
Abstract
Nanoparticles have attracted extensive attention due to their high degree of cell targeting, biocompatibility, controllable biological activity, and outstanding pharmacokinetics. Changing the size, morphology, and surface chemical groups of nanoparticles can increase the biological distribution of agents to achieve precise tissue targeting and optimize therapeutic effects. Examples of their use include nanoparticles designed for increasing antigen-specific immune responses, developing vaccines, and treating inflammatory diseases. Nanoparticles show the potential to become a new generation of therapeutic agents for regulating inflammation. Recently, many nanomaterials with targeted properties have been developed to treat acute lung injury/acute respiratory distress syndrome (ALI/ARDS). In this review, we provide a brief explanation of the pathological mechanism underlying ALI/ARDS and a systematic overview of the latest technology and research progress in nanomedicine treatments of ALI, including improved nanocarriers, nanozymes, and nanovaccines for the targeted treatment of lung injury. Ultimately, these nanomedicines will be used for the clinical treatment of ALI/ARDS.
Introduction
Acute respiratory distress syndrome (ARDS) is the most advanced form of acute lung injury (ALI), and it is caused by harmful extrapulmonary factors and pathogenic factors. 1 The mortality rate of patients with ALI/ARDS has decreased over the past decade, but it remains as high as 30–40%; moreover, ALI/ARDS is an important cause of death in critically ill patients. The pathological features of ALI/ARDS are diffuse alveolar damage, which involves the destruction of type I alveolar epithelial cells and pulmonary vascular endothelial cells; pulmonary interstitial fibrosis; and type II epithelial cell proliferation, which results in pulmonary edema and inflammatory cell infiltration in lung tissues. 2 Some patients eventually develop ARDS, which causes irreversible acute respiratory failure and multiple organ dysfunction. As medical interventions have improved, novel drugs and therapies for ALI/ARDS have gradually been developed; however, the case fatality rate of ALI/ARDS has not significantly decreased, and treatment of ALI/ARDS remains difficult. Therefore, searching for safer and more effective therapies has been the focus of recent research. The pathogenesis of ALI/ARDS is complex, and to date, it has not been fully elucidated. Currently, it is thought that ALI/ARDS represents an extensive and excessive inflammatory response in lung tissues after severe infection, trauma, shock, massive blood transfusion, infusion, etc.3,4 Therefore, the inflammatory response plays an important role in the occurrence and development of ALI/ARDS. The pathophysiological mechanism underlying ALI/ARDS consists mainly of inflammatory cell migration, fiber proliferation, and apoptosis. Inflammatory cells and inflammatory mediators constitute the ‘cell network’ and ‘cytokine network’ of the inflammatory response and regulate the immune response in ALI/ARDS. These networks regulate the inflammatory response through different signal transduction pathways. 5 Therefore, overactivation or imbalance of the inflammatory response is a primary cause of ALI/ARDS.
Nanoparticles are very small particles with diameters ranging from 1 to 100 nm. Because of their unique physical and chemical properties, nanoparticles are widely used in the fields of engineering and medicine as well as other scientific fields. Nanoparticles have attracted substantial attention due to their strong ability to target cells, excellent biocompatibility, controllable biological activity, and outstanding pharmacokinetics.6,7 Changing the size, morphology, and surface chemical groups of nanoparticles can increase the biological distribution of these agents to precisely target tissues and optimize therapeutic effects. Nanoparticles are thus powerful tools for the treatment of human immune-related diseases. Nanoparticles have been designed for applications including increasing antigen-specific immune responses, developing vaccines, and treating inflammatory diseases. Moreover, studies have shown that nanoparticles can target phagocytes. 8 Therefore, nanoparticles have the potential to become a new generation of therapeutic agents for regulating inflammation. Recently, many nanomaterials with targeted properties have been developed to treat ALI/ARDS. The emergence of nanomedicine has led to new strategies for overcoming limitations in the field of traditional drug therapy, but challenges remain, limiting the likelihood of the clinical translation of these agents. In particular, toxicity and safety are the major challenges facing the clinical translation of nanomedicines.
In this review, we provide a brief explanation of the pathological mechanism underlying ALI/ARDS, and a systematic overview of the latest technology and research progress in the treatment of ALI with nanomedicine, including improved nanocarriers, nanozymes, and nanovaccines for the targeted treatment of lung injury. Ultimately, these nanomedicines will be used for the clinical treatment of ALI/ARDS.
Pathological mechanism underlying ALI/ARDS
ALI is a common clinical syndrome in critically ill patients, and its severe form is called ARDS. 1 The pathophysiological features of this condition are alveolar epithelial cell and pulmonary microvascular endothelial cell injury and increased permeability of the alveolar membrane, resulting in diffuse pulmonary interstitial and alveolar edema. 2 Moreover, decreased levels of active alveolar surface substances and dystonia of the alveolar surface ultimately lead to decreased lung compliance and severe ventilation/blood flow imbalance. The clinical manifestations of this condition are progressive hypoxemia and respiratory distress, and the radiological manifestations of ALI are heterogeneous exudative lesions, which can develop into severe disease and lead to ARDS.
Many factors cause ALI/ARDS, including factors that act either directly or indirectly; among these factors, the most common factor that acts directly is infection, such as bacterial or viral infection. In addition, stomach content inhalation and lung contusions cause ALI/ARDS. The most common factor that acts indirectly is sepsis, which is a consequence of severe trauma, massive transfusion or infusion, acute severe pancreatitis, etc. The pathogenesis of ALI is complex, and the pathological process mainly includes the following three stages. 9 During the acute exudation stage, pulmonary vascular endothelial cells and type I alveolar epithelial cells are damaged; a large number of inflammatory cells, such as neutrophils, disseminate and infiltrate lung tissues; and the excessive release of inflammatory factors in the lungs leads to an imbalance in the proinflammatory/anti-inflammatory system and the oxidation/antioxidant system, triggering an inflammatory ‘waterfall-like’ cascade reaction and ultimately exacerbating the initial lung injury. With increased microvascular permeability, alveolar edema occurs and causes disordered lung function. During lung tissue remodeling, chronic inflammation develops, and the inflammatory cascade plays a key role in disease-related cell apoptosis, proliferation, and migration.10,11 Extracellular matrix deposition occurs in alveoli, type II alveolar epithelial cells undergo significant proliferation, and squamous metaplasia may also develop during this stage. In the fibrosis stage, a continuous inflammatory response and hyperplasia lead to the degeneration of dense collagen in the alveoli and hyalinotic changes in the alveolar wall. The deposition of cellulose in alveoli leads to pulmonary tissue fibrosis and irreversible damage to respiratory function. Due to excessive inflammatory responses and oxidative stress, the vascular endothelium, and alveolar epithelial cells are damaged, which disrupts their barrier function and leads to respiratory failure in patients with impaired gas exchange capacity.
