
Abstract
Background:
Upper limb (UL) muscle dysfunction is a common extrapulmonary manifestation of chronic obstructive pulmonary disease (COPD). UL muscle dysfunction is associated with muscle weakness, dyspnea, and exercise intolerance. Although upper limb exercise training (ULET) is typically incorporated in pulmonary rehabilitation programs, its effects on UL muscle strength remains unclear.
Objectives:
The purpose of this systematic review was to investigate the effectiveness of ULET, in UL muscle strength of people with COPD.
Design:
This is systematic review and meta-analysis study.
Data Sources and Methods:
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Protocols 2020 guidelines were used for this study. PubMed, Cochrane, CINAHL Plus and SPORTDiscus and clinicaltrials.gov registry were searched from inception to July 2022. Included studies were randomized controlled trials, assessing the effectiveness in muscle strength of ULET, compared with other types of upper or lower limb exercise or no exercise. The quality and risk of bias were assessed using the Physiotherapy Evidence Database (PEDro) scale and certainty of evidence with the Grading of Recommendations, Assessment, Development, and Evaluations approach. Treatment effects of ULET were calculated using standardized mean differences and 95% confidence intervals.
Results:
Twenty-four studies, with a total sample of 882 patients, were included. Most studies were of moderate quality and high risk of bias. Very low to low certainty evidence indicates a significant difference in UL muscle strength in favor of resistance ULET, compared with lower limb exercise alone or no exercise. No significant differences were found in different types of ULET comparisons.
Conclusion:
The results of this review showed that resistance ULET could improve UL muscle strength in people with COPD. Most studies, however, were of moderate quality and high risk of bias. Further studies with larger sample sizes, better methodological quality, and standardized training protocols are needed to confirm these findings.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disease, which can also affect other body organ systems, such as cardiovascular and musculoskeletal systems.1,2 Pathophysiological changes driven by COPD in the musculoskeletal system are associated with physiological alterations of peripheral muscles.3,4 Muscle weakness of the upper limbs (ULs) is evident in people with COPD and has a clinical and a prognostic value as it is associated with reduced muscle mass, reduced distance walked in 6-minute walk test, 5 and increased hyperinflation 6 and dyspnea. 7
Exercise training is one of the main components of pulmonary rehabilitation (PR) and has been found to improve skeletal muscle function and morphology in people with COPD.3,8,9 In order to achieve muscular improvements, however, the exercise program should be specific and tailor to the muscles of interest. Although a detailed assessment of muscle function is recommended in the PR practice, 10 it seems that muscle strength receives less attention. 11 Moreover, literature and clinical practice focus mostly on quadriceps muscle strength, 3 and in many cases, skeletal muscle function and strengthening of the UL are not addressed at all. 11 Recent reviews stress the need that all muscle groups (including UL muscles) should be tested in order to aid in the design and individualization of exercise programs or to evaluate their effectiveness.10–12
The inclusion of upper limb exercise training (ULET) is not specifically suggested for people with COPD, according to the British guidelines on PR in adults. 13 This lack of suggestion is probably driven by the conflicting evidence about the effectiveness of ULET in COPD patients’ muscle strength, despite the link between ULET and improvements in UL function. 14 Specifically, current evidence suggests that ULET when compared with no exercise improves dyspnea symptoms but not UL muscle strength in people with COPD. 15 In addition, the limited available number of evaluated studies in a Cochrane systematic review 15 implemented different UL training interventions making it hard to conclude the optimal ULET program for people with COPD. Moreover, a recent meta-analysis report that resistance exercise compared with no exercise could significantly improve muscle strength in people with COPD. The analysis, however, did not concern solely ULET and UL muscle groups, as it calculates strength results of all resistance training groups, irrespective whether they perform UL or lower limb (LL) training. 16 The main objectives of this systematic review and meta-analysis were to evaluate the effect of ULET in UL muscle strength in people with COPD and to determine the most effective exercise parameters and inform clinical practice, based on the available randomized controlled trials (RCTs).
Methods
Protocol registration and guidelines
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 17 followed recommendations of the Cochrane Handbook for Systematic Reviews, 18 and the protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO – CRD42020210565).
