
Abstract
Background:
Ventilator-induced lung injury (VILI) presents a grave risk to acute respiratory failure patients undergoing mechanical ventilation. Low tidal volume (LTV) ventilation has been advocated as a protective strategy against VILI. However, the effectiveness of limited driving pressure (plateau pressure minus positive end-expiratory pressure) remains unclear.
Objectives:
This study evaluated the efficacy of LTV against limited driving pressure in preventing VILI in adults with respiratory failure.
Design:
A single-centre, prospective, open-labelled, randomized controlled trial.
Methods:
This study was executed in medical intensive care units at Siriraj Hospital, Mahidol University, Bangkok, Thailand. We enrolled acute respiratory failure patients undergoing intubation and mechanical ventilation. They were randomized in a 1:1 allocation to limited driving pressure (LDP; ⩽15 cmH2O) or LTV (⩽8 mL/kg of predicted body weight). The primary outcome was the acute lung injury (ALI) score 7 days post-enrolment.
Results:
From July 2019 to December 2020, 126 patients participated, with 63 each in the LDP and LTV groups. The cohorts had the mean (standard deviation) ages of 60.5 (17.6) and 60.9 (17.9) years, respectively, and they exhibited comparable baseline characteristics. The primary reasons for intubation were acute hypoxic respiratory failure (LDP 49.2%, LTV 63.5%) and shock-related respiratory failure (LDP 39.7%, LTV 30.2%). No significant difference emerged in the primary outcome: the median (interquartile range) ALI scores for LDP and LTV were 1.75 (1.00–2.67) and 1.75 (1.25–2.25), respectively (p = 0.713). Twenty-eight-day mortality rates were comparable: LDP 34.9% (22/63), LTV 31.7% (20/63), relative risk (RR) 1.08, 95% confidence interval (CI) 0.74–1.57, p = 0.705. Incidences of newly developed acute respiratory distress syndrome also aligned: LDP 14.3% (9/63), LTV 20.6% (13/63), RR 0.81, 95% CI 0.55–1.22, p = 0.348.
Conclusions:
In adults with acute respiratory failure, the efficacy of LDP and LTV in averting lung injury 7 days post-mechanical ventilation was indistinguishable.
Clinical trial registration:
The study was registered with the ClinicalTrials.gov database (identification number NCT04035915).
Plain language summary
We conducted this research at Siriraj Hospital in Bangkok, Thailand, aiming to compare two ways of helping patients with breathing problems. We studied 126 patients who were randomly put into two groups. One group received a method where the pressure during breathing was limited (limited driving pressure: LDP), and the other group got a method where the amount of air given to the lungs was kept low (low tidal volume: LTV). We checked how bad the lung injury was at seven days later. The results showed that there was no difference between the two methods. Both ways of helping patients breathe had similar outcomes, and neither was significantly better than the other in preventing lung problems. The study suggests that both approaches work about the same for patients who need help with breathing using a machine.
Keywords
Background
Invasive mechanical ventilation, frequently employed to assist critically ill patients, is increasingly identified as a potential factor exacerbating lung injury. Injuries may arise through various mechanisms, encompassing barotrauma, volutrauma and biophysical stress. 1 A lung-protective ventilation strategy termed ‘low tidal volume’ (LTV) has been established as an effective approach to curtailing ventilator-induced lung injury (VILI). The strategy focuses on averting alveolar overdistension and minimizing volutrauma. It has demonstrated improved outcomes in patients needing mechanical ventilation, especially those diagnosed with acute respiratory distress syndrome (ARDS).2,3
Nevertheless, the efficacy of the LTV strategy in mechanically ventilated patients without ARDS remains inconclusive. Data from small randomized controlled trials and meta-analyses have suggested that the LTV approach correlates with fewer pulmonary complications and reduced dependency on mechanical ventilation.4–8 By contrast, a recent large randomized controlled trial found no significant benefits. 9
A parallel strategy to mitigating VILI involves ventilation with limited driving pressure (LDP). Emerging evidence posits that elevated driving pressure correlates with increased pulmonary complications in both ARDS and non-ARDS perioperative patients.10,11 By contrast, diminished driving pressure has been linked to improved survival outcomes in ARDS patients. 12 However, a definitive consensus on whether LDP can prevent VILI in mechanically ventilated patients without ARDS remains elusive. Additionally, information is limited on whether to choose the LDP or the LTV strategy to prevent VILI in non-ARDS patients with acute respiratory failure who need mechanical ventilation.