One of the critical mechanisms underlying the development of ARDS involves an imbalance in the inflammatory response, which exacerbates alveolar epithelial and endothelial cell damage and leads to increased alveolar-capillary permeability, then fibrosis, and ultimately ARDS. 12 During ALI/ARDS, the inflammatory response can be initiated by exogenous and endogenous stimuli. Exogenous stimuli, such as bacterial antigens, initiate inflammatory responses by activating Toll-like receptors (TLRs) and intracellular kinases, leading to cell membrane rupture and oxidative stress. 13 Endogenous stimuli primarily include damage-associated molecular pattern molecules that are released by dead cells or local inflammatory cells, and these molecules activate and recruit immune cells by binding to different receptors, such as TLRs or interleukin-1 receptor (IL-1R), thereby activating proinflammatory pathways.
The main inflammatory cells that are involved in ARDS are neutrophils and lung macrophages. Neutrophils, which are important inflammatory cells, release a large number of inflammatory factors and produce reactive oxygen species (ROS), which directly damage lung tissue. 14 During the initial (acute) phase of inflammation, neutrophils respond to the migration of inflammatory cells to the site of inflammation, activating these inflammatory cells, initiating inflammatory cascades, and contributing to uncontrolled inflammation in the lung. Alveolar endothelial cells are damaged by proinflammatory factors that are released by neutrophils as well as by ROS, and this damage results in pathological symptoms. Alveolar endothelial cells synthesize and release vasoactive substances and inflammatory mediators, which participate in vascular permeability, coagulation, and systemic inflammatory responses and thus play important roles in ALI/ARDS. The development of ALI/ARDS leads to the release of a variety of proinflammatory factors, including cytokines and lipid products, and the release of these factors is accompanied by the production of procoagulant factors and the activation of neutrophils, platelets, and monocytes, all of which disrupt the endothelial barrier and lead to deregulated tissue perfusion and oxygenation. In addition, alveolar macrophages can produce proinflammatory factors. Alveolar macrophages account for approximately 90% of all macrophages in the lung, they are activated at the beginning of inflammatory responses in the lungs, and they are sources of inflammatory mediators and cytokines. 15 During the initial inflammatory phase, alveolar macrophages are activated and release neutrophil-activating factors, such as tumor necrosis factor α (TNF-α), interleukin-1β (IL-1β), and IL-8. These early inflammatory factors activate neutrophils, which, in turn, activate more macrophages in the alveoli; thus, a series of inflammatory responses is initiated.
However, studies have shown that neutrophils play both proinflammatory and anti-inflammatory roles in ALI/ARDS. The main mechanism may be related to the production of chemokines by macrophages. The balance between the concentration of chemokines produced by local macrophages and the concentration of chemokines produced at distant inflammatory sites affects the direction of neutrophil migration in the lung. In response to this concentration gradient, neutrophils cross the endothelium and are recruited to infected or inflammatory sites where they release many proteolytic enzymes and ROS as well as stimulate the release of the anti-inflammatory factor IL-10 by macrophages.
Despite the severity of ARDS, there is no effective treatment. Inhaled nitric oxide, glucocorticoids, and β-agonists have been used to treat ARDS. However, these agents either only temporarily alleviate symptoms without reducing mortality rates or cause adverse effects on other organs. Therefore, effective targeted drugs with low toxicity need to be developed for the treatment of ALI/ARDS.
Application of nanoparticles in the treatment of ALI
Nanoparticles have attracted substantial attention due to their ability to effectively target therapeutic agents to particular sites, excellent biocompatibility, controllable biological activity, and outstanding pharmacokinetics. 16 Changing the size, morphology, and surface chemical groups of nanoparticles can allow better biological distribution of agents in vivo, and thus, tissue targeting and optimized therapeutic effects can be achieved.17,18 To date, many nanoparticles with different surface chemical properties have been used in clinical treatment. More than 50 nanodrugs have been approved by the FDA for therapeutic or imaging purposes, and nearly 100 nanodrugs are being evaluated in clinical trials.19,20 Previous studies have shown that nanoparticles are powerful tools for the treatment of human immune-related diseases.21,22 For example, nanoparticles are used to increase antigen-specific immune responses, to develop vaccines, and to treat inflammatory diseases. In addition, nanoparticles have been shown to target phagocytes; therefore, they are considered to be a new generation of therapeutic agents that can potentially be used to treat inflammatory diseases, such as ALI. To date, many nanoparticles have been developed to treat ALI. 23 For example, porous Se@SiO2 nanoparticles (NPs) have antioxidant properties, very low cytotoxicity, and good biocompatibility. Se@SiO2 significantly reversed the effect of LPS on inhibiting the expression of nuclear factor erythroid 2-related factor 2 (NRF2) and the downstream target NAD(P)H quinone dehydrogenase 1 (NQO1) as well as significantly increased the antioxidant capacity of an airway epithelial cell line (Beas-2B cells). Moreover, Se@SiO2 NPs upregulated the expression of zonula occludens-1 (ZO-1) and E-cadherin (E-Ca), indicating that enhanced antioxidant activity and tight junctions after Se@SiO2 treatment protected airway epithelial cells against LPS-induced damage. 24 Su et al. prepared dexamethasone (Dex)/mannose comodified branched polyethyleneimine (PEI) prodrug nanoparticles (DPMs), which effectively targeted the mannose receptor on alveolar macrophages, for the treatment of ALI. The DPM prodrug NPs showed good stability in serum and biocompatibility, and they have a certain sensitivity to acidic microenvironments. In LPS-induced ALI mouse models, DPM prodrug NPs effectively targeted inflammatory tissue and significantly reduced inflammatory cell infiltration and TNF-α secretion, thereby effectively ameliorating ALI. 25
The emergence of nanomedicine will lead to new approaches for addressing the current limitations in the field of traditional drug therapy, but challenges to the clinical translation of nanomedicines remain. Toxicity and safety are the most important problems that need to be resolved for the clinical translation of nanomedicine. Additional novel nanoparticles for use in the targeted treatment of lung injury are urgently needed; examples of such nanoparticles include improved nanocarriers, nanozymes, and nanovaccines, which will become novel nanomedicines for the clinical treatment of ALI.
