
Abstract
Background:
The modified NUTRIC (nutritional risk in the critically ill) score has been reported to predict clinical outcomes in critically ill patients. However, the applicability of this score may differ between patients undergoing short-term mechanical ventilation (STMV, < 96 h) and those undergoing prolonged acute mechanical ventilation (PAMV, ⩾96 h), as PAMV patients typically experience significantly higher morbidity and mortality.
Objective:
This study aimed to investigate the predictive ability of modified NUTRIC score for predicting 28-day mortality in patients receiving STMV and PAMV.
Design:
Retrospective single-center cohort study.
Methods:
We enrolled patients who received mechanical ventilation (MV) on the day of admission to the intensive care unit (ICU) from 1 December 2015 to 30 November 2020. Modified NUTRIC scores were calculated based on the clinical data of each patient at ICU admission.
Results:
The study population comprised 464 patients, including 319 (68.8%) men with a mean age of 69.7 years. Among these patients, 132 (28.4%) received STMV and 332 (71.6%) received PAMV. The overall 28-day mortality rate was 26.7%, which was significantly higher in STMV patients than in PAMV patients (37.9% versus 22.3%, p < 0.001). Evaluation of the predictive performance of the modified NUTRIC score for 28-day mortality revealed areas under the receiver operating characteristic curves of 0.672 [95% confidence interval (CI): 0.627–0.714] for total patients, 0.819 (95% CI, 0.742–0.880) for STMV patients, and 0.595 (95% CI, 0.540–0.648) for PAMV patients. The best overall cutoff value was 5 in total, STMV, and PAMV patients. This cutoff value was a significant predictor of 28-day mortality based on the Cox proportional hazard model for total [hazards ratio (HR): 2.681; 95% CI: 1.683–4.269] and STMV (HR: 5.725; 95% CI: 2.057–15.931) patients, but not for PAMV patients.
Conclusion:
The modified NUTRIC score is more effective in predicting 28-day mortality in patients undergoing STMV than in those undergoing PAMV.
Plain language summary
In this study, we examined the scoring system called the Modified NUTRIC (nutritional risk in the critically ill) score to determine whether it could be used to predict 28-day mortality following Intensive Care Unit (ICU) admission. In particular, we wanted to determine whether the score works equally well for patients who need short-term mechanical ventilation (STMV, less than 96 hours) and those who need prolonged acute mechanical ventilation (PAMV, 96 hours or more). PAMV patients tend to have more severe illness and use more medical resources.
Here’s what we did:
We studied 464 patients who were put on a breathing machine (mechanical ventilation) on the same day they were admitted to the ICU between December 1, 2015, and November 30, 2020. We calculated the Modified NUTRIC (m-NUTRIC) scores based on their medical information when they entered the ICU. We found that the overall 28-day mortality was 26.7%, and that it was higher for STMV patients (37.9%) than for PAMV patients (22.3%). When we checked how well the m-NUTRIC score predicted survival, we discovered that it worked better for STMV patients (with an accuracy of 81.9%) than for PAMV patients (with an accuracy of 59.5%). We also found that a m-NUTRIC score of 5 or more points was indicative of a higher mortality in STMV patients
In conclusion, the m-NUTRIC score is a more reliable predictor of 28-day survival in patients who need short-term mechanical ventilation than in those who need prolonged acute mechanical ventilation.
Introduction
Because higher nutritional risk in critically ill patients is usually associated with poor prognosis, the identification of patients at higher nutritional risk is clinically necessary.1,2 The ‘Nutritional Risk in the Critically Ill’ (NUTRIC) score was the first assessment tool designed to evaluate nutritional risk in critically ill patients. 3 A modified version of the NUTRIC score, which includes all factors used to calculate the NUTRIC score except for serum interleukin-6 (IL-6) concentration, has also been reported to predict clinical outcomes in various groups of critically ill patients.4–9
Mechanical ventilation (MV) is an essential life-saving medical resource for patients undergoing acute deterioration in the intensive care unit (ICU). Patients requiring MV in the ICU include those undergoing short-term MV (STMV, <96 h) and prolonged acute MV (PAMV, ⩾96 h), with the latter reported to have significantly higher morbidity and mortality rates and greater utilization of resources.10,11 Few studies to date, however, have evaluated the usefulness of the modified NUTRIC (m-NUTRIC) score to determine the association between mortality and the duration of MV. The present study hypothesized that the ability of the m-NUTRIC score to predict mortality would differ in patients receiving STMV and PAMV.