This research aimed to compare the efficacy of the LDP and LTV approaches in preventing VILI among non-ARDS patients with acute respiratory failure who require mechanical ventilation. By assessing these methodologies, we sought to gain insights into the optimal ventilation approach for preventing lung injury in this patient population.
Methods
Study design
This prospective, randomized, unblinded clinical trial was conducted at the medical intensive care unit (ICU) of Siriraj Hospital, Mahidol University, Bangkok, Thailand. The study enrolled participants between 25 July 2019 and 31 December 2020. The coinvestigators performed all participant screening and enrolment procedures (Figure 1). Before enrolling patients, written informed consent for participation was obtained from the patients or, in cases where patients were unable to provide consent, their next of kin or legal guardians. The principal investigator and a statistician conducted the outcome evaluation data analysis, with both blinded to the patient’s treatment group. The Siriraj Critical Care Research Fund funded the trial. The funder had no role in the study design, data analysis or outcome assessment. The reporting of this study conforms to the CONSORT (Consolidated Standards of Reporting Trials) statement. 13
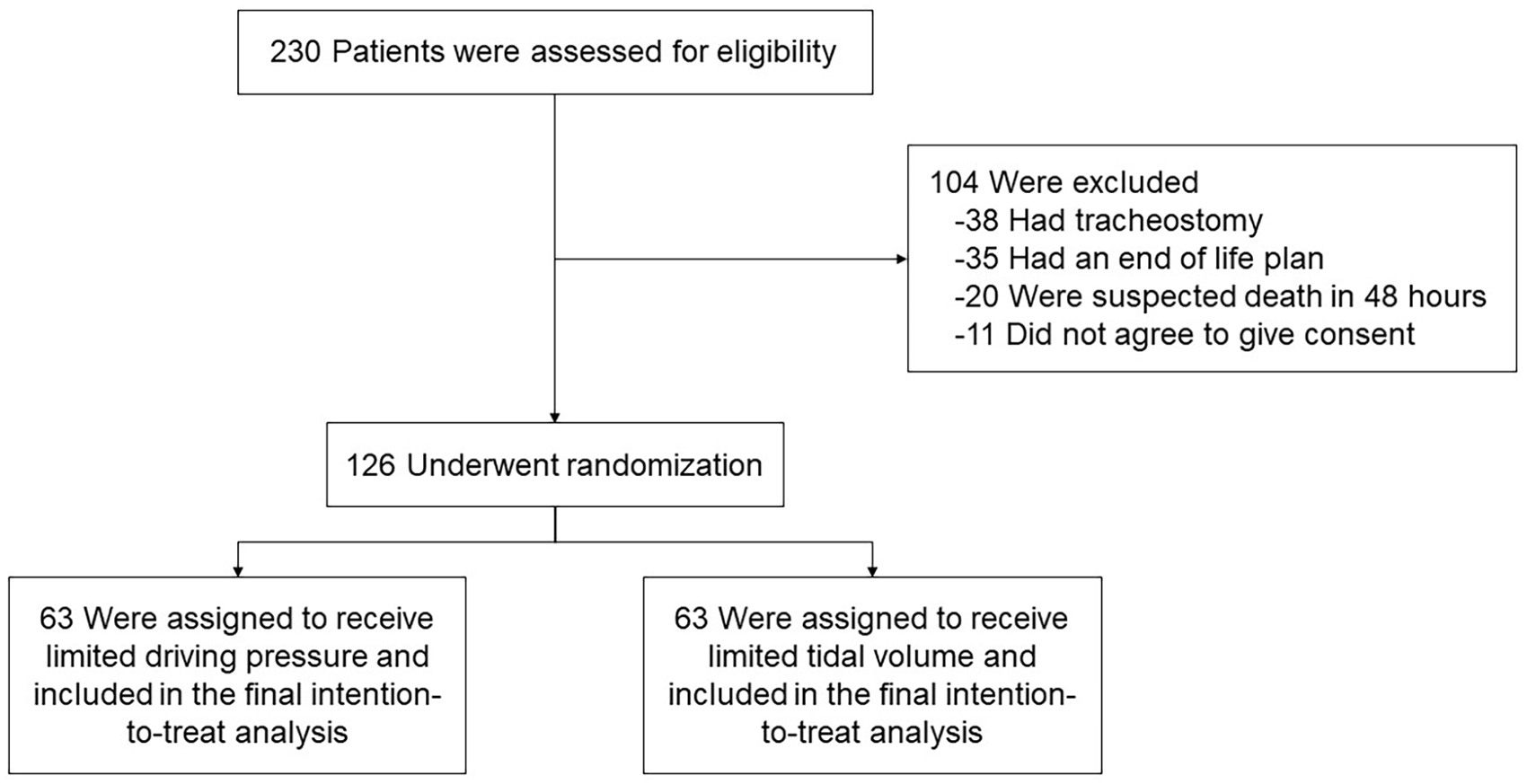
Flow diagram illustrating the screening, enrolment and randomization of the patients.
