
Abstract
Background:
Patients who need prolonged mechanical ventilation (MV) have high resource utilization and relatively poor outcomes. The pathophysiologic mechanisms leading to weaning failure in this group may be complex and multifactorial. The aim of this study was to investigate the factors associated with prolonged weaning based on the Weaning Outcome according to a New Definition (WIND) classification.
Methods:
This is a prospective observational study with consecutive adult patients receiving MV for at least two calendar days in medical intensive care units from 1 November 2017 to 30 September 2020. Eligible patients were divided in a non-prolonged weaning group, including short and difficult weaning, and in a prolonged weaning group according to the WIND classification. The risk factors at the time of first separation attempt associated with prolonged weaning were analyzed using a multivariable logistic regression model.
Results:
Of the total 915 eligible patients, 172 (18.8%) patients were classified as prolonged weaning. A higher proportion of the prolonged weaning group had previous histories of endotracheal intubation, chronic lung disease, and hematologic malignancies. When compared with the non-prolonged weaning group, the median duration of MV before the first spontaneous breathing trial (SBT) was longer and the proportion of tracheostomized patients was higher in prolonged weaning group. In addition, the prolonged weaning group used higher peak inspiratory pressures and yielded lower PaO2/FiO2 ratios at the day of the first SBT compared with the non-prolonged weaning group. In multivariate analyses, the duration of MV before first SBT (adjusted odds ratio [OR] = 1.14, 95% confidence interval [CI] = 1.06–1.22, p < 0.001), tracheostomy state (adjusted OR = 1.95, 95% CI = 1.04–3.63, p = 0.036), PaO2/FiO2 ratio (adjusted OR = 1.00, 95% CI = 0.99–1.00, p = 0.023), and need for renal replacement therapy (adjusted OR = 2.68, 95% CI = 1.16–6.19, p = 0.021) were independently associated with prolonged weaning. After the exclusion of patients who underwent tracheostomy before the SBTs, similar results were obtained.
Conclusion:
Longer duration of MV before the first SBT, tracheostomy status, poor oxygenation, and need for renal replacement therapy at the time of first SBT can predict prolonged weaning.
Trial registration:
ClinicalTrials.gov Identifier NCT05134467.
Keywords
Background
Mechanical ventilation (MV) is a commonly used intervention for respiratory support in intensive care units (ICUs). 1 Although advances in critical care have led to improved survival from acute illness, the number of patients requiring prolonged MV after acute respiratory failure is increasing,2,3 thereby leading to increased healthcare costs, morbidity, and mortality.2,4–8 Therefore, it is necessary to make predictions for the patients who will require prolonged MV to inform them, formulate surrogate decision-making, and identify targets for future interventions. Previous studies have sought to identify these predictors; however, their results are difficult to generalize because they examined varying durations of MV 9 and specific patient populations. 10
The definition of prolonged MV has been varied depending on the study, but most studies have been based on the total duration of MV ranging from 1 day to 4 weeks.9,11,12 MV is used in patients with various medical conditions that are not accompanied by impaired pulmonary function such as cardiac arrest, altered mental status, or postoperatively, however. In addition, there may be differences in the timing or technique of the MV separation attempt depending on the hospital’s policy or physician’s practice pattern. 13 Therefore, it may be reasonable to focus on the difficulty or duration of weaning process rather than the entire duration of MV in terms of evaluating MV-related outcomes. The European Respiratory Society Task Force has defined prolonged weaning as the need for the weaning process for >7 days after the first spontaneous breathing trial (SBT), but it has limitations in classifying patients with various settings encountered in real practice, such as tracheostomized patients. 14 Recently, researchers in the Weaning Outcome according to a New Definition (WIND) study suggested a new classification scheme that can overcome these limitations in predicting the prognosis of patients who receive MV.15–17 Therefore, the objective of this prospective cohort study was to evaluate the characteristics of patients who require prolonged MV and to identify predictive factors related to prolonged weaning by the WIND classification in patients admitted to the medical ICU.
Methods
Study population
All consecutive patients admitted to two medical ICUs and those requiring MV for more than 24 h from November 2017 were prospectively registered at Samsung Medical Center (a 1989-bed tertiary referral hospital) in Seoul, South Korea. For this study, we excluded from the analysis those patients who were treated with extracorporeal membrane oxygenation for respiratory support (n = 37), did not undergo SBT before extubation (n = 317), or were withdrawn from MV as palliative care (n = 17). Eligible patients were divided in a non-prolonged weaning group, including short and difficult weaning, and in a prolonged weaning group according to the WIND classification scheme (Figure 1).

Scheme of group distribution.
The institutional review board of the Samsung Medical Center approved this study (IRB no. 2017-08-141-009) and waived the requirement for informed consent because of the observational nature of the research. In addition, patient information was anonymized and de-identified prior to analysis.
