffer from more comorbidities. 13 Obviously, 30- and 90-day COPD readmissions are common, and patients with non-COPD readmission have a greater burden of comorbidities in readmission diagnosis than those in COPD. So, early identification of readmission risk populations and regulation comorbidities other than COPD is crucial.
COPD readmission is regarded as a sign of medical quality. 14 COPD is the third leading cause of readmission in the United States, with approximately one-fifth of patients hospitalized for COPD exacerbations being readmitted within 30 days. 15 COPD was included in the Hospital Readmission Reduction Program (HRRP) in October 2014, a federal policy designed to control 30-day hospital readmission for certain common, high-impact conditions by imposing financial penalties on hospitals with higher than expected 30-day readmission after hospitalization for COPD exacerbations.16,17 Previous studies reported that the initial phase of HRRP implementation was associated with a decrease in 30-day all-cause readmission.18–21 Readmission triggers off high healthcare costs and serious adverse consequences. So, prevention of COPD readmission has been recognized as a high-priority strategy for health system globally. Although the review by Alqahtani et al. 22 reported some risk factors for all-cause COPD readmission, readmission rate has not been pooled. Therefore, this study aimed to summarize and evaluate the 30- and 90-day all-cause readmission rates and identify potential risk factors, with a view to screening patients at high readmission risk, avoiding risk factors, and strengthening postdischarge management, as well as contributing to clinical practice and public health policy.
Methods
Search strategy
This study followed the Meta-analysis of Observational Studies in Epidemiology. 23 The steps are detailed in Supplemental Table 1. We systematically searched eight databases, including PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure, Chongqing VIP, WANFANG Data, and China Biology Medicine, to identify relevant studies published from database to August 1, 2022. We used a combination of Medical Subject Headings and free words and developed detailed search strategies for each database. The search terms were adjusted appropriately according to diverse databases to determine all eligible studies. The search strategies were related to ‘chronic obstructive pulmonary disease’, ‘readmission’, and ‘risk factors’. The search strategies are provided in Supplemental Table 2.
Inclusion and exclusion criteria
We included studies that met the following criteria:
Population: Participants were diagnosed with COPD based on any accepted clinical guidelines or criteria, and hospitalized due to acute exacerbation.
Outcomes: (I) All-cause readmission rate within 30 and 90 days: It was clearly defined as readmission for any reason after hospital discharge of COPD. (II) Risk factors: Risk factors for all-cause readmission obtained using multivariable regression models.
We excluded studies that met the following criteria:
The interventions or programs go beyond conventional care.
Studies that were published in any language other than English.
Duplicate publications, conference abstract and studies with incomplete or inaccessible data.
Study selection
All retrieved studies were imported into Endnote software (version X8.1), and duplicate studies were first discarded. Two researchers independently screened for potential eligible studies by checking titles and abstracts. Suitable studies were then identified by obtaining and reviewing the full-text articles. A third researcher acted as an arbitrator to resolve any disagreements through consensus.
Quality assessment
The methodological quality assessment of the included studies were assessed independently by two reviewers using the Newcastle-Ottawa Scale (NOS). 24 Each investigator determined the methodological quality of each study, focusing on three aspects: population selection (four items), comparability (one item), and exposure or outcome assessment (three items), with a total of nine stars for eight items. For each item, a series of answers will be provided, and if a study meets the evaluation criteria, a star will be awarded. Scores of 7–9 were defined as ‘good’, 4–6 as ‘fair’, and 1–3 as ‘poor’. Any inconsistencies in this stage were resolved by consensus.
Data extraction
Two investigators extracted independently necessary information using a preset data extraction form. Information included title, first author, publication year, country, age, sample size, study design, readmission rate, risk factors, and information of assessment of risk of bias. Arguments that occurred were arbitrated through a third reviewer to reach a consensus or resolved by team discussion.