Participants
We screened all patients 18 years or older admitted to the medical ICU with acute respiratory failure. Patients were eligible if they had been intubated and placed on mechanical ventilation within 24 h before enrolment. We excluded patients who:
Were suspected of having a high risk of death within 48 h after randomization, this depends on the judgement of the attending physicians, which is mostly based on the patient’s hemodynamic parameters during the screening process.
Had ARDS as defined by the Berlin criteria 14 before randomization
Were suspected of needing invasive mechanical ventilation for <48 h. This criterion is specific for patients who require endotracheal intubation for airway protection during an invasive procedure.
Had a tracheostomy tube
Were pregnant or actively lactating
Had a do-not-resuscitate decision
Had extracorporeal membrane oxygenation support before randomization
After obtaining informed consent, we recorded the patients’ baseline characteristics, baseline mechanical ventilator settings and lung mechanical parameters. Based on the underlying pathophysiology, we classified acute respiratory failure requiring intubation into four categories. The categories were type 1, acute hypoxic respiratory failure; type 2, acute hypercapnic respiratory failure; type 3, acute respiratory failure caused by perioperative atelectasis; and type 4, acute respiratory failure during shock or hypoperfusion.15,16
The acute lung injury (ALI) score was calculated to assess the severity of lung injury. The computation was based on a patient’s oxygenation status, chest X-ray results, positive end-expiratory pressure (PEEP) level and respiratory compliance measurements. Each component was assigned a score ranging from 0 (no injury) to 4 (the most severe injury), and their average was subsequently used as the ALI score 17 (Supplemental Table 1). To calculate the baseline score, we used the worst information for each component during the 24 h before enrolment.
Randomization
Patients providing informed consent were enrolled in the study and allocated randomly to the LDP or LTV ventilation strategy group. Randomization was achieved using a computer-generated table sourced from www.randomization.com. The process adopted a 1:1 ratio, employing blocks of four opaque, pre-numbered, sealed envelopes. These envelopes were dispatched to the participating ICUs, with the ICU allocations based on the computer-generated random number table. The randomization process was overseen by an investigator (S.T.) who was excluded from patient enrolment and management. Although other investigators, the patients and their families remained blinded to the study allocation, the attending clinicians and nursing staff were cognizant of each patient’s assignment to the LDP or LTV ventilation group.
Study intervention
Post-randomization, patients in the LDP group underwent ventilation targeted at a driving pressure of ⩽15 cmH2O. When patients were ventilated in pressure-controlled ventilation (PCV) mode, the driving pressure corresponded to the applied inspiratory pressure. When volume-controlled ventilation (VCV) was utilized, an inspiratory hold lasting between 0.5 and 1 s was instigated until the inspiratory pressure plateaued. The difference between the plateau inspiratory pressure and the PEEP equated to the measured driving pressure. Ventilator settings were modulated to maintain the driving pressure at 15 cmH2O or below. The inspiratory pressure was gradually decreased by 1 cmH2O (PCV mode), or the tidal volume was reduced by 50 mL (VCV mode) at 15- to 30-min intervals. Adjustments to respiratory rate, PEEP and the fraction of inspired oxygen (FiO2) were permitted to sustain an oxygen saturation level ⩾94% and a pH between 7.35 and 7.45 during mechanical ventilation.
For patients in the LTV group, ventilation targeted a tidal volume of ⩽8 mL/kg of predicted body weight (PBW). To compute the PBW, the following equations were employed: 50 + 0.91 × [height (cm) − 152.4] for men and 45.5 + 0.91 × [height (cm) − 152.4] for women. 2 The ventilator settings were periodically adjusted by dropping the inspiratory pressure by 1 cmH2O (PCV) or by reducing the tidal volume by 50 mL (VCV) every 15–30 min. The goal was to consistently maintain the tidal volume at ⩽8 mL/kg. As with the LDP group, the respiratory rate, PEEP and FiO2 were flexible, allowing maintenance of oxygen saturation at ⩾94% and pH within the range of 7.35–7.45.