Information sources and search strategy
A systematic search, from inception to July 2022, was independently conducted by two reviewers (G.P. and C.K.) using the following electronic databases and trial registries: PubMed, Cochrane, and EBSCO Host databases (CINAHL Plus and SPORTDiscus). Gray literature was searched through clinicaltrials.gov registry. Hand-searching in reference lists of citation tracking results and systematic reviews was also conducted.
The search strategy included four basic strings of key terms combined with Boolean operators in all fields: (a) related to the condition investigated (COPD, chronic obstructive pulmonary disease, chronic obstructive lung disease, chronic obstructive airway disease, emphysema, chronic airflow limitation, chronic airway obstruction), (b) focusing on the UL (arm, upper extremity, upper limb), (c) identifying the intervention (exercise therapy, exercise, respiratory rehabilitation, pulmonary rehabilitation, physical exercise, physiotherapy, physical therapy, training), and (d) specifying outcome measure (strength, muscle strength).
Study selection
The search results were initially screened by two reviewers (independently), and the duplicates were removed. Titles and abstracts of potentially relevant articles were screened, and subsequently, the full-text study was retrieved and compared against the eligibility criteria. Any disagreement was resolved with the involvement of a third reviewer (C.S.) in a consensus process.
Inclusion criteria
Study selection and eligibility were based on the ‘participant’, ‘intervention’, ‘comparator’, ‘outcome’, ‘study type’ (PICOS) model. 19 Included studies were RCTs in English language (S); including adults (⩾18 years) at any stage of COPD, who participated in a PR program lasting at least 6 weeks (P); 13 comparing (directly or indirectly) a form of ULET (I); and with lower extremity exercise training only or sham intervention or other type of ULET (C). Outcomes included any objective measure of UL muscle strength with no restrictions regarding the assessment method used [e.g. 1 repetition maximum (1RM), hand-held dynamometry] (O). Reviews, studies with study design other than RCT, and conference abstracts were excluded. No limitation was set with regard to publication year, condition severity, age, sex of the participants, and follow-up time.
Data extraction
A customized Excel spreadsheet was used for data extraction.15,20 Data were extracted on the study characteristics (study design, total duration of study, details of any run-in period, study setting, withdrawals, and date of study), the participant characteristics (sample size, mean age, sex, severity of COPD, diagnostic criteria, baseline lung function, smoking history, inclusion criteria, and exclusion criteria), the interventions (intervention and comparison groups), the measures of effect and variability (primary and secondary outcomes at baseline and reported follow-up time points), and added notes on funding and conflicts of interest.
Data presented in graphs were extracted using the plot digitizer software (http://plotdigitizer.sourceforge.net/)21,22 that is by systematic review guidelines. 23 The analyses and presentation of the results were categorized according to the follow-up into very short-term (<8 weeks), short-term (⩾8 weeks to ⩽12 weeks), mid-term (>12 weeks to <52 weeks), and long-term (⩾52 weeks).24,25
Quality and risk of bias assessment
The quality and risk of bias of each study were assessed independently by two investigators (C.K. and C.S.) using the Physiotherapy Evidence Database (PEDro) scale, 26 which is considered a valid and reliable tool.27,28 The PEDro scale consist of 10 items assessing randomization process, participant group allocation, blinding, participant characteristics, and reporting. A PEDro score of ⩾7/10 indicated a study as of ‘high quality’, studies with a score of 4–6/10 of ‘moderate quality’ while those with scores of ⩽3 were deemed of ‘low quality’.20,29 A PEDro score <7 determined a study as having ‘high’ risk of bias. 30
Data analysis and measures of treatment effect
The data analysis was performed using Review Manager V.5.4 and followed the recommendations of the Cochrane Handbook. 18 We expected a significant variability in study setting; thus, we assessed the treatment effects using random effect model to calculate the standardized mean differences (SMDs). If only one study was available, we calculated the effect size as a mean difference (MD) using a fixed effect model. The statistical heterogeneity of the studies was assessed using I2 statistic. Values ranging from 0% to 25% indicated low heterogeneity, values from 26% to 75% moderate heterogeneity, and values from 76% to 100% high heterogeneity. 31 If considerable between-group statistical heterogeneity was detected (i.e. I2 > 75%), we did not perform a meta-analysis, but proceeded with sensitivity analyses. For each time point analysis, we used the respective sample size adjusted for loss to follow-up (where applicable). Reporting bias was evaluated by funnel plots with 10 or more studies.