Statistical analysis
To measure the overall all-cause readmission rate, we performed a single-ratio meta-analysis using the metaprop procedure in STATA (version 15.1). 25 Heterogeneity between studies was assessed by Cochran’s Q test and I2 test statistic. I2 > 50% was defined as substantial heterogeneity. If the included studies had substantial heterogeneity, we used a random effects model; otherwise, we used a fixed effects model.
To identify possible sources of heterogeneity in all-cause readmission rate, we performed subgroup analysis by age group, World Health Organization (WHO) region, LOS, and associated comorbidities. Furthermore, we performed a meta-regression with a univariate model to assess differences between subgroups. Sensitivity analysis was performed by iteratively excluding one study at a time to evaluate the impact on the overall all-cause readmission rate and judge the robustness of our results. Publication bias was assessed by Begg’s test.
If a factor was reported in two or more studies and was derived using a multivariate model, we performed a meta-analysis. Risk factors were estimated using odds ratio (OR) and 95% confidence interval (CI), and I2 > 50% was defined as substantial heterogeneity. If there was significant heterogeneity in the included studies, we used a random effects model; Otherwise, we used a fixed effects model. In this study, the difference was judged to be statistically significant when p < 0.05.
Results
Study search and selection
We initially retrieved 4433 studies from eight databases. A total of 1461 duplicate studies were first excluded. After scanning titles and abstracts, 2845 studies were excluded. After obtaining and reviewing the full-text articles, 99 articles were excluded. Therefore, 28 studies were finally included for further analysis. The detailed screening steps are showed in Figure 1.

Flow diagram of study selection.
Characteristics of included studies