In both cohorts, sedatives, analgesic agents or muscle relaxants were used to counteract patient-ventilator asynchrony at the attending physician’s discretion. All patients received standard care for acute respiratory failure and treatments tailored to their individual ICU admission diagnoses for acute critical illnesses.
Outcome assessments
The primary outcome of this study was the ALI score on day 7. The score was derived from the most severe measurements of each patient’s oxygenation, chest X-ray results, PEEP level and respiratory compliance on day 7. For patients who died before day 7, an ALI score of 4 was assigned. The secondary outcomes were 28-day mortality and the onset of ARDS within 28 days post-enrolment. The Berlin criteria were employed for ARDS diagnoses. We also recorded rates of new-onset pneumothorax, ventilator-associated pneumonia, lung atelectasis and hypoventilation. The calculation of mechanical ventilator support-free days up to day 28 followed the formula suggested by Russell et al. 18 The on-duty radiologist conducted the chest X-ray interpretation, which included the extent of abnormal pulmonary infiltration as part of the ALI score calculation and the detection of pneumothorax and atelectasis. The radiologist was blinded to patient enrolment and group assignments.
Statistical analyses
We postulated that a difference of 1.5 points in the ALI scores on day 7 could influence patient outcomes. Enrolling at least 63 participants per group would afford an 80% power to discern a 1.5-point difference in the ALI score on day 7 between groups, with a two-sided alpha error of 0.05.
Continuous variables underwent normality testing using the Kolmogorov–Smirnov test. Normally distributed variables are presented as the means [standard deviation (SD)] and were assessed using a t-test. Variables deviating from a normal distribution are shown as medians and interquartile ranges (IQRs) and were analysed using the Wilcoxon rank-sum test. Categorical variables are depicted by frequency and percentage. Depending on suitability, the chi-square test or Fisher’s exact test was employed. The primary outcome was subjected to a t-test. Secondary outcomes were evaluated with the chi-square test and are presented as relative risk (RR) with a 95% confidence interval (CI). Kaplan–Meier curves were used to appraise mortality outcome days, followed by a log-rank test comparison at 28 days. For mortality assessment, the 28-day mortality was computed from the enrolment date. All primary and secondary outcome analyses adhered to the intention-to-treat principle, and p values <0.05 denoted statistical significance. Data analyses were executed using PASW Statistics, version 18 (SPSS Inc, Chicago, IL, USA). The study was registered with the ClinicalTrials.gov database (identification number NCT04035915).
Results
We screened a total of 230 patients requiring invasive mechanical ventilator support. Of these, 126 met the inclusion criteria and were randomized to the LDP or LTV treatment group. Every randomized patient was monitored until the study’s conclusion and included in the final intention-to-treat analysis (Figure 1). Patients’ baseline characteristics – age, sex, PBW, underlying conditions and disease severity – were comparable between the two groups (Table 1). The primary reason for intubation was hypoxemic respiratory failure: LDP 49.2% (31/63), LTV 63.5% (40/63), p = 0.11. Sepsis or septic shock was the predominant ICU admission diagnosis for both groups: 87.3% (55/63) in each group (p = 1.00). Pneumonia was the leading infection cause: LDP 44.4% (28/63), LTV 47.6% (30/63), p = 0.72. The median duration from intubation to enrolment was 8 h 30 min (4:00–12:00) for the LDP group and 7 h 30 min (3:25–10:45) for the LTV group. The mean (SD) baseline ALI scores were 1.83 (0.68) for the LDP group and 1.75 (0.72) for the LTV group, with p = 0.51 (Table 1). The distribution of baseline ALI scores and the association of baseline ALI scores and hospital mortality is shown in Supplemental Table 2.
Baseline characteristics of the patients.