The current study examined this hypothesis by evaluating the effectiveness of the m-NUTRIC score and determining the optimal cutoff value for predicting 28-day mortality in patients with pneumonia undergoing mechanical ventilation in the ICU. This study also compared the ability of the m-NUTRIC score to predict 28-day mortality in patients who underwent STMV and PAMV.
Materials and methods
Study design and patient selection
In this retrospective, observational cohort study, we evaluated all individuals aged 18 years and older who were admitted to a 12-bed adult respiratory ICU at a regional respiratory disease center from 1 December 2015 to 30 November 2020. This center is part of a tertiary care, university-affiliated hospital with a capacity of 1200 beds. All patients were managed according to therapeutic recommendations based on a ‘lung-protective ventilator strategy’. 12
Patients were included if (1) they had received ventilator care on the day of ICU admission, (2) the duration of ventilation was >24 h, and (3) pneumonia (community-acquired and hospital-acquired) was the main reason for MV at ICU admission. The definitions of community-acquired and hospital-acquired pneumonia were based on those reported previously in the literature.13,14 The study was intended to validate the m-NUTRIC score according to the duration of ventilation. Because differences in the day of ICU admission and the day of intubation would lead to inaccurate results, patients who had first received ventilator care after 24 h of ICU admission were excluded. Patients with irreversible brain injury or neuromuscular diseases were also excluded, regardless of length of ICU stay. The primary study outcome was 28-day mortality after the day of intubation. STMV was defined as ventilator care for <96 h, whereas PAMV was defined as ventilator care for ⩾96 h. 10 The reporting in this study conforms with the guidelines in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 15 The STROBE checklist was provided in Supplemental Material 1.
Data collection
Demographic and clinical parameters such as age, sex, and body mass index (BMI) were extracted from the electronic medical records (EMRs) of each subject. The severity of illness was quantified using the Acute Physiology and Chronic Health Evaluation (APACHE) II scoring system, while organ dysfunction was assessed by the Sequential Organ Failure Assessment (SOFA) score,16,17 with both of these scores calculated based on clinical and laboratory data at the time of ICU admission. The underlying comorbidities of all enrolled subjects on admission were obtained from their EMRs and recorded utilizing Charlson’s weighted index for evaluation. 18 Mortality within 28 days after ICU admission was assessed by review of the National Health Insurance Service database. 19
The m-NUTRIC scores were calculated based on the reported data. 4 To evaluate the associations between m-NUTRIC scores and patient medical expenditures at hospital discharge, total and out-of-pocket medical expenditures for all medical resources (including all medicines) during the hospital stay (ICU and general ward) were obtained from the patient EMRs. All medical costs are expressed in United States Dollars (USD) using a Korean Won to USD exchange rate of 1 USD = 1471.00 Korean Won (exchange rate on 1 November 2022).
Statistical analysis
Continuous variables following a normal distribution were expressed as mean ± standard deviation and analyzed using Student’s t-tests. For continuous variables not adhering to the normal distribution, the median and interquartile ranges were calculated and examined using Wilcoxon rank-sum tests. Categorical variables were denoted as counts and percentages and assessed using the chi-square (χ2) or Fisher’s exact test where applicable. The relationships between m-NUTRIC scores and other clinical variables were evaluated by determining Pearson’s correlation coefficients (γ).
Patient survival analysis was conducted employing the Kaplan–Meier method and compared using the log-rank test. Factors that were significantly associated with 28-day mortality were subjected to further analysis using a Cox proportional hazard model to adjust for potential confounding effects of each factor. Factors significant on univariable analysis were included in a multivariable logistic regression model, using backward stepwise logistic regression, to identify factors independent of 28-day mortality. 20 Hazard ratios, along with their corresponding 95% confidence intervals, were calculated. The ability of the m-NUTRIC score to predict 28-day mortality was assessed by calculating the area under the receiver operating characteristic curve (AUC), with AUCs of 0.90–1.00, 0.80–0.90, 0.70–0.80, 0.60–0.70, and 0.50–0.60 considered excellent, good, fair, poor, and unsatisfactory, respectively.21,22 The optimal cutoff values for the m-NUTRIC score and other variables were determined based on the maximum Youden index. 22 The sensitivity (SS), specificity (SP), positive likelihood ratio (PLR), negative likelihood ratio (NLR), positive prediction value (PPV), and negative predictive value (NPV) of the m-NUTRIC score for predicting 28-day mortality were calculated.
