
Abstract
Background:
Muscular atrophy often can be seen at the end of stage in many chronic diseases. It will also negatively influence patients’ outcomes. Different studies showed that the association between muscular atrophy and mortality in patients with chronic obstructive pulmonary disease (COPD) was unclear. This study will continue to assess the influence of muscular atrophy on mortality in patients with COPD.
Objectives:
To systematically evaluate the association between muscular atrophy and death in patients with COPD.
Design:
Systematic review.
Methods and data sources:
A systematic review and meta-analysis was conducted. Databases including PubMed, Web of Science, Embase, the Cochrane Library, the China Biomedical Literature Service System, China Biomedical Literature Service System (CINAHL), China National Knowledge Infrastructure, the Wanfang database, and the WeiPu (VIP) were systematically searched for cohort studies on muscular atrophy and COPD from inception to July 1st, 2023. Two reviewers independently review, assess, and extract data from the included studies. Meta-analysis was performed using RevMan 5.4 software.
Results:
Thirteen cohort studies were ultimately included, involving 10,528 patients with COPD. There were seven cohort studies included in the meta-analysis, including 3,458 COPD patients. The meta-analysis showed that patients with COPD combined with muscular atrophy had a higher mortality risk (HR = 2.20, 95%CI (1.74, 2.79), p < 0.00001). At the same time, patients with COPD who had muscular atrophy may had longer hospital stays.
Conclusion:
Muscular atrophy is associated with the mortality and disease prognosis of patients with COPD. The conclusion needs to be supported and validated by more high-quality studies given the limitation of the number of articles included in this study.
Trial registration:
This systematic review protocol was prospectively registered with PROSPERO (No. CRD42024589435).
Introduction
Muscular atrophy refers to the limitation or extensive reduction of muscle volume, occurring in aging and other clinical conditions. 1 This process of muscle mass or strength loss is closely related to age as well as a normal physiological response to muscle lack of load. 1 Muscular atrophy is considered to be the most common process in sarcopenia-related disorders and cachexia. There is no consensus definition or common classification system of muscular atrophy to date. As an important public health issue, muscular atrophy mostly occurs at the late stage of diseases, with an estimated prevalence varying from 24.2% to 40.4%. 2 Studies have found that muscular atrophy reduces patients’ daily living activity and extends the course of diseases. 3 Also, muscular atrophy is a risk factor for death in patients with cardiovascular disease, cancer, and respiratory diseases, 4 and may cause a significant socioeconomic burden. Muscular atrophy will negatively affect the clinical outcomes of chronic obstructive pulmonary disease (COPD) patients such as exercise capacity, dyspnea, acute exacerbation, and frailty. 5 However, previous reviews on muscular atrophy and COPD prognosis have focused on patients’ dyspnea, lung function, and exercise capacity, and few studies have explored the mortality risk. Therefore, the association between muscular atrophy and the mortality risk in COPD patients is inconclusive. In 2005, a 5-year cohort study 6 on patients with stable COPD showed that muscular atrophy may be an independent predictor for all-cause mortality in patients with COPD (RR = 1.96, 95% CI (1.21, 3.17), p < 0.001). Benz et al.’s 7 results from a large population of cohort study also suggested that sarcopenia is independently associated with all-cause mortality in patients with COPD (HR = 2.11, 95% CI (1.44, 3.09), p < 0.001), and sarcopenia may increase the mortality risk in patients with COPD. Contrarily, another study showed that there is no correlation between sarcopenia and mortality in patients with COPD (p < 0.05). 8 Our study aimed to conduct a systematic review of cohort studies related to muscular atrophy and COPD, explore the association between muscular atrophy and mortality risk in patients with COPD, and hopefully contribute to improving the reference for reducing mortality and promoting early recovery of patients with COPD.
Methods
Data sources and search strategy
Cohort studies on the association between muscular atrophy and COPD were searched from the establishment of the database to July 1st, 2023. The databases included PubMed, Web of Science, Embase, the Cochrane Library, the China Biomedical Literature Service System, China Biomedical Literature Service System (CINAHL), China National Knowledge Infrastructure (CNKI), the Wanfang database, and the WeiPu (VIP) database. Relevant references were manually searched for literature supplements simultaneously. This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines. 9
Taking the PubMed database as an example, the specific retrieval strategies are as follows: (“Pulmonary Disease, Chronic Obstructive” [MeSH] OR “COPD” [Title/Abstract] OR “COPD”[Title/Abstract] OR “chronic obstructive pulmonary disease”[Title/Abstract] OR “chronic obstructive airway disease”[Title/Abstract] OR “chronic obstructive lung disease”[Title/Abstract] OR “chronic airflow obstruction”[Title/Abstract] OR “chronic obstructive”[Title/Abstract] OR “pulmonary disease”[Title/Abstract]) AND (“muscular atrophy”[MeSH] OR “muscle weakness” [MeSH] OR “Sarcopenia”[Title/Abstract] OR “muscular atrophy”[Title/Abstract] OR “less muscle disease”[Title/Abstract] OR “muscle loss”[Title/Abstract] OR “muscle mass”[Title/Abstract] OR “muscle weakness”[Title/Abstract]).