Novel nanocarriers for the treatment of ALI
Liposome-based nanoparticles
Liposomes are artificial membrane-bound vesicles. In water, the hydrophilic heads of phospholipid molecules interface with water molecules, and the hydrophobic tails of liposomes extend into the air. After agitation, spherical liposomes with a double lipid membrane form. Liposomes are among the most well-studied and relatively mature nanocarriers due to their advantages of high selectivity, low toxicity, lack of immunogenicity, and easy degradation in vivo. Liposomes can be used to control drug release at appropriate target sites, effectively maintain drug stability, prevent rapid drug degradation, significantly increase drug therapeutic indices, and reduce the number of adverse reactions. However, there are some problems associated with the use of liposome carrier systems. For example, liposomes that enter systemic circulation are easily phagocytosed by mononuclear macrophages; therefore, liposomes accumulate in tissues that are enriched with endothelial cells. To date, this accumulation is mainly prevented via PEGylation. Embedding cilomilast into PEGylated phosphatidylcholine-rich niosomes (phosphatiosomes) significantly increases drug delivery to the lungs. Moreover, phosphatiosomes significantly reduced alveolar hemorrhage, neutrophil infiltration, and lung parenchyma injury in mice with ALI. 26 However, PEGylated nanocapsules cannot be chemically modified, and they can produce factors that induce toxic degradation and elicit specific anti-PEG antibody production under oxidative conditions; these characteristics limit the application of liposome nanocapsules. In addition, when nanomaterials enter blood circulation, a layer of plasma proteins is passively adsorbed onto their surface, forming a protein corona. The formation of a protein corona can inhibit tissue targeting mediated by ligands on the nanomaterial surface and can lead to the degradation of intentionally added surface modifications, limiting the specific binding of nanomaterials to endogenous cells.
Li et al. developed liposomes composed of inverse-phosphocholine (CP) lipids (n-DOCPs) that effectively target activated neutrophils in vivo through a specific interaction between the cell-bound complement receptor CR3 and the adsorbed complement fragment iC3b. These authors found that the n-DOCPs triggered a ‘voluntary opsonization’ process in blood, resulting in the formation of a protein corona that was enriched with the complement fragment iC3b. The iC3b fragment specifically recognizes and binds to the complement receptor CR3 on neutrophil surfaces to induce neutrophil phagocytosis. In addition, activated neutrophils express high levels of CR3, thereby increasing the targeting specificity of n-DOCPs. This ‘voluntary opsonization’ process enables excellent targeting and mobility of these nanoparticles when stimulated by inflammatory factors. Activated neutrophils can carry n-DOCPs through physiological barriers to increase the specificity of nanodrug delivery, allowing the drug to exert its effect at the lesion site. Under inflammatory conditions, neutrophils can act as microvessels or release n-DOCPs to kill bacteria, leading to significant therapeutic effects. After the intravenous administration of dexamethasone encapsulated by n-DOCPs, the levels of the inflammatory cytokines TNF-α and IL-6 in bronchoalveolar lavage fluid (BALF) and serum were significantly reduced, and the number of infiltrating neutrophils in inflamed lungs was decreased; these effects resulted in the effective alleviation of ALI in mice with LPS-induced pneumonia. In addition, in a mouse model of pneumonia that was induced by clinically isolated Streptococcus pneumoniae (S. pneumoniae), the injection of ampicillin-encapsulated n-DOCPs effectively suppressed bacterial proliferation, inhibited pneumonia development, and prolonged the survival of mice with bacterial pneumonia. These results show that n-DOCPs can be used as novel nanocarriers to target circulating cells via the protein corona that spontaneously formed during nanodrug administration; thus, these particles can enhance drug delivery and have wide application prospects for the treatment of inflammatory diseases 27 (Figure 1 and Table 1).

Lipid nanoparticles based on the formation of protein corona for treatment of acute lung injury. (a) n-DOCPs targeted activated neutrophils in inflammatory mice. (b) Neutrophils-mediated delivery of drug-loaded n-DOCPs mitigated acute lung injury and pneumococcal pneumonia.
The therapy application of nanomedicine in ARDS.

ACM, apoptotic cell membrane; ALI, acute lung injury; DMON, dendritic mesoporous silicon nanoparticles; GNPs, gold nanoparticles; MOFs, metal-organic frameworks; MSN, mesoporous silica nanoparticles; PBA, phenylboronic acid.
Novel polymeric nanoparticles
The use of polymer nanoparticles as carriers for pulmonary drug delivery has attracted substantial attention. Polymer nanomaterials are designed from natural or synthetic polymers, most of which are biodegradable and biocompatible. Commonly used polymer materials include natural products (chitosan, alginate, and cyclodextrin) and synthetic products [polyethylene glycol (PEG), polylactic acid-co-glycolic acid (PLGA), polyacrylate, and PEI]. Among these materials, PLGA has been approved by the FDA for clinical use due to its high biocompatibility. PLGA is often used to prepare NPs for pulmonary drug delivery.44,45 However, before PLGA polymer nanoparticles can be applied in vivo, many challenges must be overcome. The solubility of PLGA in water is relatively poor, large nanoparticles are formed, and these nanocarriers are easily cleared by the liver and spleen, reducing the concentration of drugs in damaged tissues. In addition, the low drug-loading capacity of PLGA NPs has limited their application.
Dendrimers are macromolecules that exhibit regular branching. Recently, novel dendrimer–drug conjugates and dendrimer gene carriers have been developed. The outer layer of dendrimers can be polymerized to establish higher-order dendrimer structures, and the outer layer of dendrimers can be engrafted with a large number of functional groups to enhance their functionality. Based on their clear structural advantages, dendrimers can be used as nanocarriers to deliver different types of drugs, and they exhibit a combination of various characteristics that render them useful as a therapeutic strategy for efficient and precise treatment; thus, dendrimers play an important role in drug delivery.
Poly(amidoamine) (PAMAM) dendrimers
PAMAM dendrimers are polymers with special structures that have increasingly attracted attention. PAMAM dendrimers are perfectly formed monodisperse polymers with an organized and highly branched three-dimensional structure, and these structures are easy to modify to change their solubility because they not only form an internal cavity but also have a large number of functional groups on their surface. Therefore, PAMAM dendrimers have the potential to be used as drug delivery systems in biomedicine and other fields. In many studies, PAMAM dendrimers have been shown to mediate effective cell uptake and siRNA transfection in vitro for the treatment of acute pulmonary inflammation. For example, Bohr et al. used a third-generation poly(amidoamine) (PAMAM) dendrimer to deliver siRNA targeting tumor necrosis factor α (TNF-α) to treat acute lung inflammation. The results of their experiment revealed that the PAMAM dendrimer–siRNA complexes (dendriplexes) led to a high degree of siRNA coagulation and excellent uptake by RAW264.7 macrophages, and these complexes exhibited highly efficient and specific TNF-α silencing compared with siRNA administered alone. In vivo experiments confirmed that PAMAM dendriplexes induced effective siRNA-mediated TNF-α inhibition in the lungs of mice with LPS-induced inflammation, and these results were different from those observed after the administration of free siRNA. These results suggest that PAMAM dendrimer nanocarriers can significantly enhance the efficiency of TNF-α-targeting siRNA delivery and thus can be used to effectively treat pulmonary inflammation (Table 1). 28 In addition, Gao et al. constructed a novel nanocarrier (G5.NH2-PBA) that was synthesized based on generation 5 (G5) PAMAM dendrimers, modified with phenylboronic acid (PBA), and coated with fibronectin (FN), which is used in the treatment of ALI caused by inflammation. The G5.NH2-PBA carrier showed good cytocompatibility, and at an optimized dendrimer-to-FN weight ratio of 8, the carrier efficiently delivered FN into cells, thus promoting the polarization of macrophages toward the anti-inflammatory M2 phenotype. The G5.NH2-PBA system-mediated intracellular delivery of FN significantly reduced TNF-α and IL-1β secretion, inhibited nuclear factor-κB (NF-κB) pathway activation, and increased ROS scavenging, thereby effectively inhibiting the LPS-induced inflammatory response. Moreover, mice with LPS-induced ALI were treated with G5.NH2-PBA and the symptoms of ALI were effectively relieved by reducing lung inflammation and oxidative stress 29 (Figure 2 and Table 1). Therefore, these PAMAM dendrimer-based nanocarriers may be a novel strategy for the treatment of ALI and other inflammatory diseases.