All tests were two-tailed, with p-values <0.05 considered statistically significant. All statistical analyses were performed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA) and MedCalc Ver.20.111 (MedCalc Software, Ostend, Belgium) statistical software.
Results
Clinical characteristics and outcomes in the STMV and PAMV groups
Out of the 1746 patients admitted to the respiratory ICU throughout the study period, 464 (26.6%) met the eligibility criteria of the study, as depicted in Figure 1. The baseline characteristics and clinical outcomes of this patient cohort are presented in Table 1. Among these patients, diabetes (n = 146, 31.9%), with or without complications, was the most prevalent underlying condition. The 28-day mortality rate for all enrolled patients reached 26.7% (n = 124).

Flowchart of patient selection.
Demographic and clinical characteristics in patients who received short-term and prolonged acute mechanical ventilation.

Normally distributed continuous variables are reported as mean ± standard deviation, non-normally distributed continuous variables are reported as median (range), and categorical variables are reported as number (%).
Data from 458 patients (short-term mechanical ventilation, n = 128; prolonged acute mechanical ventilation patients, n = 330).
All clinical data were calculated or obtained from medical records on the day of ICU admission.
Total and out-of-pocket medical expenditures for all medical resources used (including all medicines) during hospitalization in the ICU and general ward.
APACHE II, Acute Physiology and Chronic Health Evaluation II; BMI, body mass index; NUTRIC, nutrition risk in critically ill; SOFA, Sequential Organ Failure Assessment; USD, U.S. dollars.
Among the enrolled patients, 132 (28.4%) received STMV, while 332 (71.6%) received PAMV. It is noteworthy that the rates of chronic neurological diseases as comorbidities and tracheostomies at hospital discharge were significantly higher in the PAMV group than in the STMV group. However, the 28-day mortality rate was significantly higher in the STMV group than in the PAMV group, as indicated in Table 1.
The mean m-NUTRIC score for all enrolled patients was 5.3 ± 1.8. There was no significant difference in the mean m-NUTRIC score between the STMV and PAMV groups. However, the m-NUTRIC score was positively correlated with Charlson’s weighted index in total and STMV patients (γ = 0.313, p < 0.001 and γ = 0.195, p = 0.025). Furthermore, in the PAMV group, the m-NUTRIC score was positively correlated with total medical expenditure (γ = 0.138, p = 0.012), ventilator LOS (γ = 0.120, p = 0.029), Charlson’s weighted index (γ = 0.364, p < 0.001), as determined by Pearson’s correlation coefficients.
Comparisons of survivors and non-survivors
A comparison of the demographic and clinical characteristics of survivors and non-survivors revealed that survivors were significantly younger, had a lower m-NUTRIC score, had a higher rate of chronic neurological diseases, and a lower rate of malignant tumors as comorbidities. In addition, survivors had higher total and out-of-pocket medical expenditures and a higher rate of tracheostomy at hospital discharge (Table 2).
Comparison of demographic and clinical characteristics and outcomes between survivors and non-survivors.