Results were presented as summary tables and forest plots with total and subtotal values where applicable. 18 Forest plots were presented only if aggregate pooled estimates met the predefined homogeneity criteria.
Certainty of evidence
The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach was used to evaluate the certainty of evidence, 18 performed independently by two reviewers (C.K. and G.P.), while a third author (V.K.) was consulted in any disagreement.32,33 The certainty of evidence was rated as ‘high’, ‘moderate’, ‘low’, or ‘very low’, depending on presence and extent of limitations in five domains as indicated by the GRADE methodology. All outcomes were considered of high certainty of evidence and were downgraded based on: (1) risk of bias (if the ‘low risk’ studies contributed less than 50% of participants in the pairwise comparison), (2) inconsistency [poor overlap of the confidence intervals (CIs) in forest plots; inconsistent magnitude and direction of the effects; and substantial heterogeneity, that is, p value from χ2 test, or CI for I2, or Q-statistic and degree of freedom (df), or the between-study variance–Tau 2 ], (3) indirectness [if clinical heterogeneity was present in participants characteristics such as age, sex, and severity of the condition according to the Global Initiative for Obstructive Lung Disease (GOLD) criteria], 34 (4) imprecision of treatment effects (>20% attrition and upper or lower 95% CI spanned an effect size of 0.5 in either direction), and (5) publication bias.35,36 We graded an outcome a priori with only one trial as low certainty, and if the study had also high risk of bias, the evidence was graded as of very low certainty. 37
Subgroup and sensitivity analyses
Sensitivity analyses were performed examining: (1) unexpectedly large treatment effect sizes and ‘leave-one-out’ exclusion, (2) studies contribution where heterogeneity was substantial (I2 > 50%), and (3) studies presenting significant heterogeneity at baseline for participant characteristics. Also, we aimed to perform analyses by subgrouping studies according to various differences concerning patient characteristics (e.g. COPD severity, participant sex), type of intervention, or assessment methods where applicable.
Results
We identified 297 potentially relevant studies from database search and 19 studies from citations search (total 316 studies). Thirty-three of them were full-text screened for inclusion. Twenty-four studies (882 total people with COPD) met the eligibility criteria and were included in the systematic review (Figure 1).

Flowchart of the record selection process.
Quality and risk of bias assessment
The quality of the included studies ranged from 3 to 9 on the PEDro scale (Supplementary Table 1). Most of the studies were of moderate quality, and 71% of the studies rated as presenting ‘high’ risk of bias.
Participant characteristics
The eligible studies included mostly males and the pooled mean age of the participants was 65.3 years (range = 49–71.5 years). The number of participants randomized per trial ranged from 19 to 64, and in most of the studies, the participants had moderate to severe COPD according to the GOLD criteria 34 (Table 1).
Participant and study characteristics.

BMI, body mass index; CG, comparator group; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in the first second; LL, lower limb; LLEET, lower limb endurance exercise training; LLRT, lower limb resistance training; N/A, not available; PEDro, Physiotherapy Evidence Database; SD, standard deviation; UG, upper limb group; UL, upper limb; ULEET, upper limb endurance exercise training; ULRT, upper limb resistance training.
BMI was calculated from reported participant data on height and weight.
Data of sex, age, FEV1%, and BMI concern the baseline sample size (patients who lost to follow-up and discontinue the study are not excluded).
Several COPD diagnostic criteria were used among those studies, with spirometry most frequently used. One study did not report any information for the clinical diagnosis of COPD, 54 while three studies included the presence of dyspnea and fatigue during activities of daily living or with upper-body activities as an inclusion criterion.46,48,52
The presence of a COPD exacerbation between 3 weeks and 3 months prior the study was considered as an exclusion criterion in eight of the included studies.46–48,50–52,58,59 Two studies reported that subjects should not have a recent exacerbation without any other details,38,54 while seven studies recruited only non- or ex-smokers.42,50,51,55–57,59 Only one of the studies examined the effects of exercise training immediately after an exacerbation and participants followed an early rehabilitation program within 10 days of hospital discharge. 53
Exercise program characteristics
Different UL exercise programs were performed in the included studies. Most studies contain UL resistance training with weights or elastic bands or tubes (with or without LLET). The frequency, intensity, and time of intervention vary between studies with most studies have a frequency of two to three times a week, for 8–12 weeks. Intensity was set mostly from the results of 1RM assessment, and usually patients perform 2–4 sets of 8–12 repetitions with a load 50–85% of 1RM (Supplementary Table 2). A summary of exercise parameters and a suggested program is available on Table 2.