Poly(amidoamine) dendrimer mediated intracellular delivery to alleviate acute lung injury. (a) The synthesis of G5.NH2-PBA and formation of Den/FN complexes. (b) Treatment of LPS-induced ALI mouse models with G5. NH2-PBA effectively relieved the symptoms of ALI.
Phosphorus dendrimers
Phosphorus dendrimers are commonly synthesized by introducing phosphate-containing units (such as hachlorocyclotrimonitrile and thiophosphate) into PAMAM dendrimers. Phosphorus dendrimers are widely used as nanocarriers to treat several diseases due to the highly branched, symmetrical structure and highly uniform molecular weight distribution of traditional dendrimers as well as the good biocompatibility that is conferred by phosphorus. Studies have shown that phosphorus dendrimers can be used as effective nanocarriers of oligodeoxynucleotides or small interfering RNAs (siRNAs).46,47 As the molar ratio between the positively charged groups of the dendrimer and the phosphate in the siRNA skeleton increases, the surface potential of the cationic phosphorus dendrimer/siRNA complex changes from negative to positive, and the hydrodynamic diameter gradually increases. More importantly, the siRNA molecules in the complex do not change, indicating that cationic phosphorus dendrimers can effectively prevent RNA digestion and can be used as effective nanocarriers for RNA-based disease therapy. 46 Bohr et al. designed and synthesized two kinds of protonated cycloamine (pyrrolidinium or morpholinium)-modified cationic phosphorus-based dendrimers and used them as siRNA nanocarriers for the treatment of ALI in mice. The results showed that in LPS-treated mouse RAW264.7 macrophages, dendriplexes containing pyrrolidinium surface groups exhibited stronger siRNA complexation, greater cellular uptake, and enhanced TNF-α silencing efficiency in vitro compared to morpholinium-containing dendriplexes. In addition, the superior effect of pyrrolidinium dendriplexes was shown to significantly ameliorate ALI in mice with LPS-induced ALI. These results suggest that phosphorus dendriplexes have a strong potential for use in the delivery of siRNA for the treatment of inflammatory lung diseases. 48 Li et al. developed a novel gene-delivery nanocarrier based on pyrrolidinium-modified amphiphilic generation 1 phosphorus dendron (C12G1) nanomicelles, which formed a rigid phosphorous dendritic structure and exhibited excellent biocompatibility. Compared with the pyrrolidinium-modified G1 phosphorus dendrimer material, the C12G1 in these nanocarriers resulted in greater gene delivery efficiency. C12G1 nanoparticles were used to codeliver miRNA-146a mimics (miR-146a mimic) and a miRNA-429 inhibitor (miR-429i). The results showed that C12G1 significantly inhibited the secretion of the proinflammatory cytokines TNF-α, IL-1β, and IL-6 and the polarization of alveolar macrophages toward the M1 phenotype. Therefore, the C12G1/miR-mixture polyplexes significantly suppressed inflammatory cell infiltration and alveolar wall damage in lung tissues in vivo, effectively alleviating ALI in LPS-treated mice 30 (Table 1).
Novel inorganic nanoparticles
Inorganic nanoparticles (NPs) are a class of nanoparticles that can be synthesized by physical or chemical methods; these NPs have a variety of morphologies and a size range of 1–100 nm. They are usually composed of inert metals and biocompatible metals. NPs include metal nanomaterials, such as gold, silver, gadolinium, hafnium oxide, iron oxide, and quantum dots, and inorganic nonmetallic nanomaterials, such as carbon and black phosphorus. The surface of NPs is easily modified, and it can be combined with drug molecules in different ways, such as through electrostatic interactions, hydrophobic interactions, and covalent bonds between enzyme-sensitive groups, to achieve responsive cargo release; thus, these NPs are ideal choices for drug delivery. In addition to the ease of surface modification, NPs are simpler to prepare than other nanomaterials, and they have higher drug-loading capacity and better biocompatibility for drug delivery; these NPs exert greater therapeutic effects. For example, gold nanoparticles (GNPs) are becoming the preferred delivery system for anti-inflammatory drugs because of their easy synthesis, controllable size, and relative safety, and their surface can be easily modified with peptides, allowing them to exhibit novel biological activities. Wang et al. constructed a novel anti-inflammatory nanoparticle (P12) based on a gold nanoparticle (GNP) whose surface was coated with a hexapeptide (amino acid sequence of CLPFFD); P12 effectively reduced lung inflammation and injury by inhibiting TLR signaling pathways in macrophages. In vivo experiments showed that P12 alleviated lung inflammation and injury in mice with LPS-induced ALI by reducing the number of infiltrating inflammatory cells and increasing the levels of anti-inflammatory cytokines (IL-10) in the lungs. In addition, P12 promoted the polarization of mouse bone marrow-derived macrophages toward the anti-inflammatory M2 phenotype. In ALI mouse models, P12 increased alveolar M2 macrophage numbers and reduced both alveolar and interstitial M1 macrophage numbers in bronchoalveolar lavage fluid (BALF) and lung tissues. These results confirmed that hexapeptide-coated GNPs can induce the polarization of M2 macrophages in vivo and in vitro, effectively regulate lung inflammation, protect the lung from damage, and promote the attenuation of inflammation. Therefore, peptide-GNP hybrids that regulate macrophage polarization and inhibit TLR signaling pathways represent a new generation of safe and effective anti-inflammatory nanomedicines for the treatment of ALI. 31
Mesoporous silica nanoparticles (MSNs), which are novel inorganic materials, possess excellent characteristics, such as a high specific surface area, large pore volume, controllable particle size, and good biocompatibility. Compared to other carriers, MSNs have a higher loading efficiency, and thus, they are widely used in the field of biomedicine. Importantly, due to the ability of MSNs to preferentially accumulate in lung tissues and sites of inflammation, they may have advantages over other nanoparticles in the treatment of ALI.49,50 For instance, García-Fernández et al. constructed an MSN nanocarrier that was loaded with dexamethasone, and a TNFR1 receptor peptide (GGGGFIGLMYRYQRWKSKLY) was anchored onto the surface. The high specific surface area and large pore volume of MSNs allowed these particles to carry higher loads and prevented cargo leakage. In addition, the TNFR1 receptor peptide on its surface facilitated the internalization of TNFR-Dex-MSNs by activated proinflammatory macrophages, leading to enzymatic degradation and cargo release within lysosomes. Through the action of TNFR-Dex-MSNs, the levels of TNF-α and IL-1β that were produced by activated proinflammatory M1 macrophages were significantly decreased. Moreover, in an LPS-induced ALI mouse model, the accumulation of TNFR-Dex-MSNs at the site of injured lung tissue after their intravenous injection significantly decreased the inflammatory response by controlling dexamethasone release. Using MSNs as carriers promotes drug transport and release, enabling targeted dexamethasone delivery to the lungs and decreasing dexamethasone-induced side effects. This research establishes MSNs as a potential efficient drug delivery system for the treatment of ALI (Figure 3 and Table 1). 32

The application of mesoporous silica nanoparticles (MSN) to treat acute lung injury. (a) Design of the TNFR-MSNs nanodevices for acute lung injury therapy. (b) Evaluation of the therapeutic effect of TNFR-Dex-MSNs in LPS-ALI mice.