A total of 28 studies5,6,7,9,13,26–48 were included, with publication years from 2011 to 2021. There were 5 prospective and 23 retrospective studies, respectively. Based on the WHO regions, 18, 5, and 5 studies were conducted in the Americas region, European region, and Western Pacific region, respectively. The sample size ranged from 82 to 1,055,830 individuals, with the average age between 65.77 and 76.81 years old. After discharge from the COPD hospitalization, respiratory diseases were the primary discharge diagnosis of readmission occurring within 30 and 90 days. In particular, most readmissions were due to acute exacerbation of COPD (AECOPD), followed by pneumonia, respiratory failure, and heart failure. The basic characteristics are presented in Table 1.
Characteristics of included studies.
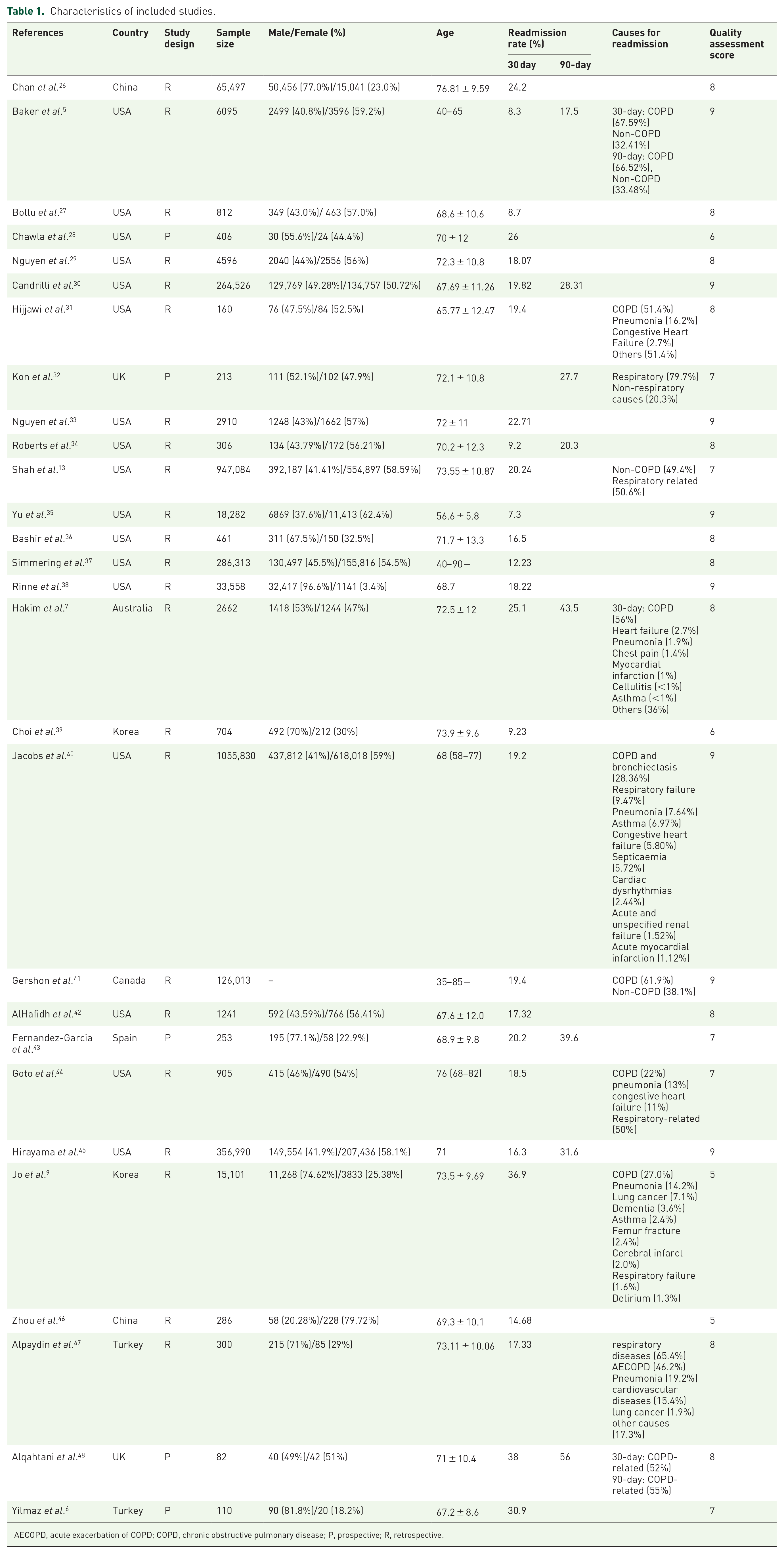
AECOPD, acute exacerbation of COPD; COPD, chronic obstructive pulmonary disease; P, prospective; R, retrospective.
Quality assessment of included studies
We assessed the methodological quality using the NOS, with scores ranging from 5 to 9. The overall quality was good, and only four articles were judged as fair, two of which were both awarded six points and five points, respectively. Considering that the comparability is not completely clear, some studies did not clearly describe the relevant variables that they controlled. The methodological assessment results of included studies are illustrated in Table 1.
All-cause readmission rate for COPD
Of the 28 studies, 27 studies summarized the all-cause COPD readmission rate within 30 days after discharge, ranging from 7.3% to 38.0%, and the pooled all-cause readmission rate was 18% (95% CI: 0.16–0.19; I2 = 99.86%) (Figure 2). Eight studies reported 90-day all-cause readmission rate ranging from 17.5% to 56.0%, and the pooled all-cause readmission rate was 31% (95% CI: 0.28–0.34; I2 = 99.55%) (Figure 3).

Forest plot of all-cause COPD readmission rate within 30 days.

Forest plot of all-cause COPD readmission rate within 90 days.
Sensitivity analysis
Sensitivity analysis indicated no outliers for all-cause COPD readmission rates within 30 and 90 days after exclusion of one study at a time, confirming the stability of our results (Supplemental Figures 1 and 2).