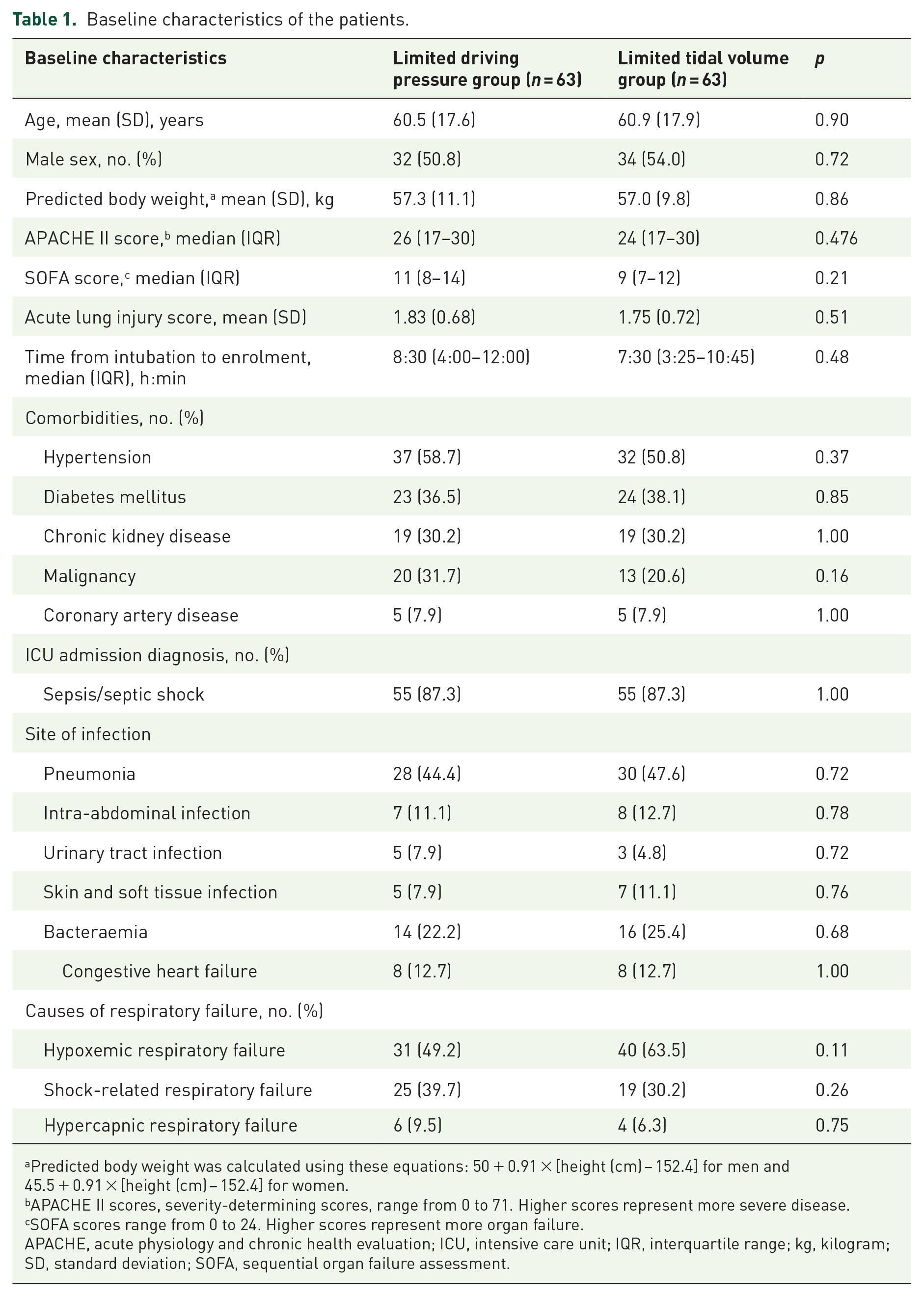
Predicted body weight was calculated using these equations: 50 + 0.91 × [height (cm) − 152.4] for men and 45.5 + 0.91 × [height (cm) − 152.4] for women.
APACHE II scores, severity-determining scores, range from 0 to 71. Higher scores represent more severe disease.
SOFA scores range from 0 to 24. Higher scores represent more organ failure.
APACHE, acute physiology and chronic health evaluation; ICU, intensive care unit; IQR, interquartile range; kg, kilogram; SD, standard deviation; SOFA, sequential organ failure assessment.