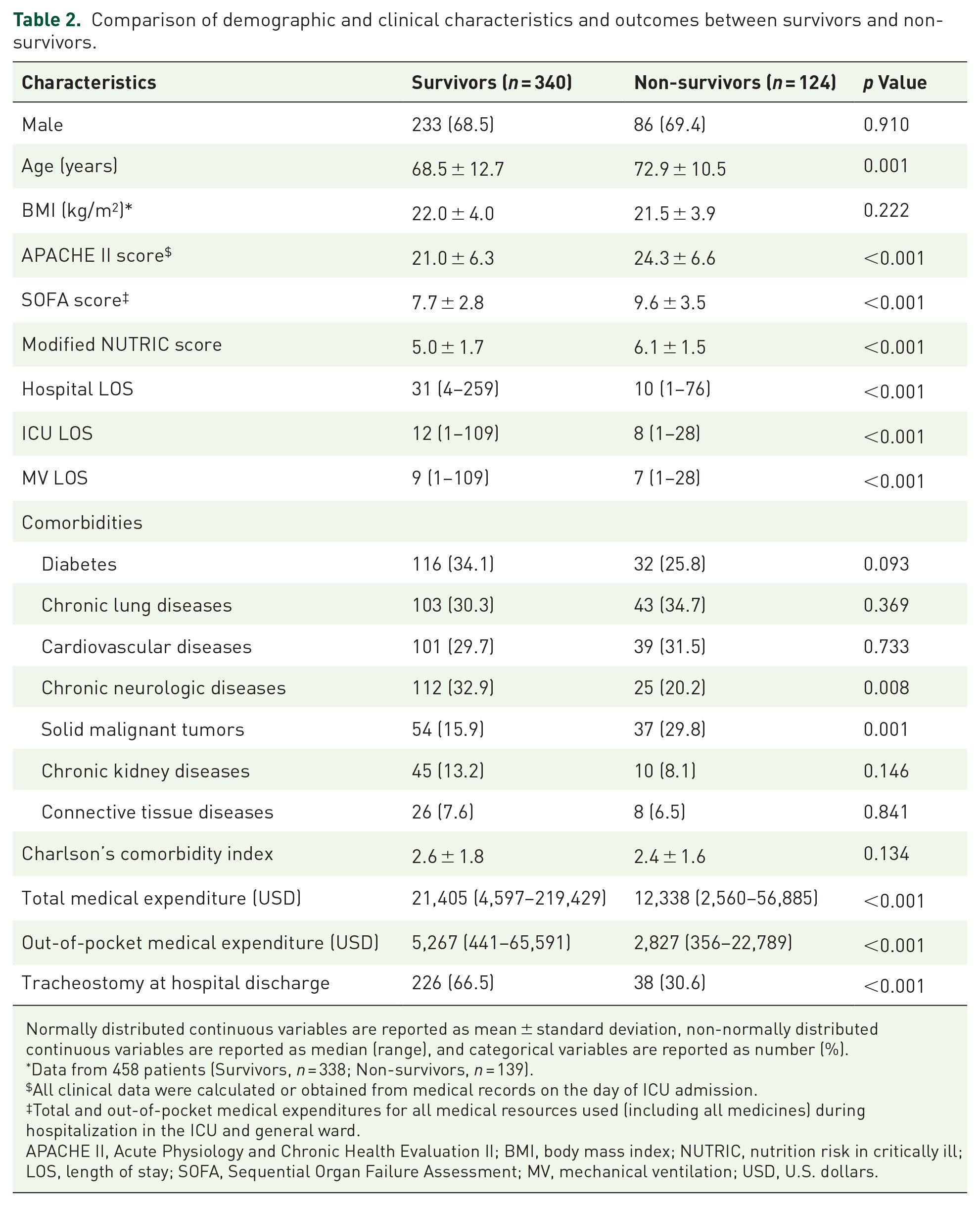
Normally distributed continuous variables are reported as mean ± standard deviation, non-normally distributed continuous variables are reported as median (range), and categorical variables are reported as number (%).
Data from 458 patients (Survivors, n = 338; Non-survivors, n = 139).
All clinical data were calculated or obtained from medical records on the day of ICU admission.
Total and out-of-pocket medical expenditures for all medical resources used (including all medicines) during hospitalization in the ICU and general ward.
APACHE II, Acute Physiology and Chronic Health Evaluation II; BMI, body mass index; NUTRIC, nutrition risk in critically ill; LOS, length of stay; SOFA, Sequential Organ Failure Assessment; MV, mechanical ventilation; USD, U.S. dollars.
Ability of modified NUTRIC score to predict 28-day mortality
An assessment of the ability of the m-NUTRIC score to predict 28-day mortality within the entire cohort of 464 patients revealed an AUC of 0.672 (95% CI, 0.627–0.714). Further investigation indicated that the AUCs for 28-day mortality were 0.819 (95% CI 0.742–0.880) in the STMV group and 0.595 (95% CI, 0.540–0.648) in the PAMV group, as shown in Figure 2(a)–(c). The optimal cutoff value was 5 for total patient, STMV patient, and PAMV patient groups, and the corresponding SS, SP, PLR, NLR, PPV, and NPV are shown in Table 3. Furthermore, patients in these groups with m-NUTRIC scores ⩾ 5 exhibited significantly higher 28-day mortality rates than those with m-NUTRIC scores < 5 (32.8% versus 14.4%, p < 0.001 in total patients; 48.4% versus 10.8%, p < 0.001 in STMV patients; 25.9% versus 15.5%, p = 0.038 in PAMV patients), respectively.