Definition of muscular atrophy
We defined muscular atrophy as a loss of muscle mass due to aging or any underlying illness with or without decreases in muscle function or fat tissue wasting.4,10 Based on previous studies, we included studies that reported muscular atrophy of any severity under any definition criteria.
Study selection
Inclusion criteria
Domestically and internationally published cohort studies on the association between muscular atrophy and COPD. The exposure factor was the comorbidity of muscular atrophy. The primary outcome was all-cause or cause-specific mortality. The secondary outcome was prolonged length of hospital stay.
Exclusion criteria
Reviews, editor’s letters, dissertations, conference summaries, low-quality articles with Newcastle–Ottawa Scale (NOS) < 5, and non-Chinese and non-English literature were excluded.
Data extraction
EndNote was used to check the search results and eliminate duplicates. Two researchers with evidence-based training independently screened the articles and extracted data according to the inclusion and exclusion criteria. In case of disagreement, the dispute shall be settled through discussion, if necessary, arbitrated by a third person. If data were missing or ambiguous in the literature, contact the first author for verification.
Data is extracted from eligible articles using a standardized form. The form included the first author, publication year, country, study design, sample size, source of study subjects, age, sex, follow-up duration, assessment method of muscular atrophy (standard and cut-off value), outcome indicators, and adjusted factors.
Methodological quality assessment
The quality of cohort studies was evaluated by the NOS. 11 Two researchers independently evaluated the quality of cohort studies, and disagreements were discussed or resolved by a third person. The NOS scale has 3 dimensions with a total of 8 items, including the selection of research subjects (4 items, 4 points), comparability between groups (1 item, 2 points), and outcome measurement (3 items, 3 points). The total score is 9, a score of < 5 is low-quality studies, and a score of ⩾5 is high-quality studies. The Grading of Recommendation, Assessment, Development, and Evaluation approach was used to assess the quality of evidence for outcomes.
Statistical methods
RevMan 5.4 (Copenhagen: The Cochrane Collaboration) was used for Meta-analysis. HR was the effect index, and the interval was estimated with 95%CI (according to the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0, HR≈RR). The chi-square test was used to analyze the heterogeneity of the results among the studies, and the test level was α = 0.10. Without statistical and clinical heterogeneity (p > 0.1, I2 < 50%), a fixed-effect model was used for meta-analysis. If there was moderate or above statistical heterogeneity but no clinical heterogeneity among the results of each study (p ⩽ 0.1, I2 ⩾ 50%), subgroup analysis or sensitivity analysis could be performed. If there was no obvious source of heterogeneity, a random-effects model would be used for meta-analysis, and the test level of meta-analysis was set at α = 0.05.
Results
Search results and characteristics of included studies
A total of 5,172 relevant studies were initially detected. Then, 3,944 studies were obtained after removing the duplicates, and 50 studies were obtained after reading the title and abstract. Finally, 13 cohort studies were included in the systematic review. Twelve of the 13 studies are prospective cohort studies while the other is retrospective. Also, a total of seven cohort studies6,7,12 –16 were included in the Meta-analysis. The PRISMA flow diagram of the literature search and selection is demonstrated in Figure 1.

Preferred reporting items for systematic reviews and meta-analyses flow diagram of article selection.
All cohort studies were evaluated by the NOS quality evaluation scale, and the scores were > 5 points, indicating that they were high-quality studies. The results of the quality assessment of the included studies are shown in Table 1. The basic characteristics of the included studies are shown in Table 2.
Methodological quality evaluation results of the included studies.

Basic characteristics of the included studies (N = 13).