Metal-organic frameworks
Metal-organic frameworks (MOFs) are coordination polymers that are composed of metal ions and organic ligands. Due to the diversity of metal ions and the different modes of organic ligand coordination, synthesized MOFs exhibit high porosity, structural diversity, and controllable functionality. Modifying MOFs allows the generation of novel functional materials. Compared to other porous nanomaterials, MOFs have strong adaptability to nanoparticle pore sizes. Nanomedicines that include MOFs as carriers can be adapted to the size of drug particles, increasing drug loading. In addition, MOFs have high permeability and retention properties, enabling passive targeting in the treatment of disease. 51 Furthermore, recent studies have revealed the potential efficacy of MOFs in the treatment of ALI. 52 For instance, Wang et al. utilized zeolitic imidazolate framework-8 (ZIF-8) as a drug carrier for treating lung injury. ZIF-8 is a MOF material that is composed of Zn2+ and 2-methylimidazolate ZIF-8 requires mild preparation conditions, has a tunable size, and can be loaded with various small and large molecules through in situ encapsulation or postmodification. Moreover, ZIF-8 spontaneously degrades under acidic pH conditions, allowing it to function as a stimulus-responsive drug carrier. These authors prepared PLB@ZIF-8 nanoparticles by encapsulating plumbagin (PLB) onto ZIF-8; that is, PLB was adsorbed onto the ZIF-8 nanoparticles through π–π stacking interactions. The high surface area of ZIF-8 significantly enhanced PLB adsorption and facilitated its effective release in vivo. In an LPS-induced mouse model of lung injury, PLB@ZIF-8 significantly reduced the secretion of the inflammatory factors TGF-β and IL-6. In addition, the expression of collagen I, α-SMA, and TNF-α was suppressed. Therefore, PLB@ZIF-8 shows promise as a novel approach for treating severe lung injuries. 33 Furthermore, Weng et al. developed a nanoscale Zr(IV)-based porphyrin metal-organic framework (ZPM) that is capable of effectively delivering siRNA targeting zinc finger E-box binding homeobox 1 and 2 (ZEB1/2), thereby alleviating early pulmonary fibrosis during ALI. ZEB1/2 is closely associated with the progression of early lung fibrosis. 53 Targeting siRNA to lung tissues to silence gene expression can be an effective molecular therapy for lung injury. However, the large molecular weight (~14 kDa), abundant negative charge, and poor stability of free siRNA molecules limit their application.54,55 Weng et al. coupled nanoscale ZPM with poly(2-diethylamino) ethyl methacrylate (PDEA)-branched polyethyleneimine (bPEI) (PDE). Utilizing the strong binding affinity between bPEI and siRNA, along with the ultra-pH-sensitive nature of PDEA (pKa ≈ 6.4), ZPM@PDE-siZEB1/2 enters cells through endocytosis, undergoes rapid protonation in endosomes/lysosomes (pH 4.5–6.0), which facilitates endosomal escape, and releases siRNA into the cytoplasm. Ultimately, ZPM@PDE nanoparticles effectively delivered siZEB1/2, significantly inhibited ZEB1/2 expression, and alleviated early pulmonary fibrosis in LPS-treated mice (Figure 4 and Table 1). 34

The application of MOFs to treat acute lung injury. (a) The scheme for ZPM@PDE-siZEB1/2 preparation and intratracheal therapeutic mechanism of ZPM@PDE-siZEB1/2 in ALI model mice. (b) Histopathological changes of lung tissue in ALI mice after treatment with ZPM@PDE-siZEB1/2.
Nanozymes for the treatment of ALI
Nanozymes are novel nanomaterials with enzyme-like activities. Nanozymes, which are recently developed artificial enzymes, have contributed to the field of simulated enzymes. Nanozymes catalyze substrates under mild or extreme conditions and convert them into products through enzymatic kinetics, such as the property represented by the Michaelis–Menten equation. Compared with traditional enzymes, nanozymes have advantages such as high catalytic activity, functionality under mild reaction conditions, good stability, and inexpensive and large-scale production. Nanozymes are classified as oxidoreductases, hydrolases, synthases, and isomerases according to their catalytic activity. Many nanomaterials have been reported to exhibit unique oxidoreductase-mimicking activities. For example, Fe3O4, Au, and carbon nanotubes have very high peroxidase (POD)-like catalytic activity.56–58 CeO2 exhibits oxidase (OXD)-like activity. 59 In addition, Pt, Pd, MnO2, etc., show unique catalase (CAT)- and superoxide dismutase (SOD)-like activities, enabling them to effectively scavenge harmful ROS and play important roles in cell protection, especially via their anti-inflammatory effects.60–62