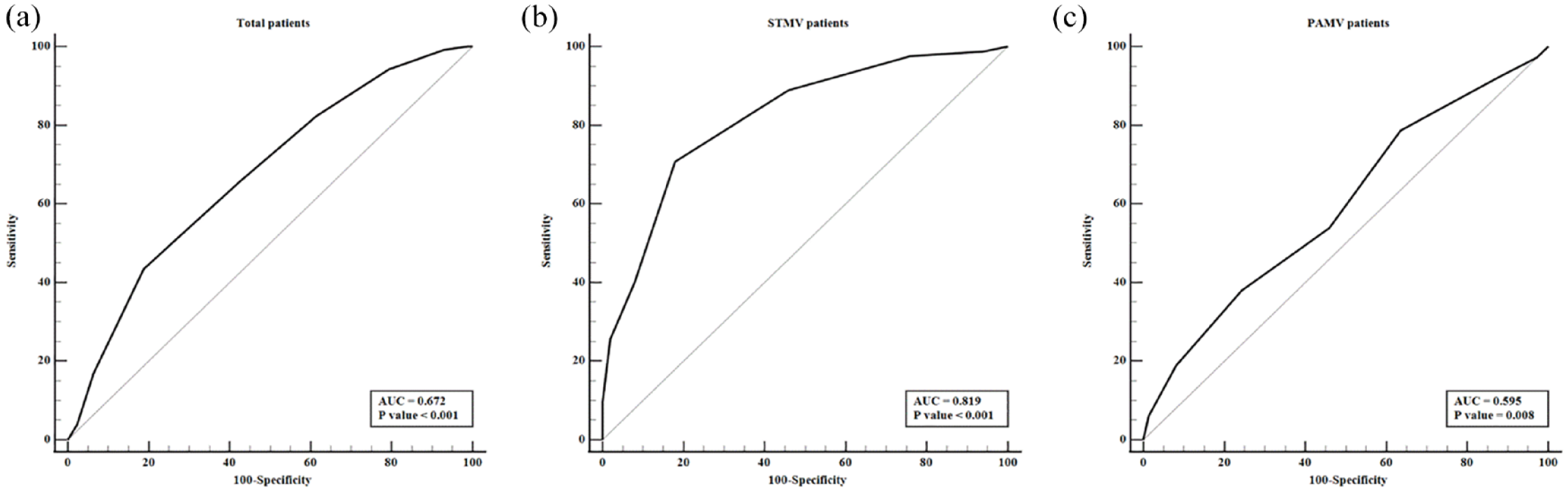
AUCs for the m-NUTRIC score in (a) total patients and patients who received (b) STMV and (c) PAMV. Their AUCs were 0.672 (95% CI: 0.627–0.704; p value <0.001), 0.819 (95% CI: 0.742–0.880; p value <0.001), and 0.595 (95% CI: 0.540–0.48; p-value = 0.001), respectively.
Sensitivity, specificity, and positive and negative predictive values of modified NUTRIC score for predicting patient mortality.