BIA, bioelectric impedance analysis; BMI, body mass index; CC, Calf circumference; COPD, chronic obstructive pulmonary disease; DXA, dual-energy X-ray absorptiometry; EWGSOP-2, European Working Group of Sarcopenia in Older People; FEV1, Forced expiratory volume in one second; FFMI, Fat-Free Mass Index; LOS, length of stay; MAMA, Mid-arm muscle area; mMRC, modified British medical research council; PaO2, Partial Pressure of Oxygen; PM, pectoralis muscle, PMA, pectoralis muscle area; SGRQ, St George’s Respiratory Questionnaire; %ΔESM = ([ESMCSA at 2nd evaluation] – [ESMCSA at baseline])/[ESMCSA at baseline], the cross-sectional area of erector spinal muscle (ESMCSA).
In our study, six studies assessed muscular atrophy by Bioelectric Impedance Analysis (BIA), four studies assessed by CT, and other assessment methods Dual Energy X-ray absorptiometry (DXA) and Calf circumference.
Meta-analysis
The association between muscular atrophy and mortality risk
Seven studies reported the association between muscular atrophy and mortality in patients with COPD (Figure 2). Among the seven studies, Teixeira 15 reported the association between muscular atrophy and in-hospital mortality in patients with COPD while the other six studies reported all-cause mortality. Although the rest six studies16 –21 reported the association between muscular atrophy and mortality risk in patients with COPD, their muscular atrophy was represented by quantitative data that could not be statistically combined. As a result, they were not included in the meta-analysis. However, all the study results indicated that muscular atrophy was relevant to mortality risk in patients with COPD. Finally, the heterogeneity of the results of the included studies was I2 = 0%, so the fixed-effect model was adopted. Meta-analysis results showed that muscular atrophy increased the mortality risk in COPD patients (HR = 2.20, 95% CI (1.74, 2.79), p < 0.00001).
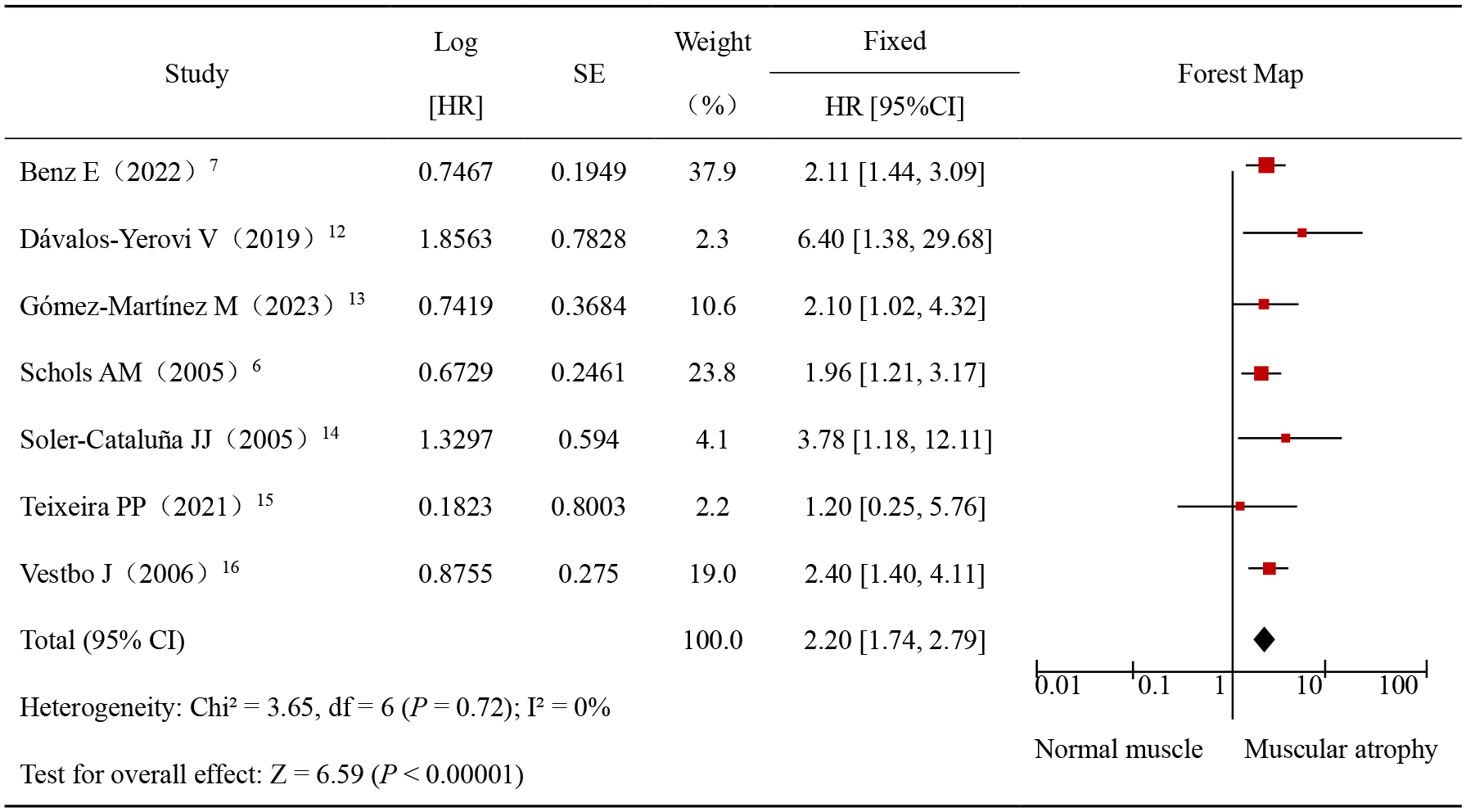
Meta-analysis of the effects of muscular atrophy on mortality in patients with COPD.