Summary of training parameters and a proposal of an exercise training program for increase of upper limb muscle strength.
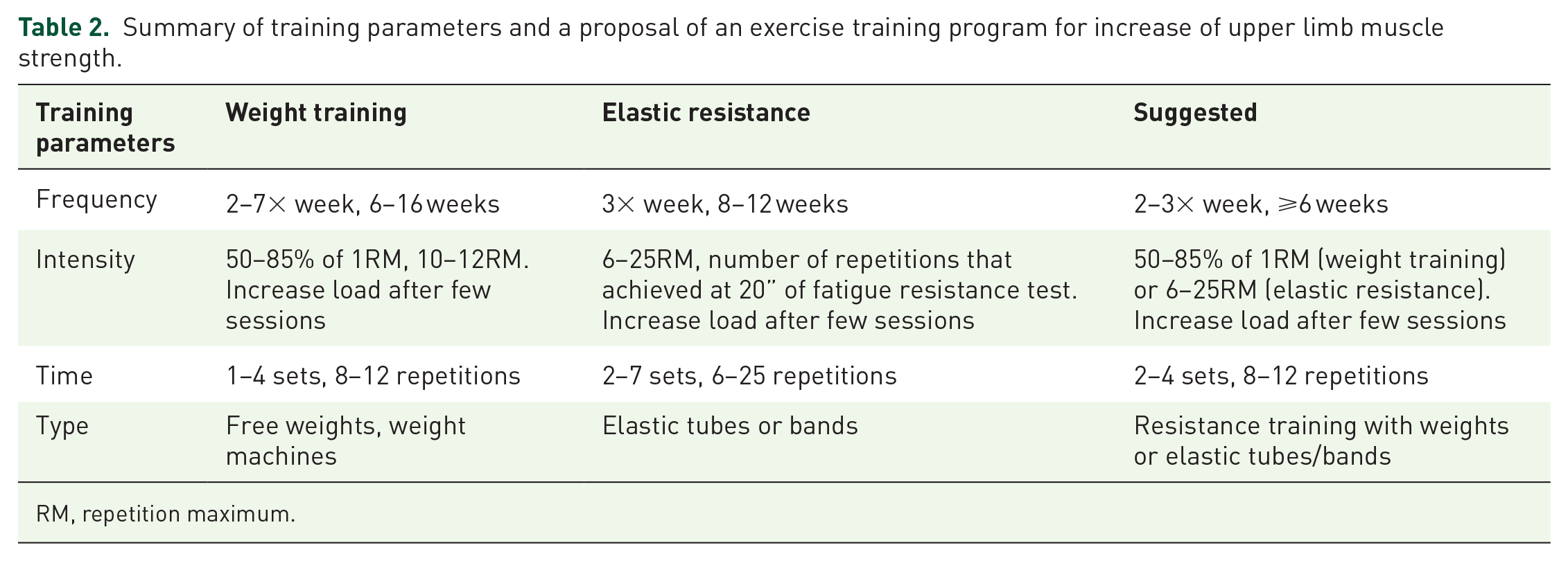
RM, repetition maximum.
Strength assessment of the UL
Various muscle groups and different assessment methods were used for the evaluation of the UL muscle strength among studies (Supplementary Table 2). The most common assessment methods were 1RM, maximal isometric strength, maximal isokinetic strength, and handgrip strength. Elbow flexors, shoulder flexors and abductors, latissimus dorsi, and pectoralis major were the most frequently assessed muscles.