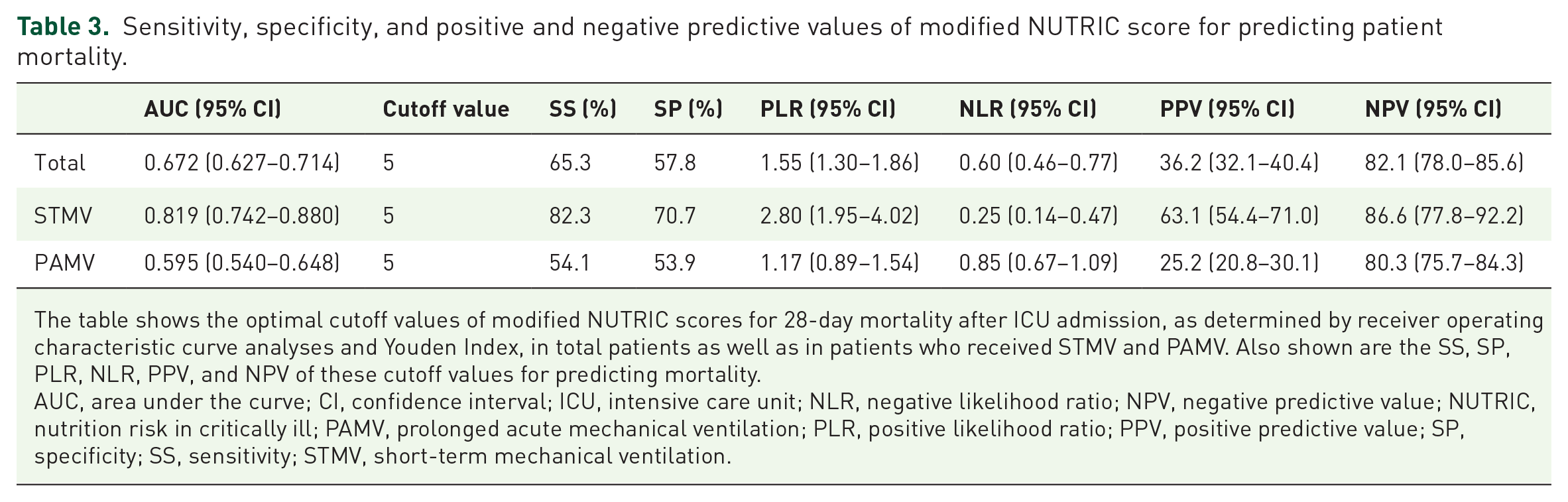
The table shows the optimal cutoff values of modified NUTRIC scores for 28-day mortality after ICU admission, as determined by receiver operating characteristic curve analyses and Youden Index, in total patients as well as in patients who received STMV and PAMV. Also shown are the SS, SP, PLR, NLR, PPV, and NPV of these cutoff values for predicting mortality.
AUC, area under the curve; CI, confidence interval; ICU, intensive care unit; NLR, negative likelihood ratio; NPV, negative predictive value; NUTRIC, nutrition risk in critically ill; PAMV, prolonged acute mechanical ventilation; PLR, positive likelihood ratio; PPV, positive predictive value; SP, specificity; SS, sensitivity; STMV, short-term mechanical ventilation.
Table 4 provides an overview of the factors independently predicting 28-day mortality for total patients, STMV patients, and PAMV patients based on a Cox regression hazard model. An m-NUTRIC score ⩾ 5 was found to be associated with mortality through multivariable Cox regression analysis. The Kaplan–Meier survival estimate at 28 days lends further support to the results of this analysis, as shown in Figure 3. In subgroup analyses, the cutoff value of 5 emerged as a significant prognostic indicator in STMV patients, while not in PAMV patients, as detailed in Table 4.
Univariate and multivariate analyses of factors associated with 28-day mortality in patients who received mechanical ventilation.
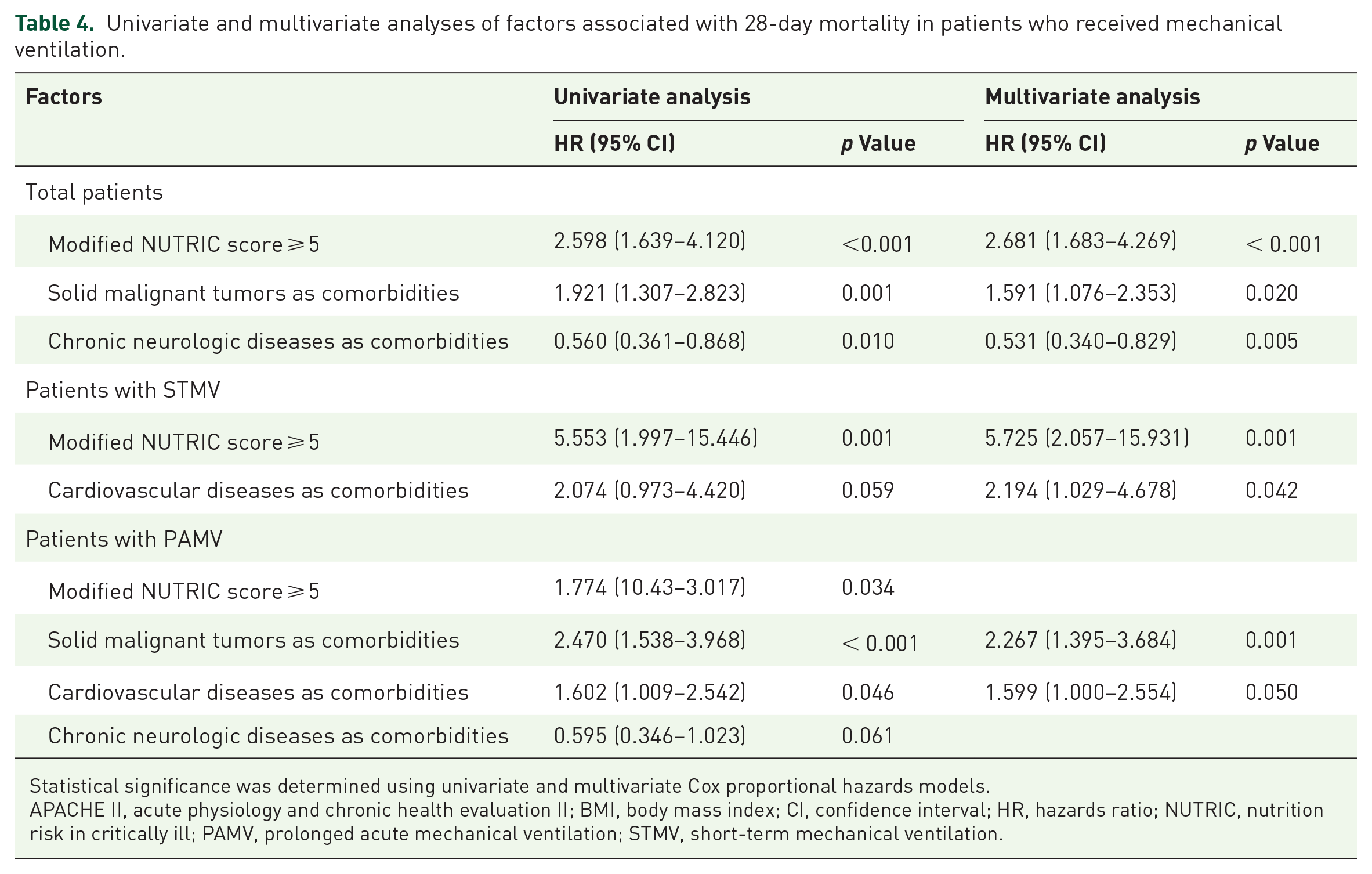
Statistical significance was determined using univariate and multivariate Cox proportional hazards models.
APACHE II, acute physiology and chronic health evaluation II; BMI, body mass index; CI, confidence interval; HR, hazards ratio; NUTRIC, nutrition risk in critically ill; PAMV, prolonged acute mechanical ventilation; STMV, short-term mechanical ventilation.