Association between muscular atrophy and mortality in patients with Stable COPD and AECOPD
The result of group analysis shows that muscular atrophy is associated with mortality in patients with Stable COPD and Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD). Muscular atrophy will increase the risk of all-cause mortality in patients with stable COPD (HR = 2.35, 95% CI (1.53, 3.60), p < 0.0001). Only Teixeira 15 reported the association between muscular atrophy and in-hospital mortality in patients with AECOPD (HR = 1.20, 95% CI (0.25, 5.76)). The subgroup analysis result is shown in Figure 3.

Subgroup analysis of the effects of muscular atrophy on mortality in patients with stable COPD and AECOPD.
Descriptive analysis of muscular atrophy versus length of hospital stays
In the included studies, two cohort studies12,15 reported the association between muscular atrophy and length of hospital stay, therefore meta-analysis could not be performed. A descriptive analysis was conducted instead. After adjusting the variables of sex and mMRC, the results of multivariate analysis from Teixeira’s study 15 showed that muscular atrophy in AECOPD patients was independently correlated with prolonged length of stay (Hospital stay > 11 days; OR = 2.25, 95% CI (1.1, 4.61), p = 0.026). According to the other study, 12 the patients with COPD who also had sarcopenia indicated a stronger relevance to a prolonged hospital stay (Hospital stay > 10 days) after adjusting for age (OR = 6.27, 95% CI (1.74, 22.53), p = 0.005). These findings suggest that muscular atrophy may prolong hospital stay in patients with COPD.
Sensitivity analysis and publication bias
Sensitivity analysis was conducted by eliminating studies one by one and studies with small sample sizes. The results showed that muscular atrophy increased the mortality risk in COPD patients, and the combined effect size did not change significantly, thus, the results were stable. As the number of studies included in the meta-analysis was <10, publication bias was not analyzed.
Discussion
This study suggested that muscular atrophy increases the mortality risk in patients with COPD, resulting in a worse disease prognosis when compared to COPD patients without muscular atrophy. However, the specific mechanism between muscular atrophy and the mortality risk in patients with COPD is still unclear. The mechanism may be the interactive association between muscular atrophy and respiratory dysfunction. Studies have shown that chronic hypoxia can induce muscular atrophy in patients with COPD. Muscle strength declines by 1%–2% per year 23 in healthy elderly people, while muscle strength declines by about 4.3% per year 24 in patients with COPD. In return, respiratory muscles assist the patient’s ventilatory function. Respiratory muscle dysfunction will limit the patient’s respiratory function. As a result, it may worsen the underlying chronic respiratory failure frequently present in patients with COPD and consequently may increase the risk of death in COPD patients, 25 especially in advanced stages. Research confirms that reduced the pectoralis muscle area (PMA) assessed by chest CT, leads to an increased risk of death in patients with COPD.20,22 Routine chest CT examination in patients with COPD also provides an opportunity to assess muscle mass in patients with COPD.