Upon enrolment, most patients in both groups were under PCV mode: LDP 93.7% (59/63), LTV 88.9% (56/63), p = 0.53. As shown in Table 2, the baseline respiratory parameters of the LDP and LTV groups were comparable. Specifically, there were no significant differences in tidal volume per PBW [mean (SD) 8.6 (2.1) versus 8.3 (2.3) mL/kg, p = 0.45], driving pressure [mean (SD) 17.2 (4.1) versus 17.9 (4.2) cmH2O, p = 0.31] or peak inspiratory pressure [median (IQR) 23 (20–26) versus 24 (20–26) cmH2O, p = 0.47]. Baseline arterial blood gas analyses for arterial blood pH, partial pressure of oxygen in arterial blood (PaO2), oxygen saturation, partial pressure of carbon dioxide in arterial blood (PaCO2) and the PaO2:FiO2 ratio were consistent across both groups (Table 2). An analogous number of patients in each group were administered vasopressors, inotropes, sedatives and paralytic agents. Renal replacement therapy was needed for 38.1% (24/63) of the LDP group and 25.4% (16/63) of the LTV group (p = 0.13, Table 2).
Baseline respiratory parameters of the patients at the time of enrolment and other treatments.

Proportion of patients who had tidal volume per predicted body weight <8 mL/kg during 7 days (study period) after enrolment.
Duration of tidal volume per predicted body weight over 8 mL/kg is calculated by the duration (h) that the patient had tidal volume per predicted body weight over 8 mL/kg divided by 168 h.
Proportion of patients who had driving pressure <15 cmH2O during 7 days (study period) after enrolment.
Duration of driving pressure over 15 cmH2O is calculated by the duration (h) that the patient had driving pressure over 15 cmH2O divided by 168 h.
cmH2O, centimetres of water; FiO2, fraction of inspired oxygen; HCO3, bicarbonate; IQR, interquartile range; mL/kg, millilitres per kilogram; PaCO2, partial pressure of carbon dioxide in arterial blood; PaO2, partial pressure of oxygen in arterial blood; SD, standard deviation.
After randomization, patients in the LDP group exhibited a higher tidal volume per PBW than those in the LTV group, although the difference was not statistically significant [Figure 2(a)]. There was no difference in driving pressure between the LDP and LTV groups [Figure 2(b)]. There were 19 (30.2%) patients in LDP and 33 (52.4%) patients in LTV who had tidal volume per PBW lower than 8 mL/kg at all times after study enrolment (p = 0.01). The percentage of timing that patients had tidal volume per PBW higher than 8 mL/kg within 7 days after enrolment was significantly higher among LDV than LTV group (7.14 + 7.30 versus 4.05 + 5.88, p = 0.01). The proportion of patients who had driving pressure lower than 15 cmH2O [21 (33.3%) versus 19 (30.2%), p = 0.70] and the percentage of timing that patients had driving pressure higher than 15 cmH2O (6.67 + 6.87 versus 7.57 + 7.10, p = 0.47) were not different between groups (Table 2).

Comparison of the tidal volumes (a), driving pressures (b) and acute lung injury scores (c) of the limited driving pressure and low tidal volume groups.
The primary outcome, the ALI score on day 7, showed no significant difference between the LDP and LTV groups [mean (SD) 1.90 (1.14) versus 1.89 (0.99), p = 0.95]. The result remained no significant different after a sensitivity analysis, excluding 15 patients who died before day 7, was performed [1.51 (0.74) versus 1.71 (0.80), p = 0.17]. An increase in the ALI score was observed in 38.1% (24/63) of LDP patients and 34.9% (22/63) of LTV patients (p = 0.71). Figure 2(c) illustrates the progression of the ALI score for both groups. The rate of successful extubation at 14 days was comparable between the groups: LDP 39.7% (25/63), LTV 41.3% (26/63), p = 0.86. New-onset ARDS appeared in 14.3% (9/63) of the LDP group compared to 20.6% (13/63) in the LTV group (RR 0.81, 95% CI 0.55–1.22, p = 0.35). Other adverse events linked with mechanical ventilator support, such as pneumothorax, ventilator-associated pneumonia, atelectasis and carbon dioxide (CO2) retention, showed no significant differences between the groups (Table 3).
Primary and secondary outcomes.

ARDS, acute respiratory distress syndrome; CI, confidence interval; CO2, carbon dioxide; ICU, intensive care unit; IQR, interquartile range; SD, standard deviation.