Kaplan–Meier survival curves for 28-day survival after endotracheal intubation based on m-NUTRIC score ⩾ 5 in total patients.
Discussion
The present study evaluated the prognostic value of m-NUTRIC scores in patients who received MV in the ICU for pneumonia. The AUC analysis of all enrolled patients showed that this score performed poorly in its prediction of a 28-day mortality rate, a finding consistent with previous results.4,5 When divided into STMV and PAMV groups, however, m-NUTRIC scores differed significantly in predicting mortality rate. To our knowledge, this study is the first to analyze the predictive performance of modified NUTRIC score according to the duration of MV in patients requiring invasive ventilator care.
The main strength of this study was that the m-NUTRIC score demonstrated good discriminative ability, as shown by AUC analysis, in predicting 28-day mortality in patients who received STMV. This suggests that this score could be a useful prognostic indicator for predicting 28-day mortality in these patients. Furthermore, patients with cutoff values ⩾5 exhibited elevated 28-day mortality rates. Multivariate analysis revealed that these cutoff values were associated with a high HR for predicting 28-day mortality, which is consistent with the findings of previous reports.5,7,8,23 This m-NUTRIC score is objective and easy to extract, making it easy to use EMRs to inform clinical care. In addition, the 28-day mortality rate was significantly higher in the STMV than in the PAMV group, suggesting that the m-NUTRIC score could help critical care physicians inform patients’ families or surrogates about the likelihood of death within 96 h, despite early intensive treatment in the ICU.