Subgroup analysis
Subgroup analysis regarding the age stage, the 30- and 90-day all-cause readmission rates in COPD patients with aged <70 years old were 15% (95% CI: 0.13–0.18) and 28% (95% CI: 0.19–0.37), respectively. The readmission rates in those aged ⩾70 years old were 20% (95% CI: 0.18–0.22) and 35% (95% CI: 0.27–0.43), respectively (Table 2). The regional all-cause COPD readmission rates within 30 and 90 days were 25% (95% CI: 0.17–0.34) and 40% (95% CI: 0.27–0.55) in the European region, 21% (95% CI: 0.16–0.28) and 44% (95% CI: 0.42–0.45) in the Western Pacific region, and 16% (95% CI: 0.14–0.17) and 25% (95% CI: 0.21–0.28) in the Americas region, respectively (Table 2). In terms of LOS, the 30- and 90-day all-cause readmission rates with LOS <7 days were 17% (95% CI: 0.14–0.19) and 28% (95% CI: 0.28–0.29), respectively, and those LOS ⩾7 days were 26% (95% CI: 0.12–0.42) and 44% (95% CI: 0.38–0.49), respectively (Table 2). The subgroup analysis of heart failure and diabetes indicated that all-cause COPD readmission rates were 18% (95% CI: 0.16–0.21) and 19% (95% CI: 0.16–0.21) within 30 days, and 29% (95% CI: 0.19–0.41) and 27% (95% CI: 0.17–0.37) within 90 days. The subgroup results without comorbidities were 18% (95% CI: 0.16–0.19) and 17% (95% CI: 0.15–0.19), and 35% (95% CI: 0.25–0.45) and 38% (95% CI: 0.27–0.49), respectively (Table 2).
Subgroup analysis of all-cause COPD readmission rate within 30 and 90 days and subgroup differences.
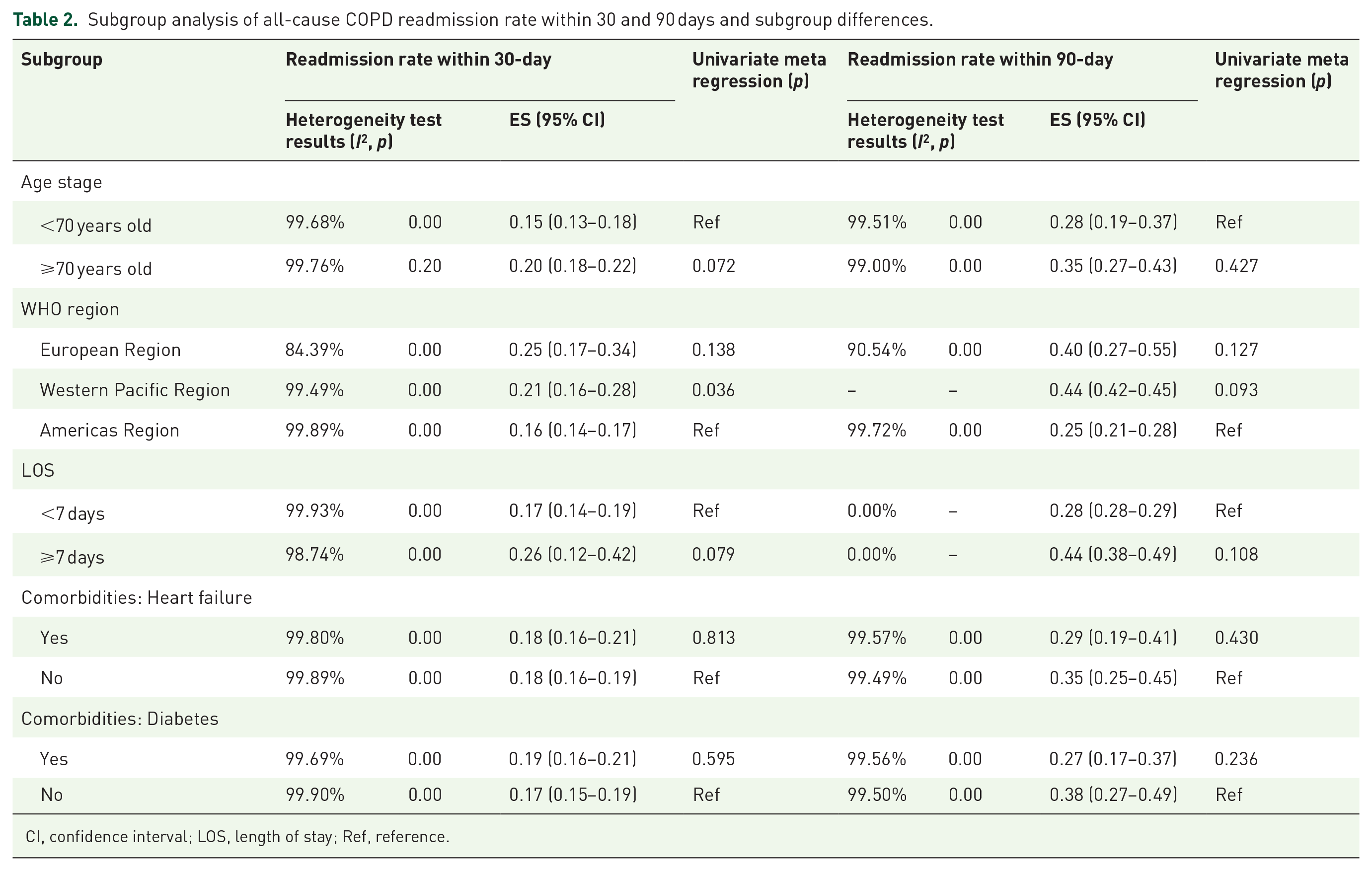
CI, confidence interval; LOS, length of stay; Ref, reference.
Subgroup differences and meta-regression