Comparisons and effects of interventions
The included studies present clinical heterogeneity in terms of comparator interventions (Table 1 and Supplementary Table 2); hence, the results are separated and presented as three main categories/comparisons: (1) combined ULET and lower limb exercise training (LLET) compared with LLet alone; (2) ULET compared with no exercise; and (3) ULET (with or without other interventions) compared with another type of ULET.
Combined UL and LLET compared with LLet alone
Five studies (171 patients) compared combined UL and LL resistance training (plus LL endurance training) with LL endurance training alone.8,41,42,49,51 Three studies had a group that performed only resistance training.41,49,51 All studies reported on the strength of pectoralis major. The training parameters were variable among studies (sets ranging from 1 to 4, repetitions from 6 to 15, and load from 60% to 85% 1RM) (Supplementary Table 2). All studies evaluated outcomes at the short-term follow-up (⩾8 and ⩽12 weeks), while one study reported outcomes at the 24-week follow-up. 41
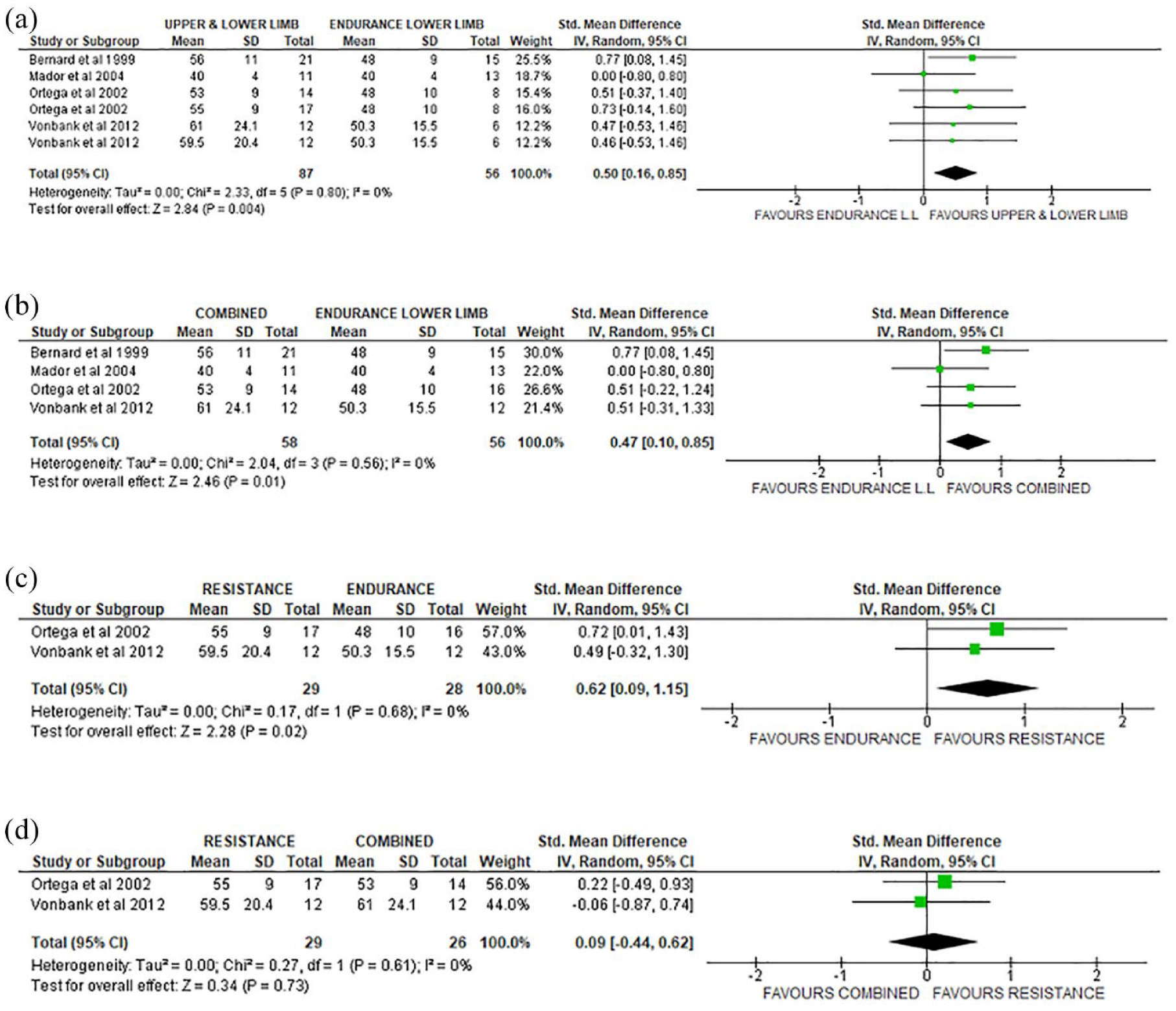
Very low certainty evidence indicates a significant difference in pectoralis major (SMD = 0.50, 95% CI = 0.15, 0.85) (Figure 2(a)) and in latissimus dorsi strength (SMD = 0.50, 95% CI = 0.16, 0.85) (Figure 3(a)), in favor of the resistance ULET (with or without LL endurance training) group, compared with LL endurance training only, at the short term (Table 3). Subgroup analysis showed very low certainty evidence (Table 3) that both UL and LL resistance training (without endurance training) and combination of UL and LL resistance and endurance LL training could significantly increase muscle strength of pectoralis major (Figure 2(c)) and latissimus dorsi (Figure 3(b) and (c)), compared with LL endurance training. The only between-group comparisons that did not reveal significant differences in any muscle group or follow-up were UL and LL resistance exercise compared with a combination of resistance and endurance exercise training (Figures 2(d) and 3(d) and Supplementary Figures 4 and 7).

Forest plot of muscle strength comparison for pectoralis major (short term) (a) resistance UL and LL + combined resistance UL and LLET and endurance LL versus endurance LL training alone, (b) subgroup analysis of combined resistance UL and LLET and endurance LL versus endurance LL training alone, (c) subgroup analysis of resistance UL and LLET versus endurance LL training alone, and (d) resistance UL and LLET versus combined resistance UL and LLET and endurance LL.