Standardized weaning process
Since 2010, the two medical ICUs in our hospital have been using the same standardized weaning programs based on a respiratory care practitioners-driven, protocol-directed approach; the details of the weaning process have been described in our previous studies.5,16,18 Every morning, respiratory care practitioners assessed a patient’s readiness to be weaned from MV in all patients who received MV for more than 24 h. First, we comprehensively evaluated the patient’s condition, including improvement of the underlying cause of respiratory failure, clinical stability, and adequacy of pulmonary function and oxygenation. If the patient fulfilled all of the criteria of readiness for weaning trials (Supplementary Table S1), SBT was conducted according to the protocol to assess the ability of the patient for spontaneous breathing; if the patient did not fulfill the criteria, no further weaning process was performed on that day. Our hospital performed the T-piece trial, in which supplemental oxygen was provided through a T-piece connected to an endotracheal tube or tracheostomy tube, on all patients until July 2019. From July 2019, SBT was performed with inspiratory pressure augmentation (the ventilator was set with a pressure support of 8 cmH2O and zero-positive end-expiratory pressure) for patients who received MV through an endotracheal tube according to the revised weaning protocol. 19 The T-piece trial was conducted for patients with tracheostomy as before. Tolerance for SBT was evaluated for 30 min on the first attempt and for 2 h after the second attempt, regardless of the method used. If a sign of SBT failure was identified even before the target duration, however, the trial was immediately stopped. When the patient satisfied all the criteria for successful SBT (Supplementary Table S2), extubation was performed directly, and supplemental oxygen was provided by a high-flow nasal cannula for at least 24 h in patients with an endotracheal tube; administration of supplemental oxygen was continued through a T-piece system in patients with tracheostomy. Decisions about when and how to perform a tracheostomy were left to the discretion of the clinicians and were not guided by a prescribed algorithm.
Weaning outcomes
Successful weaning was defined as (1) extubation without death or reintubation within the next 7 days irrespective of whether non-invasive ventilation was used postextubation, or whether the patients were discharged from the ICU without invasive MV within 7 days, whichever came first for intubated patients and (2) spontaneous ventilation through tracheostomy without any MV during 7 consecutive days, or discharged with spontaneous breathing, whichever came first in the cases of tracheostomized patients. 15 The date of the successful weaning was counted retrospectively to the actual day of extubation after the patient had completed 7 days without reintubation or was discharged earlier without reintubation.
The weaning outcomes were classified in three categories using the WIND classification 15 : (1) short weaning when the first separation attempt resulted in the termination of the weaning process within a day, (2) difficult weaning when the weaning process was completed after more than 1 day but in less than 1 week after the first separation attempt, and (3) prolonged weaning when the weaning was still not terminated 7 days after the first separation attempt (by successful separation or death), respectively. The weaning process was considered to be terminated if the patient was successfully separated from MV or if the patient died.
Data collection
A trained study coordinator reviewed hospital medical records and obtained clinical, laboratory, and outcome data. Patient demographics and the major reason for MV were assessed by the physician responsible for care and were recorded on the day of the initiation of MV. Details of the patient’s readiness for weaning trials and the methods and results of SBT were recorded in the format specified by the respiratory care practitioners. Patient vital signs – including blood pressure, heart rates, respiratory rates, and transcutaneous oxygen saturation – were continuously monitored and automatically recorded every hour. There was no protocol for the time at which blood gas analysis was performed except at the end of SBT, but arterial blood was usually obtained for blood gas analyses at approximately 5 am every day. The values of the MV setting and respiratory parameters were synchronized to the hospital electronic medical chart and recorded every hour, and we collected the values at 8 am. Patients were followed up until discharge from hospital and clinical outcomes, including weaning success, respiratory status at ICU discharge, ICU length of stay, and hospital mortality, were identified based on a review of the medical records.
Statistical analysis
Data are presented as medians and interquartile ranges (IQRs) for continuous variables and as numbers and percentages for categorical variables. Comparisons of clinical characteristics and weaning outcomes between the prolonged weaning group and non-prolonged weaning group was carried out using the Mann–Whitney U test for continuous variables, and the χ2 or Fisher’s exact test for categorical variables, wherever applicable. To identify risk factors for prolonged weaning, we performed logistic regression analyses. Variables that appeared to be related in the univariate logistic regression analyses with a p-value of <0.1 were considered in multivariate regression models. Because tracheostomy may have been performed in patients with expected prolonged weaning, we performed additional multivariate analysis after the exclusion of tracheostomized patients according to the physician’s judgment. The results of logistic regression models were reported as odds ratios (ORs) of each variable with their 95% confidence intervals (CIs). For all analyses, a two-tailed p-value of <0.05 was considered statistically significant. Statistical analyses were performed using the software STATA (version 16.0, Stata Corporation, College Station, TX, USA).
Results
During the study period, a total of 1286 patients were eligible, but 371 (28.8%) patients were excluded by the exclusion criteria. The final cohort included 915 patients with a median age of 67 (IQR = 57–75) years, and 594 patients (64.9%) were male. According to the WIND classification, 561 (61.3%) patients were classified as short weaning, 182 (19.9%) as difficult weaning, and 172 (18.8%) as prolonged weaning patients (Figure 1).