For all-cause readmission rate within 30 days after discharge in patients with COPD, subgroup difference was found in the WHO region (p = 0.036) (Table 2). Therefore, we initially considered the WHO region as the source of heterogeneity in this study. However, no subgroup difference in 90-day all-cause readmission rate was found, confirming the robustness of our results.
Publication bias
The Begg’s test did not reveal significant publication bias in all-cause COPD readmission rates within 30 and 90 days (p = 0.967 and p = 0.711) (Supplemental Figures 3 and 4).
Risk factors for all-cause COPD readmission
The meta-analysis indicated that alcohol use (OR: 1.12; 95% CI: 1.04–1.20; p = 0.002), two or more hospitalizations in the previous year (OR: 2.40; 95% CI: 1.79–3.22; p = 0.000), discharge destination (skilled nursing facility versus home) (OR: 1.37; 95% CI: 1.23–1.52; p = 0.000), discharge destination (home healthcare versus home) (OR: 1.33; 95% CI: 1.29–1.36; p = 0.000), heart failure (OR: 1.27; 95% CI: 1.23–1.32; p = 0.000), diabetes (OR: 1.11; 95% CI: 1.04–1.19; p = 0.001), chronic kidney disease (OR: 1.22; 95% CI: 1.13–1.31; p = 0.000), anemia (OR: 1.41; 95% CI: 1.10–1.80; p = 0.006), and cancer or tumor (OR: 1.80; 95% CI: 1.38–2.35; p = 0.000) were the major risk factors for 30-day all-cause COPD readmission, whereas female (OR: 0.93; 95% CI: 0.88–0.99; p = 0.020) and obesity (OR: 0.88; 95% CI: 0.85–0.91; p = 0.000) were protective factors. Two or more hospitalizations in the previous year (OR: 4.69; 95% CI: 2.62–8.41; p = 0.000) was associated with an increased risk of 90-day all-cause readmission. However, the pooled analysis results of comorbidities such as depression and chronic kidney disease were not statistically significant (p > 0.05) (Table 3).
Meta-analysis of risk factors for all-cause COPD readmission within 30 and 90 days.

CI, confidence interval; OR, odds ratio.