Forest plot of muscle strength comparison for latissimus dorsi (short term) (a) resistance UL and LL + combined resistance UL and LLET and endurance LL versus endurance LL training alone, (b) subgroup analysis of combined resistance UL and LLET and endurance LL versus endurance LL training alone, (c) subgroup analysis of resistance UL and LLET versus endurance LL training alone, and (d) resistance UL and LLET versus combined resistance UL and LLET and endurance LL.
Summary of evidence for the effectiveness of upper limb exercise training.

CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development, and Evaluations; LL, lower limb; LLET, lower limb exercise training; SMD, standardized mean difference; UL, upper limb; ULET, upper limb exercise training.
Downgraded due to risk of bias.
Downgraded due to inconsistency.
Downgraded due to indirectness.
Downgraded due to imprecision.
In sensitivity analyses, by removing a study that did not reported on sex configuration, 42 all comparisons showed significant differences in favor of the group that performed ULET (Supplementary Figures 1(b), 2(b), 5, and 6 and Supplementary Table 3). At the mid-term follow-up (24 weeks), low certainty evidence suggests significant differences in favor of the UL and LL training compared with LL endurance training alone for neck press (SMD = 0.85, 95% CI = 0.22, 1.49; p = 0.008) (Figure 4(c) and Table 3).

Forest plot of muscle strength comparison between resistance UL and LL + combined resistance UL and LLET and endurance LL versus endurance LL training alone (mid-term): (a) pectoralis major, (b) latissimus dorsi, and (c) deltoid and triceps (neck press).
ULET compared with no exercise or sham intervention
Eleven studies (441 patients) compared ULET with no exercise or sham intervention (Supplementary Table 2).38–40,44,46–48,51–53,59 In 10 studies, patients performed combined UL and LL exercises, while in one study, 48 the intervention involved only ULET. The intervention group performed resistance exercises with46,53 or without endurance training.38,44,48,59 Three studies had two exercise arms compared with a third control group;48,51,53 owing to lack of exercise detail in one study, one arm was excluded from analysis. 53 In the study of Clark et al., 39 ULET was performed without resistance. The frequency of exercise training was three times per week in most of the included studies, whereas the total duration of training ranged between 6 and 16 weeks. Three studies included home training sessions as part of their training program.39,44,48
Significant differences in favor of the ULET group were observed (Table 3 and Figure 5) at the short-term follow-up in elbow flexors (SMD = 0.77, 95% CI = 0.27, 1.26) and chest press strength (SMD = 1.51, 95% CI = 0.90, 2.11), and at the long-term follow-up in the upper-body strength (SMD = 0.72, 95% CI = 0.11, 1.34). Sensitivity and subgroup analyses did not change the direction or the size of the effect (Figure 5(c) and Supplementary Figure 8).