Inflammation is a normal immune response and is normally beneficial for the body. However, when inflammation in the body is dysregulated, acute inflammation can become chronic and lethal. The inflammatory response is closely related to the excessive production of ROS; therefore, antioxidants are extremely important in the treatment of inflammation. 63 In recent years, many nanozymes, such as SOD- and CAT-like nanozymes, have been shown to exhibit activity similar to endogenous antioxidants. Specifically, nanozymes can mimic endogenous antioxidant systems and participate in cell protection. Nanozymes with CAT-, SOD-, glutathione peroxidase (GPx)-like activities and other activities can decompose ROS into molecules that are characterized by low reactivity, such as H2O or O2, to relieve cellular oxidative stress; therefore, they can be used as antioxidant therapeutic agents. For example, Huang et al. combined selenium with dopamine to construct Se@pDA nanozymes. Se@pDA nanozymes possessed excellent GPx-mimicking activity and catalyzed the decomposition of H2O2 to produce nontoxic products in the presence of glutathione (GSH). In addition, the dopamine component scavenged toxic ROS, such as ·OH and O2•−, and thus played an antioxidant role. Therefore, these Se@pDA nanozymes showed excellent ROS-scavenging abilities, which effectively attenuated ROS-induced oxidative damage to lipids and DNA and significantly alleviated damage in mice with lipopolysaccharide (LPS)-induced pneumonia. 35
Nanozymes benefit anti-inflammatory therapy due to their potent anti-inflammatory properties, ROS-scavenging capabilities, and ability to function as combination drug carriers that can be loaded with certain antioxidant active ingredients, thereby enhancing overall anti-inflammatory effects. For instance, nanozymes that are constructed using FeCl3 and poly(vinylpyrrolidone) (PVP) can efficiently encapsulate curcumin, functioning as a combined antioxidant nanomedicine. The Fe nanoparticles in the nanozymes can scavenge ROS, while curcumin is a natural antioxidant that suppresses inflammation. Fe-Cur NP treatment significantly reduced the levels of TNF-α, IL-1β, and IL-6 in the serum and bronchoalveolar lavage fluid (BALF) of mice with ALI, reduced the release of intracellular Ca2+ and inhibited NLRP3 inflammasome and NF-κB signaling pathway activation. In addition, Fe-Cur NPs were intratracheally and intravenously injected into mice with ALI, and the accumulation of these nanozymes in lung tissues was higher than that of free curcumin, confirming the therapeutic efficacy of nanozymes in ALI. Moreover, Fe-Cur NPs decreased the numbers of macrophages (CD11bloF4/80hi) and CD3+CD45+ T cells in the lungs of mice with ALI, contributing to decreasing the inflammatory cytokine storm that was induced by ALI. More importantly, these nanoparticles were noncytotoxic in vivo. Therefore, Fe-Cur NPs can eliminate intracellular ROS via their nanozyme activity and be used in synergistic ALI treatment via their anti-inflammatory nanomaterials, making them promising therapeutic agents for the clinical treatment of ALI. Fe-Cur NP nanozymes were designed to attenuate ALI by clearing intracellular ROS and synergistically reducing inflammation. 36
The modifiable properties of nanozymes allow them to potentially be applied for targeted therapy. For example, the preparation of AOzyme@ACM, which uses an apoptotic cell membrane (ACM) to encapsulate antioxidant nanozymes (AOzyme), enhances macrophage recognition of ‘eat me’ signals by simulating apoptotic bodies, thereby effectively enhancing the clearance of apoptotic cells. In addition, the AOzyme nanozyme portion comprises HMnO2 and Cu NPs. Cu NPs can scavenge a wide range of ROS, including H2O2, O2•−, ·OH, and other free radicals. MnO2 effectively eliminates H2O2. Therefore, the HMnO2-Cu composite in AOzyme@ACM exhibits antioxidase-mimicking activity and efficiently scavenges ROS. Therefore, AOzyme@ACM treatment significantly inhibited inflammation in mice with LPS-induced ALI, promoted macrophage polarization toward the M2 phenotype, and suppressed the activation of the NF-κB signaling pathway, thereby reducing inflammatory cell infiltration and alleviating edema in mice with ALI (Figure 5 and Table 1). 37 Wu et al. designed an H2O2-reactive nanocarrier that targeted the removal of bacterial toxins and pathogenic bacteria at sites of infection, thus alleviating damage to infected tissues and reducing bacterial diffusion; this study suggested a new approach for the clinical treatment of toxin-secreting bacteria. Clinically, bacterial pathogens secrete toxic substances that cause tissue damage. H2O2, which is a critical bacterial toxin, can seriously damage infected tissues and increase blood vessel leakage, leading to life-threatening systemic bacteremia or septicemia. However, no treatment can alleviate the damage that is caused by bacterial hydrogen peroxide or prevent sepsis. Wu et al. developed H2O2-reactive metal-organic framework nanosystems (MOFs) for the treatment of infections with H2O2-secreting bacteria, such as Streptococcus pneumoniae (S. pneumoniae). These authors constructed Fe3+-doped MOFs that were loaded with ampicillin (nFMs@Amp) to sequester the H2O2 that is secreted by S. pneumonia. nFMs@Amp exhibited catalase (CAT)-like activity and catalyzed the decomposition of H2O2 through a Fenton/Fenton-like reaction. In addition, the hydroxyl radical (·OH) that was produced by this reaction exerted a chemodynamic bactericidal effect on drug-resistant bacteria, and Amp was released from nFMs@Amp to specifically kill drug-sensitive bacteria. In vivo experiments demonstrated that after intravenous (i.v.) injection, nFMs@Amp efficiently crossed the damaged alveolar-capillary barrier and accumulated in infected lungs, where it eliminated the H2O2 that was secreted by S. pneumoniae via MOF activity, reduced endothelial DNA damage, and prevented systemic bacterial spread; thus, this agent significantly increased the survival rate of mice. Therefore, the use of nFMs@Amp for the treatment of lethal streptococcal infection in mice was highly effective, and these results suggested new approaches for the clinical treatment of infection with H2O2-secreting bacteria (Table 1). 