Discussion
This study is the first to conduct a systematic review and meta-analysis of 30- and 90-day all-cause readmission rates and associated risk factors after discharge due to an admission for AECOPD. Our study demonstated that the quality assessment of risk of bias in 28 studies was overall good. The pooled all-cause COPD readmission rates within 30 and 90 days were 18% and 31%, respectively. We also found that alcohol use, discharge destination, heart failure, diabetes, chronic kidney disease, anemia, and cancer or tumor were the major risk factors for 30-day all-cause readmission, and two or more hospitalizations in the previous year was a common risk factor for both 30 and 90 days after discharge. However, female and obesity were protective factors for all-cause readmission. Our study is different from the existing review that considered only readmission due to COPD, 49 which differed from a patient-centered approach to holistic healthcare and clinical outcomes. In recent years, a review with similar screening criteria only described the 30- and 90-day prevalence of all-cause readmission ranging from 2.6% to 82.2% and 17.9% to 63.0%. 22 On this basis, we performed a quantitative synthesis of the 30- and 90-day readmission rates, which will have a positive guiding role and significance for clinical epidemiology. The predictors that we identified were basically consistent with the results of all-cause readmission reviewed by Alqahtani et al. 22 However, considering the difference in inclusion and exclusion criteria and the sources of retrieved database compared to previous review, as well as our principle of pooling risk factors in two or more studies, this will lead to a slight difference in the summary results.
The subgroup results based on age group indicated that all-cause COPD readmission rate aged ⩾70 years old was higher than that of aged <70 years old, but no significant difference was found (p > 0.05). Although elderly patients were related to all-cause COPD readmission in previous reports,50,51 probably due to their more serious diseases and comorbidities. 52 Nevertheless, no significant differences in age group were found in our study. For one thing, this study is only a preliminary report. Then, the age provided by some studies is median, mean, or age range, and the age of included subjects in the literature was heterogeneous, which may affect the results to some extent.
The 30-day all-cause readmission rate in patients with COPD revealed a subgroup difference among the WHO regions (p < 0.05). Therefore, the WHO regions may be the source of heterogeneity. Although no statistical difference was found at 90 days, readmission rates varied by WHO regions, with higher readmission rates in the Europe region and Western Pacific region than that in the Americas region, which corresponded to 30-day readmission trend. Potential geographical differences may exist in the 30- and 90-day readmission rates in different countries: 16.3% and 31.6% in the United States, 45 25.1% and 43.5% in Australian, 7 and 20.2% and 39.6% in Spain. 43 . This also coincides with our findings. Compared with the Americas region led by the United States, the European region and Western Pacific region have higher trend of all-cause readmission at each time point. Different WHO regions and countries may have different definition criteria for readmission, which may also be used to explain the differences in readmission rate. Another consideration is the inclusion of COPD in the HRRP in 2014, which would account for the relatively low readmission rate.
The average LOS for patients with COPD is 7–10 days.53,54 Therefore, combined with the average LOS reported in the included studies, we conducted subgroup analysis with a 7-day period, and no difference was found between groups (p > 0.05). This was consistent with a meta-analysis from Wang et al., 55 which did not find a significant association between LOS and COPD readmission. Though nine and three of included studies reported a correlation between LOS and all-cause readmission, meta-analysis were not available to determine the relationship. So, further studies are needed to be explored and summarized. Comorbidities are highly prevalent among patients with COPD, seriously affecting the quality of life, and increasing the frequency of exacerbation and mortality.56,57 We conducted subgroup analyses based on common comorbidities including heart failure and diabetes, but no difference was found at each time point. A key point to consider was that when we selected the subgroups, if a study did not report this comorbidity, it was classified into a group without comorbidity, which may bring about some bias. In other terms, it also proved the stability of our pooled results.
Our meta-analysis found that alcohol use and heart failure were significant risk factors for all-cause COPD readmission within 30 days, while female was a protective factor. These results were basically accordance with the risk factors reviewed by Alqahtani et al. 22 Besides, this study have a few new findings, identifying that comorbidities such as diabetes, chronic kidney disease, anemia, and cancer or tumor as the major risk factors for all-cause readmission. The association of comorbidities with all-cause readmission is actually not surprising, given the high prevalence of comorbidities in patients with COPD. Gershon et al. 41 indicated that COPD patients along with congestive heart failure, diabetes, renal disease, and cancer tend to have higher readmission rates. Though there was some controversy about whether comorbidities were associated with frequent readmissions, our study confirmed that they were vital risk factors for all-cause readmission. This also reflects the lack of specific interventions beyond COPD during exacerbation of hospitalization. Therefore, we should actively intervene in comorbidities and focus on addressing critical risk factors for multiple diseases. This will alleviate the economic burden induced by frequent readmissions in a short time after discharge.