Forest plot of muscle strength comparison between UL exercise and no exercise: (a) elbow flexors (short term), (b) upper body (long term), (c) resistance UL and LLET + combined resistance UL and LLET and endurance LL versus no exercise (pectoralis major) (short term), and (d) subgroup analysis of combined resistance UL and LLET and endurance LL versus no exercise (pectoralis major) (short term).
Substantial heterogeneity in strength assessment method, UL muscles evaluated, or training program allowed only single study effect size calculation for the rest of the studies of this category (Supplementary Figures 9–14).
Comparison of different types of ULET
Nine studies (283 patients) compared UL and LL training with different types of UL exercise with significant variability in the exercise and the exercise programs (Supplementary Table 2).9,43,45,50,54–58 Four studies compared training with elastic resistance to weight machines;50,54,56,57 two studies compared endurance training with combined endurance and resistance training;43,45 one study compared resistance training and diagonal movements with diagonal movements only, 55 and two studies compared resistance with endurance training 9 and resistance with combined training. 58
Very low certainty evidence indicates a nonsignificant difference between elastic resistance exercise and weight machines training in all muscle groups at the short-term follow-up (Figure 6 and Table 3). In sensitivity analysis (Supplementary Figures 20 and 21 and Supplementary Table 3) by removing heterogeneous studies,56,57 results did not change.

Forest plots of muscle strength comparison between resistance UL and LLET with weights versus resistance UL and LLET with elastic tubes (short term): (a) elbow flexors, (b) shoulder flexors, and (c) shoulder abductors.
Two studies comparing UL and LL endurance training to combined UL and LL endurance and resistance training43,45 presented high heterogeneity (89%), and we did not proceed with meta-analysis (Supplementary Figure 15). Very low certainty evidence from a single study indicates a significant increase in pectoralis major strength in favor of combined exercise group at the short-term follow-up (Supplementary Figure 15(b) and (c)). 43
Substantial differences among studies in strength assessment method, UL muscles training program, or time of intervention did not allow quantitative synthesis (Supplementary Figures 16–19). Only one study showed a significant difference in favor of the combined resistance ULET and diagonal movements group (MD = 1.30, 95% CI = 0.06, 2.54) at the short-term follow-up (low certainty of evidence) (Supplementary Figure 17).
Discussion
The objective of this systematic review and meta-analysis was to evaluate whether ULET could improve UL muscle strength in people with COPD. The results indicate that ULET could significantly improve UL muscle strength in both within-group and between-group in which the comparators did not perform ULET. Very low to low certainty evidence indicates a significant difference in UL muscle strength between resistance ULET compared with LLET exercise or no exercise. Comparison of different types of ULET or when ULET compared a combination of ULET and LLET, however, no significant changes were observed.
Five previous systematic reviews have examined the effectiveness of ULET in muscle strength in people with COPD.15,60–63 Three reviews have shown that resistance exercise could improve UL muscle strength, but all included limited number of studies in the meta-analysis (one to six).60–62 O’Shea et al. have not shown significant effects for all UL muscles. On the contrary, McKeough et al. have analyzed only three trials concerning UL muscle strength and found no significant between-groups difference when compared with no exercise or LL exercise only. Finally, in one other systematic review, authors investigate the efficacy of elastic resistance training. 63 They include five studies concerning ULET for meta-analysis, but no significant differences in UL muscle strength were found compared with no exercise (two studies analyzed) and conventional weight training (three studies analyzed). The results of the present systematic review were comparable with most reviews mentioned above, as resistance training seems to improve muscle strength, without significant difference among different types of resistance training.