Skeletal muscle dysfunction affects both respiratory and limb muscles with limb muscles largely the focus of sarcopenia treatment and management in COPD. 26 As the quadriceps is a major locomotor muscle, it has been chosen as the best option for studies on the limb muscle dysfunction of COPD patients. Research has shown that quadriceps femoris muscular atrophy is the most common in patients with COPD. The quadriceps femoris muscle strength in patients with COPD is reduced by 20%–30% 27 compared to normal individuals. Reduced muscle mass as measured by mid-thigh cross-sectional area was, indeed, shown to negatively influent COPD mortality. 17 The conversion of quadriceps femoris muscle fiber types and muscle oxidative phenotypes may lead to decreases in skeletal muscle energy utilization and exercise endurance, accompanied by airway obstruction, leading to ‘forced braking’ in COPD patients. 28 Thus, the formation of a vicious cycle of ‘decreased activity-skeletal muscle function is impaired-increased dyspnea’ 29 increases the mortality risk in COPD patients, which is more common in AECOPD patients. 30
This study shows that muscular atrophy affects the mortality of both stable COPD and AECOPD. Acute exacerbations also impair respiratory muscle function as they severely affect whole-body muscle mass.31,32 Additionally, the need for respiratory muscle to overcome the inspiratory loads imposed by the increased ventilatory demands occurring during COPD acute exacerbations further impairs respiratory muscle function in these patients. The above factors can indirectly increase the risk of death.
In addition, the study found that muscular atrophy may lead to an extended stay in the hospital of COPD patients and slow recovery, which may increase family and socioeconomic burdens. At the same time, muscular atrophy has a high incidence in patients with COPD, which will exacerbate the adverse outcomes. Byun et al. 33 showed that the prevalence of muscular atrophy in COPD patients was 25%, while the prevalence of muscular atrophy in the same disease group in China was 28.1%. 34 Muscular atrophy not only further reduces the ability of daily activities in COPD patients, but also increases the risk of falls, pressure sores, fractures, and death,35,36 leading to a poor prognosis and prolonged hospital stay. Furthermore, studies have shown that patients with COPD are often admitted to the hospital for acute exacerbation. 37 The accelerated muscle deterioration in AECOPD patients, with more significant muscular atrophy, accompanied by worsening lung function, may also be the reason for the extended hospital stay in COPD patients.
In summary, muscular atrophy exerts a deleterious effect on the prognosis of patients with COPD. Hence, it is essential to know the therapeutic options for muscular atrophy. Exercise training has been shown to be the most viable treatment for muscular atrophy. 38
Effective exercise can ameliorate and even reverse the process of muscular atrophy. Studies showed that resistance training is an effective method for increasing skeletal muscle mass. 39 In a study by Constantin et al., 40 59 patients with COPD underwent knee extensor resistance training for 8 weeks, and it was found that the participants experienced an increase in both muscle mass and muscle strength. Also, nutritional support is considered a protective factor against muscular atrophy, including the intake of protein-rich, vitamin-enriched nutritional supplements, as well as the use of fish oils (omega-3 polyunsaturated fatty acids; PUFA). 41 In addition, as researchers gain a deeper understanding of the pathogenesis of muscular atrophy, a variety of drugs that modulate protein synthesis and degradation have gradually been employed in the treatment of muscular atrophy. However, their safety has not yet been established. 42 Therefore, a comprehensive intervention through exercise intervention, nutritional support, and pharmacological treatment may offer new perspectives for the management of muscular atrophy in patients with COPD.
Strengths and limitations of this study
This study has several advantages. First, according to our knowledge, this is the first meta-analysis to comprehensively evaluate the association between muscular atrophy and mortality risk in patients with COPD. Second, we included cohort studies from different countries, which are more comprehensive than a single study. In addition, the heterogeneity of the meta-analysis was 0, and the studies were highly homogenous, making the results of the meta-analysis relatively reliable.
Nevertheless, there are some limitations in this study. First of all, since the evaluation indicators of muscular atrophy could not be statistically combined, few cohort studies were finally included in the meta-analysis. In addition, few cohort studies regarded the length of hospital stay as an outcome, so only descriptive analysis was conducted.
Conclusion
To conclude, muscular atrophy is a risk factor for death in patients with COPD, and it may prolong the length of hospital stay. Therefore, clinical medical staff need to pay attention to the impact of muscular atrophy on the prognosis of patients with COPD, enhance the awareness of early warning, and strengthen disease prevention and management. If necessary, early screening of muscular atrophy in COPD patients and effective intervention measures could be taken to improve the prognosis of patients with COPD.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241304626 – Supplemental material for Association between muscular atrophy and mortality risk in patients with COPD: a systematic review
Supplemental material, sj-docx-1-tar-10.1177_17534666241304626 for Association between muscular atrophy and mortality risk in patients with COPD: a systematic review by Wenyan Li, Ying Wu, Xun Yang, Jing Zhu, Mei Feng, Rong Deng, Cui Yang and Chengcheng Sun in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.