38 Moreover, many nanozymes can not only eliminate ROS but also regulate the immune system to synergistically relieve inflammation. 64
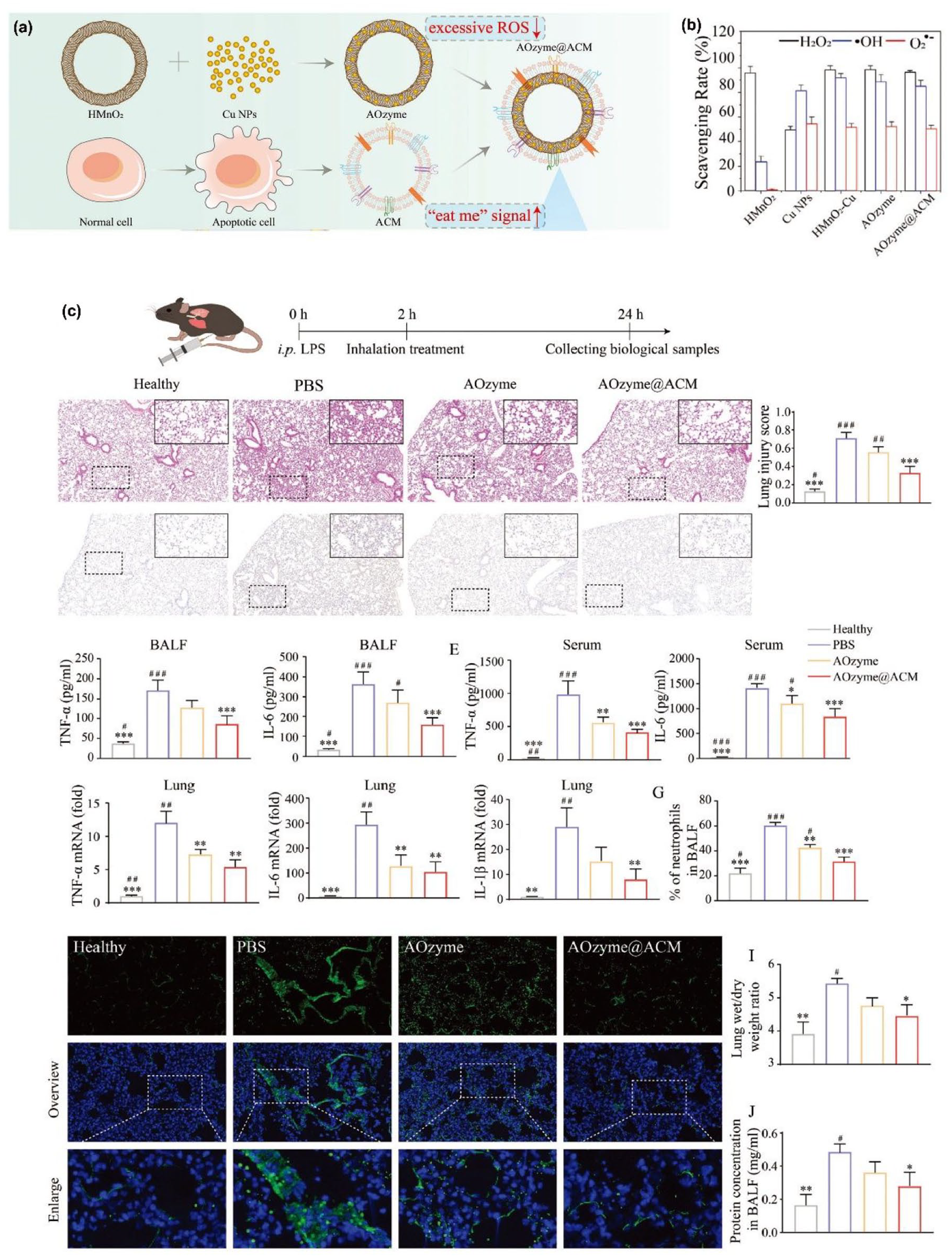
Nanozymes for the treatment of acute lung injury. (a) The synthesis of apoptotic cell membrane-coated antioxidant nanozymes (AOzyme@ACM). (b) ROS scavenging capabilities of AOzyme@ACM. (c) Pro-efferocytic AOzyme@ACM alleviated sepsis-related acute lung injury.
Carbon nanodots (C-dots), which are fluorescent nanomaterials, have attracted considerable attention due to their unique properties. 65 There are abundant oxygen-containing functional groups on the surface of C-dots, such as hydroxyl, carboxyl, and amino groups, which endow C-dots with effective antioxidant enzymatic activities. 66 In addition, C-dots exhibit catalytic activity due to their small size and abundant active sites. C-dots show great potential for application in the treatment of diseases, especially ROS-related diseases. 67 Therefore, C-dots have been extensively studied in the treatment of inflammatory diseases, such as ALI. For example, Wang et al. prepared C-dots from L-ascorbic acid via a one-step electrochemical method, and the products exhibited excellent ROS-scavenging activity and significantly inhibited LPS-induced inflammatory responses. In mice, C-dots were completely degraded into CO2 and H2O at 37°C without damaging tissues. In addition, C-dots significantly upregulated heme oxygenase 1 (HMOX1) expression by regulating BACH1 signaling pathway activation and reduced ROS levels in cell models of LPS-induced inflammation. In vivo experiments confirmed that C-dots effectively attenuated ALI and increased the survival rate of mice. In these experiments, C-dots that were synthesized from L-ascorbic acid showed the potential to treat ALI. 39 In addition, Zhao et al. prepared C-dots from Armeniacae Semen Amarum Carbonisata (ASAC-CDs) via a one-step calcination strategy, and these CDs exerted good antioxidant effects. ASAC-CDs alleviated LPS-induced inflammation by reducing the levels of inflammatory factors, including IL-6, IL-1β, and TNF-α. More importantly, ASAC-CDs attenuated the increase in neutrophil numbers in the blood and, to a certain extent, reduced the chemotaxis that drives neutrophils to sites of inflammation, thereby reducing the secretion of inflammatory mediators and alleviating the lung tissue injury and exacerbated symptoms. These experiments showed that ASAC-CDs exert a certain defensive effect against LPS-induced ALI and their mechanism of action may be closely related to their antioxidant effects and ability to suppress inflammation and thus decrease respiratory edema (Table 1). 40 The C-dot nanozymes effectively entered cells and accumulated in mitochondria, protecting cells from oxidative damage by scavenging ROS and reducing proinflammatory cytokine levels. The C-dot SOD nanozyme achieved effective targeting of the site of inflammatory lung injury, and the therapeutic effect of this nanozyme on lung injury in mice was comparable to that of the clinical drug dexamethasone. Thus, C-dot nanozymes will provide a foundation for the development of ultrasmall nanozymes with high catalytic activity, which will promote their application in the treatment of inflammatory diseases. 41
Nanovaccines for the treatment of lung injury
Nanovaccines are a new generation of vaccines based on nanotechnology, and vector design and surface ligand modification allow nanovaccines to elicit long-term and effective immune responses. Nanovaccines have advantages over conventional vaccines in terms of lymph node accumulation, antigen assembly, and antigen presentation. Nanotechnology can promote the processing of nanovaccines as targets for the immune response. Once nanovaccines are internalized by antigen-presenting cells (APCs), nanoparticles induce the formation of inflammasome complexes, the secretion of inflammatory cytokines, and the recruitment of immune cells. Nanovaccines increase antigen stability and target antigen-presenting cells, promote the maturation of these cells, and activate specific immune responses. In addition, by adjusting the shape, particle size, and charge of nanovaccines or by applying surface modification, scientists can enhance the tissue targeting capacity of these vaccines, increase the efficiency of their uptake by cells, and reduce their cytotoxic effects. Therefore, nanovaccines show great promise in the treatment of ALI caused by pneumonia.