The 28-day mortality rate was 34.9% (22/63) for the LDP group and 31.7% (20/63) for the LTV group (RR 1.08, 95% CI 0.74–1.57, p = 0.71, Table 3). The Kaplan–Meier curves for 28-day mortality are depicted in Figure 3. The ICU mortality rates showed no significant difference: LDP 36.5% (23/63), LTV 38.1% (24/63), RR 0.97, 95% CI 0.68–1.38, p = 0.85. In-hospital mortality rates were also consistent: LDP 50.8% (32/63), LTV 52.4% (33/63), RR 0.97, 95% CI 0.68–1.37, p = 0.86, Table 3. The mean (SD) number of days alive and free from mechanical ventilation up to day 28 showed no difference: LDP 8.71 (10.44) days, LTV 10.22 (11.21) days, p = 0.44, Table 3. A subgroup analysis for hypoxemic respiratory failure was performed. The results of the subgroup analysis are shown in Supplemental Table 3. There was no significant difference in primary and secondary outcomes among hypoxemic respiratory failure patients in the LDP and the LTV groups.
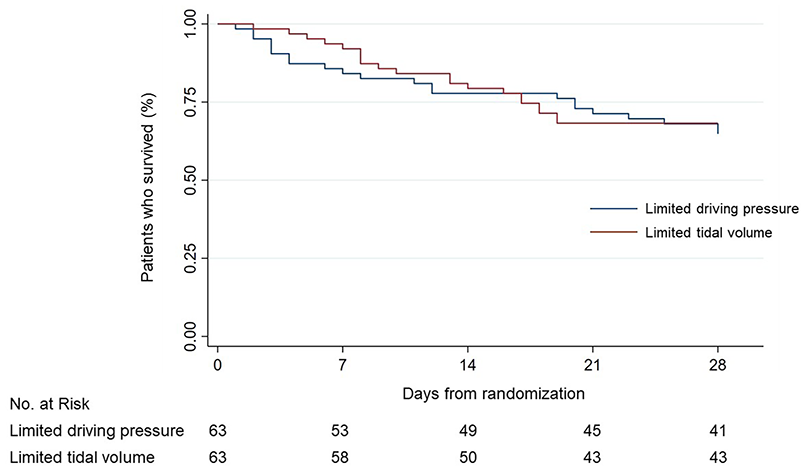
Kaplan–Meier analysis of 28-day mortality. There was no difference between the limited driving pressure and low tidal volume groups (log-rank p = 0.71).
Discussion
Our randomized controlled trial studied adult patients with acute respiratory failure who lacked ARDS and required mechanical ventilation support. We found no significant difference in the lung injury scores of the LDP and LTV strategy groups on day 7. Similarly, the rates of pulmonary complications – new-onset ARDS, pneumothorax, ventilator-associated pneumonia and atelectasis – exhibited no significant variations between the groups. The 28-day and in-hospital mortality rates also showed no notable variance between the two groups.
This study used a driving pressure threshold of ⩽15 cmH2O for the LDP group and a tidal volume threshold of ⩽8 mL/kg for the LTV group. These values were selected because they aligned with previous research findings.9,10,19 Past observations have shown that a driving pressure increase exceeding 15 cmH2O is linked to higher hospital mortality among ARDS patients. The earlier studies also found that non-ARDS patients ventilated with an LTV strategy (6–8 mL/kg) had similar outcomes to those using an intermediate tidal volume strategy (8–10 mL/kg). Specifically, there was no significant difference in the number of days they were alive without mechanical ventilation at 28 days.9,10,19
Our results support the proposition of targeting lower driving pressure to prevent VILI10,18 and suggest that it is an alternative to the lower tidal volume strategy. Considering the heightened heterogeneity of lung parenchyma pathology in non-ARDS patients relative to ARDS patients, 20 constraining the driving pressure could mitigate the mechanical stress on preserved lung parenchyma. Reducing this stress is particularly important as the inconsistency in lung expansion in non-ARDS patients results in regional strains. The strains are notably more severe than the overall strains seen in the healthy and inflamed lungs of such patients. By adopting a lower driving pressure, we can preclude overdistension of preserved alveoli, thereby reducing the risk of VILI. Conversely, while the LTV strategy relies predominantly on PBW-based calculations, the LDP approach offers a more physiologically congruent method to guard against VILI.