Consistent with previous reports,22,49 our study also identified hospitalization in the previous year as a common risk factor within 30- and 90-day readmissions after discharge. We consider that patients with frequent exacerbations may have more comorbidities and severe disease severity. Similarly, previous literature has emphasized the importance of this risk factor. 58 In addition, discharge destination was found to be a important risk factor for 30-day all-cause readmission. We tentatively considered this to be associated with disease severity and comorbidities. Among them, Bashir et al. 36 and Jacobs et al. 40 demonstrated that COPD patients who received skilled nursing facility or home healthcare were more likely to be readmitted within 30 days, compared with those who were discharged home. We consider these patients receiving nursing facility tend to have more comorbidities and complicated disease conditions, and thus, the major cause for readmission was not COPD but other related illnesses.
Alqahtani et al. 22 also illustrated that female was a protective factor and may reduce the risk of readmission, which was consistent with our findings. Compared with female, male increased the risk of COPD readmission, 59 mainly associated with higher smoking rates and lower adherence to medical services. Obesity was also a protective factor identified in our study. Compared with COPD patients with normal weight, obese patients had a 13% lower risk of 30-day readmission, and if malnutrition existed, the risk increased by 29%. 60 Depression was a common comorbidity in patients with COPD and was also documented as a vital risk factor for readmission61,62; however, this was not the case in our study. Among the included studies, only two original studies35,37 determined depression as a risk factor, with one study 37 had a p value of 0.04 and a lower limit of CI close to 1.00. So, the CI of the pooled result was wide, and no statistical difference was found. Given the high 30- and 90-day all-cause COPD readmission rates after discharge, early identification of risk factors for readmission may assist clinicians in screening patients at high risk for readmission and implement early and aggressive interventions.
Limitations
There are some limitations that need to be further elaborated. We only included articles published in English and those in other languages may be omitted, which may affected our results’ reliability. Based on current literature inclusion and exclusion criteria, we excluded studies that separately reported readmission rates and predictors for readmission. Future studies may consider conducting separate meta-analysis of the readmission rate and predictors of readmission in patients with COPD. The included studies were highly heterogeneous. In terms of subgroup analysis, we identifed WHO regions as the source of heterogeneity. However, we only explored partial significant factors obtained in the current literature and did not conduct subgroup analyses on disease severity and lung function grading, which may also be the source of heterogeneity. Despite the inclusion of heterogeneous studies, the results of sensitivity analysis were stable. No publication bias was found. So, our results were relatively reliable.
Conclusion
The all-cause COPD readmission rates within 30 and 90 days after discharge following a hospitalization for acute exacerbation were high. We identified alcohol use, discharge destination, hospitalizations in the previous year, and comorbidities such as heart failure and diabetes as common risk factors for all-cause COPD readmission, whereas female and obesity were protective factors. Our study highlighted the importance of comorbidities as a major determinant of short-term readmission in COPD. Thus, clinicians should not only focus their attention on the management of COPD itself but also on the investigation and management of COPD comorbidities. However, to truly deliver value-based care to patients will face challenges. Moreover, future research should concentrate on the development of readmission prediction models with strong applicability and effectiveness to identify, adjust, control, or avoid modifiable risk factors as soon as possible, so as to prevent and reduce the significant negative impact caused by COPD readmissions.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231202742 – Supplemental material for All-cause readmission rate and risk factors of 30- and 90-day after discharge in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tar-10.1177_17534666231202742 for All-cause readmission rate and risk factors of 30- and 90-day after discharge in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Huanrong Ruan, Hulei Zhao, Jiajia Wang, Hailong Zhang and Jiansheng Li in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.