Evidence suggests that activities with the UL could exacerbate dyspnea sooner and present higher fatigability compared with those activities involving the LL 64 in people with COPD. One of the possible reasons for this phenomenon is the established UL muscle weakness. 7 According to previous studies, resistance exercise training has the potential to improve muscle strength in healthy individuals;65,66 however, the current evidence for people with COPD is conflicting. 15 Our findings showed that UL resistance training plays a key role in the improvement of UL muscle strength, despite one of the two studies that did not report significant improvements (within- or between-groups) did not implement a resistance training component. 39 Nevertheless, it remains unclear if the improvements in muscle strength are maintained after the cessation of exercise. The evidence is still conflicting, with studies reporting that all the gains have been reversed at 12 weeks, 44 or others showing slight decrease but not reaching baseline values at the mid- and long-term follow-up.41,48
Based on the available evidence, an ideal program of UL resistance training in people with COPD could not be specified. In the meta-analysis of two types of resistance training (elastic resistance compared with weight training), we were not able to identify significant differences between them. In all studies that involve training with elastic bands or tubes, however, a significant within-group improvement in muscle strength has been reported.44,50,54,56,57,59 Thus, it could be an alternative and cost-effective way of training, even at home following an introductory educational session. 44
A substantial diversity of the other exercise parameters (frequency, intensity, time) has been reported from the included studies. Despite these differences, we try to summarize the parameters of training programs and it seems that resistance exercise of the UL (2–3 times a week) for at least 6 weeks could improve UL muscle strength. In addition, it could be assumed that weight training that consists of 2–4 sets, 8–12 repetitions with a load 50–85% of 1RM could be ideal in order to increase muscle strength in UL of people with COPD (Table 2). These parameters seem that are in accordance with a previous systematic review 16 and recent guidelines. 13
Muscle strength is only one part of the puzzle that characterizes the disabilities of these patients. To define the optimal ULET program for people with COPD, it should be taken into account its effectiveness on other condition specific and relevant outcomes. A previous systematic review has shown that both resistance and endurance ULET could improve dyspnea. 67 Previous reviews, however, have highlighted the uncertainty of the evidence with regard to the effectiveness of the ULET, along with the optimal exercise parameters on reduction of fatigue, the ability to perform activities of daily living and quality of life.20,67,68
We acknowledge several limitations in this study. First, the quality of the included studies was only moderate and most of them present high risk of bias. This is a reason why certainty of evidence ranging from low to very low in this study. Second, most included studies did not perform power calculation, and in some (pilot) studies, only a small sample was included in each group (⩽10 patients). Third, although it is well known that there are significant differences between men and women with COPD in muscle strength of UL and LL,69–71 the majority of studies included mostly males, limiting the generalizability of our findings in female patients with COPD. A fourth limitation was the diversity of the disease severity among studies and high attrition rate (>20%) presented in most of the studies. Previous studies have shown that muscle strength values were significant different in patients of different COPD stages.72,73 With regard to the attrition rates that could have probably influence the outcomes, most studies reported that patients discontinued intervention due to personal reasons not related with the exercise program. Finally, the high heterogeneities among studies in the strength assessment methods, units of strength reporting, and muscle groups evaluated, possibly affected the quantitative synthesis.
In conclusion, the current systematic review suggests that ULET including resistance training is an effective intervention to improve UL muscle strength at the short term, when compared with no exercise or LLet alone, in people with COPD. Moreover, resistance exercise with elastic bands or tubes could be an effective alternative method of conventional resistance training. More research is needed, however, with better quality of study design, in terms of allocation concealment, blinding, adequate follow-up and intention to treat analysis. Moreover in future studies sample sizes should be estimated through power calculation. In addition, it will be very useful to investigate the efficacy and the proper parameters of ULET training considering its effectiveness in other relevant outcomes such as symptoms, UL function, and activities of daily living. Finally, future studies should evaluate sex differences in response to ULET, the long-term results of strengthening interventions, and ways to maintain the benefits of the UL muscle strengthening in the long term.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231170813 – Supplemental material for The effects of upper limb exercise training on upper limb muscle strength in people with chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-tar-10.1177_17534666231170813 for The effects of upper limb exercise training on upper limb muscle strength in people with chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials by Christos Karagiannis, Christos Savva, Vasileios Korakakis, George Ploutarchou, Tonia Adamide, Andreas Georgiou and Theodoros Xanthos in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.