In contrast to findings in the STMV group, AUC analysis showed that the m-NUTRIC score had poor discriminative ability to predict 28-day mortality in the PAMV group. Their cutoff for this score was lower, with multivariate analysis indicating that some underlying comorbidities should also be considered prognostic factors. Although the 28-day mortality rate was lower in the PAMV than in the STMV group, the m-NUTRIC score in the PAMV group was less valuable as a predictive factor. Models that include other various clinical variables and underlying comorbidities would be necessary for predicting mortality.
Previous reports have reported that an m-NUTRIC score cutoff value of ⩾5 predicts a high mortality rate and nutritional status.5,7,8,23 The present study also found that this cutoff value was optimal for predicting 28-day mortality, especially for STMV patients. In contrast to these previous studies, other studies have reported different cutoff values for m-NUTRIC scores for patients who received MV for other conditions,4,6,9 indicating that the cutoff values of m-NUTRIC scores for predicting mortality are dependent on the characteristics of the enrolled populations. Further large-scale studies are necessary to determine the cutoff values in different subgroups of ventilated patients.
Recently, patients receiving PAMV have been categorized as having a ‘chronic critical illness’, with the number of these patients projected to increase over time.24,25 Their long-term mortality rates and medical expenses are high. 24 Various prognostic indicators have been identified, including older age (⩾65 years); underweight (BMI ⩽ 18.5 kg/m2); hemato-oncologic malignancies as comorbidities; the requirement for medical resources such as vasopressors, neuromuscular blockade, and hemodialysis on day 4 of MV; and other clinical variables, such as PaO2/FiO2 < 200 mm Hg, platelet count < 100 × 109/L, albumin < 3.5 g/dL, BUN >7 mmol/L, pH < 7.35, lactic acid > 2.0 mmol/L, and serum sodium ⩾ 145 mmol/L.26–32 Other extraneous factors, including the perspectives of patients’ families or surrogates, physician–family communications, and the utilization of medical resources, could also be considered prognostic indicators. A model that includes these individualized parameters, rather than the m-NUTRIC score alone, may be more predictive of mortality in patients undergoing PAMV.
The present study had several limitations. First, it attempted to evaluate the ability of the m-NUTRIC score to predict mortality in various patient subgroups, including those with sepsis (or septic shock) and those with different demographic characteristics and underlying comorbidities. Significant differences, however, were not observed, possibly due to the small number of enrolled patients. Second, it would have been better to distinguish between STMV patients with severe lung involvement and those with mild/indirect lung involvement. However, due to the retrospective design, it was impossible to separate these patients into separate groups. Third, differences in the number of MV days may result in diverse nutritional requirements. However, due to the retrospective nature of the study, differences in these requirements between STMV and PAMV patient groups could not be precisely examined or compared. Although it is postulated that the m-NUTRIC score can potentially predict these differences, the retrospective design posed challenges in thoroughly investigating this aspect of the study. Fourth, due to the single-center, retrospective design of this study, selection bias may have been introduced and the sample size was not calculated. Finally, although performed at a university-affiliated tertiary care hospital, the present study was performed on patients at a single center. Therefore, the results may not be generalizable to other populations.
Conclusion
In conclusion, this study found that the m-NUTRIC score was more valuable in predicting 28-day mortality in patients who underwent STMV than PAMV. In addition, the cutoff value for predicting mortality was higher than that previously reported. Additional well-designed studies are needed to determine the ability of the m-NUTRIC score to predict 28-day mortality in ICU patients, especially those requiring STMV.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241232263 – Supplemental material for Ability of the modified NUTRIC score to predict mortality in patients requiring short-term versus prolonged acute mechanical ventilation: a retrospective cohort study
Supplemental material, sj-docx-1-tar-10.1177_17534666241232263 for Ability of the modified NUTRIC score to predict mortality in patients requiring short-term versus prolonged acute mechanical ventilation: a retrospective cohort study by Wanho Yoo, Hyojin Jang, Hayoung Seong, Saerom Kim, Soo Han Kim, Eun-Jung Jo, Jung Seop Eom and Kwangha Lee in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.