Another potential advantage of the LDP over the LTV strategy is its allowance for variations and potentially higher tidal volumes. This attribute is particularly beneficial in response to an escalating respiratory drive, especially in patients with metabolic acidosis or shock-related respiratory failure. When patients are ventilated using an LTV strategy, their inability to augment tidal volume might lead to an amplified respiratory drive, which, in turn, can potentially result in patients’ self-inflicted lung injury. 21 To mitigate this, sedative and analgesic agents or muscle relaxants might be employed.22,23 However, while these drugs can enhance patient–ventilator synchrony, their overuse can lead to delirium, protracted dependency on mechanical ventilation, weaning difficulties and extubation failure.24–26 Our findings revealed a marginally elevated use of the sedative and analgesic agent fentanyl in the LTV group compared with the LDP group, although the difference was nonsignificant. Crucially, this variance in medication administration did not significantly influence the extubation rate at 14 days or the number of days alive without mechanical ventilation up to day 28. Additionally, no significant differences were noted in the use of muscle relaxants by the two groups.
Our study has several noteworthy strengths. Firstly, it is a prospective randomized controlled trial, which is considered a robust design for evaluating interventions. Moreover, a blinded investigator conducted the outcome evaluations, lending greater objectivity to the results. Another merit is the adoption of the ALI score as the primary outcome. This metric integrates four clinical parameters that are ubiquitously employed globally in clinical practice. The use of the ALI score is therefore feasible even in resource-constrained settings, as it draws on easily accessible clinical data. Although introduced several decades ago, the sustained employment of the ALI score in acute respiratory failure, ARDS and emergent conditions such as COVID-19 attests to its worth in severity evaluation and prognostic predictions.27,28 This continued use accentuates the utility and pertinence of the ALI score for both non-ARDS and ARDS patients with acute respiratory failure.
Several limitations of this study merit attention. Firstly, we could not blind attending physicians and nurses to the intervention, introducing potential study bias. To address this, we designated an investigator who was blinded to the intervention allocations to evaluate patient outcomes. Secondly, our decision to use an ALI difference of 1.5 on day 7 for sample size calculation may have resulted in the study being underpowered to detect more subtle differences with the given study population size. In a multicenter trial with larger population size, control of the rate is certainly required to assess the potential benefit of low driving pressure in the prevention of VILI. Thirdly, as the investigation focused on non-ARDS patients with good respiratory compliance, its findings might not directly apply to patients with poor respiratory compliance. Finally, we employed the inspiratory pressure of patients on PCV as a surrogate for driving pressure. This approach might have underestimated the driving pressure, especially in patients exerting high inspiratory efforts. Notwithstanding this potential shortcoming, using inspiratory pressure to titrate the driving pressure remains a practicable method in bedside clinical practice.
Conclusion
In adults with acute respiratory failure but without ARDS, there was no difference in the efficacy of LDP and LTV in averting lung injuries 7 days after mechanical ventilation. Specifically, no variation was observed in the prevention of injuries when comparing an LDP of ⩽15 cmH2O to an LTV of <8 mL/kg of PBW.
Supplemental Material
sj-doc-4-tar-10.1177_17534666241249152 – Supplemental material for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial
Supplemental material, sj-doc-4-tar-10.1177_17534666241249152 for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial by Surat Tongyoo, Tanuwong Viarasilpa, Phitphiboon Deawtrakulchai, Santi Subpinyo, Chaiyawat Suppasilp and Chairat Permpikul in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-1-tar-10.1177_17534666241249152 – Supplemental material for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial
Supplemental material, sj-docx-1-tar-10.1177_17534666241249152 for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial by Surat Tongyoo, Tanuwong Viarasilpa, Phitphiboon Deawtrakulchai, Santi Subpinyo, Chaiyawat Suppasilp and Chairat Permpikul in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666241249152 – Supplemental material for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial
Supplemental material, sj-docx-2-tar-10.1177_17534666241249152 for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial by Surat Tongyoo, Tanuwong Viarasilpa, Phitphiboon Deawtrakulchai, Santi Subpinyo, Chaiyawat Suppasilp and Chairat Permpikul in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-3-tar-10.1177_17534666241249152 – Supplemental material for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial
Supplemental material, sj-docx-3-tar-10.1177_17534666241249152 for Comparison of limited driving pressure ventilation and low tidal volume strategies in adults with acute respiratory failure on mechanical ventilation: a randomized controlled trial by Surat Tongyoo, Tanuwong Viarasilpa, Phitphiboon Deawtrakulchai, Santi Subpinyo, Chaiyawat Suppasilp and Chairat Permpikul in Therapeutic Advances in Respiratory Disease
Footnotes
Appendix
Acknowledgements
Our gratitude goes to Mr. David Park for linguistic editing. This research was conducted at the Division of Critical Care Medicine, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.