Notably, Wu et al. prepared nanovaccines using bacterial outer membrane vesicles (OMVs) to treat bacterial pneumonia caused by P. aeruginosa by stimulating the immune response. Most bacteria secrete OMVs during their life cycle. These OMVs are nonreplicable bilayer structures that carry large loads of virulence-related proteins that can be used as potential bacterial vaccine candidate antigens to prevent antibiotic overuse. This group synthesized a biocompatible nanovaccine (LPS@DMON@OMV) using dendritic mesoporous silicon nanoparticles (DMONs) as carriers, loaded these carriers with an appropriate amount of adjuvant lipopolysaccharide (LPS), and coated these carriers with OMV antigen. After injection into mice, the LPS@DMON@OMV nanovaccine was rapidly captured by dendritic cells (DCs), which cross-presented the antigens to stimulate DC maturation in lymph nodes. Then, histocompatibility complex-I (MHC-I) on the surface of mature DCs presented these antigens to CD8 T cells to induce cellular immunity. In addition, MHC-II on the surface of mature DCs interacted with receptors on helper T cells, triggering subsequent humoral immunity. Ultimately, this approach exerted immunotherapeutic effects against pneumonia through both cellular immunity and humoral immunity. More importantly, the memory cells that were formed during the process of immunization effectively prevent secondary bacterial infections. In addition, these nanovaccines were susceptible to internalization by DCs in three-dimensional space, ensuring adequate antigen uptake. In addition, these antigens interacted with the T-cell receptor on the surface of T cells through cross-presentation and activated T cells via their interaction with helper molecules in vivo. After injection of LPS@DMONs@OMV, the immune system of mice was quickly and effectively activated, and toxic CD8+ T cells were thus produced to effectively eliminate bacteria in the mice, specifically reducing the bacterial load in the lungs. Moreover, LPS@DMON@OMV was rapidly and safely metabolized in vivo, showing good biocompatibility. Therefore, LPS@DMON@OMVs represent a feasible strategy for acute pneumonia with immunotherapy (Figure 6 and Table 1). 42 Du et al. prepared a multiepitope peptide nanovaccine and evaluated its immunogenicity and protective effect in BALB/c mice. These authors selected outer membrane protein 22 (Omp22) from A. baumannii as the candidate antigen and screened the optimal B-cell and T-cell epitopes of Omp22 (rOmp22). Then, rOmp22 was encapsulated with chitosan (CS) and poly(lactic-co-glycolic) acid (PLGA) to construct the CS-PLGA-rOmp22 nanovaccine. BALB/c mice that were immunized with CS-PLGA-rOmp22 exhibited increased levels of rOmp22-specific IgG in their serum and IFN-γ in splenocyte supernatants. In addition, BALB/c mice that were inoculated with CS-PLGA-rOmp22 exhibited reduced lung injury and decreased bacterial burdens in the lungs and blood, and CS-PLGA-rOmp22 effectively protected these mice against acute fatal intratracheal A. baumannii challenge. Thus, the CS-PLGA-rOmp22 nanovaccine elicited specific IgG antibodies, triggered Th1 cell-based immunity, and protected against acute lethal intratracheal A. baumannii challenge in BALB/c mice (Table 1). 43

Nanovaccines for the treatment of acute lung injury. (a) A schematic diagram of the antibacterial immune regulation of nanovaccine encapsulated by bacterial OMVs. The nanovaccine induced bacteria-specific immunity against the source bacteria and produced specific antibodies and toxic T cells, which were used to treat acute pneumonia and prevent infection. (b) The treatment effect of pneumonia by injecting serum containing the antibody and pure serum in vivo. Blood routine analysis and bacterial burden in the lungs of mice.
Limitations and prospects
One advantage of nanomedicines over traditional drugs is their ability to be used in combination therapy. Nanocarriers can efficiently deliver anti-inflammatory or antioxidant drugs, such as dexamethasone, resveratrol, and curcumin. In addition, polymer- or lipid-based nanocarriers and peptides can be used to deliver various nucleic acids, including cDNA, plasmid DNA, siRNA, and miRNA. Multiple drugs can be incorporated into nanocarriers to achieve codelivery, enhance the efficiency of drug delivery, reduce off-target side effects, and exert synergistic therapeutic effects. Furthermore, targeted delivery through nanocarriers can improve the pharmacokinetic properties of therapeutic agents. Many nanocarriers have characteristics that are desirable for drug delivery, especially characteristics that improve the solubility, stability, or activity of hydrophobic agents, nucleic acids, enzymes, and peptides.28,47 Some traditional drugs, such as the Src tyrosine kinase inhibitor (PP2) and sivelestat, have disadvantages such as insufficient solubility, poor stability, and short in vivo half-lives, and these disadvantages significantly impact treatment outcomes and lead to suboptimal clinical results.68–70 The development of nanocarriers effectively overcomes limitations related to drug efficacy and stability, and these nanocarriers allow efficient delivery. Importantly, through the modification of targeting ligands, nanocarriers can significantly alter the biological distribution of drugs, resulting in their accumulation at inflammatory sites, decreased nontargeted side effects, targeted delivery, improved efficiency, and reduced toxicity; thus, nanocarriers have significant clinical importance. 17 Moreover, modifications of nanocarriers to improve active targeting can be achieved using specific molecules that are highly expressed in the inflammatory microenvironment, enabling more precise distribution. 71
The emergence of nanomedicine provides new directions for overcoming the limitations of traditional drug treatment, but challenges remain in enhancing the clinical translation of these agents. Although nanoparticles have certain advantages in terms of particle size, easy synthesis methods, surface modification capacity, and biocompatibility, in vivo analyses of their behavior, toxicity, biological distribution, and clearance are difficult, but these evaluations are necessary for their clinical application. By modifying biological membranes and employing other optimization methods, nanomedicine delivery systems can overcome biological barriers, including clearance and degradation mechanisms as well as physical barriers such as the lung barrier. In addition, these systems can capitalize on the excessive recruitment of inflammatory cells, enabling targeted delivery to inflamed lungs. Based on these mechanisms, nanocarriers have tremendous potential for increasing lung distribution and cellular uptake while simultaneously limiting toxic side effects. Nanomedicines can target hyperactivated immune cells and incorporate therapeutic agents with anti-edema activity via conjugation or encapsulation within nanomedicines. Through passive, active, or physicochemical targeting, they interact with pulmonary epithelial/endothelial cells and inflammatory cells, reversing abnormalities, restoring lung homeostasis, and demonstrating good therapeutic activity. Therefore, the use of nanomedicines for treating ALI presents a wide range of alternative treatment strategies, including delivering anti-inflammatory drugs to the site of the disease, directly clearing inflammatory factors, regulating the activity of inflammatory cells, or modulating inflammatory signaling pathways.
Some nanomedicines are in clinical use, but many are still in clinical trials, and these clinical trials are mostly focused on the use of nanomedicines for in vivo imaging rather than drug delivery. Therefore, ways to translate nanomedicines into clinical drugs need to be identified, and this line of research is urgently needed in the future.
Conclusion
The clinical treatment of ALI prioritizes supportive care and mechanical ventilation. Although some preclinical studies demonstrated the benefits of drug interventions, to date, these measures have not been proven to be entirely effective, and no pharmacological therapy has been established as a fully effective treatment for ALI. In the past few decades, a variety of nanocarriers, such as liposomes, microemulsions, nanoemulsions, nanogels, polymeric micelles, and polymeric nanoparticles, have been widely used for the efficient delivery of drugs. Changing the size, morphology, and surface chemical groups of nanoparticles can improve the biological distribution of these agents in the body as well as tissue targeting, thereby optimizing therapeutic effects. Therefore, nanoparticles have gradually become a powerful tool for the treatment of human immune-related diseases. In addition to optimized nanocarriers, nanozymes and nanovaccines have been used as effective nanomaterials for the treatment of inflammatory diseases in recent years. Recent advances in nanotechnology may provide new perspectives for the treatment of ALI with drugs.