Baseline characteristics
The clinical details of patients in the non-prolonged and prolonged weaning groups are listed in Table 1. Age, sex, and body mass index were similar between the two groups. Compared with the non-prolonged weaning group, the prolonged weaning group had higher proportions of chronic lung disease (25.0% versus 17.5%, p = 0.031) and hematologic malignancies (26.9% versus 19.2%, p = 0.032), but a lower proportion of dementia (21.5% versus 31.9%, p = 0.007). In both groups, hypoxemic respiratory failure was the most common cause of MV initiation.
Clinical characteristics and outcomes..
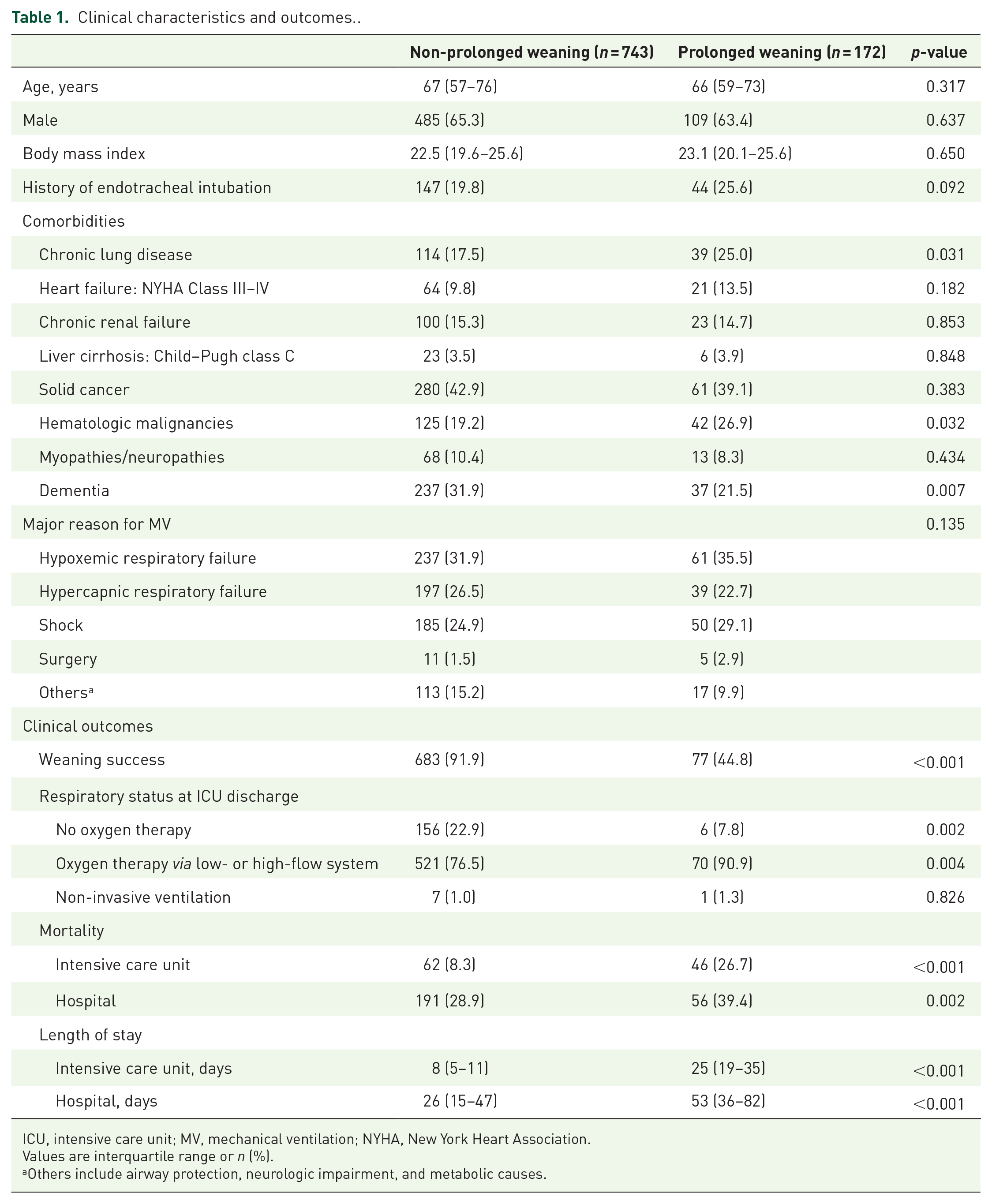
ICU, intensive care unit; MV, mechanical ventilation; NYHA, New York Heart Association.
Values are interquartile range or n (%).
Others include airway protection, neurologic impairment, and metabolic causes.
Characteristics at the day of the first separation attempt
Comparison of clinical characteristics at the day of the first separation attempt is listed in Table 2. The median durations of MV before the first SBT were 5 (3–7) and 7 (4–11) days in the non-prolonged and prolonged weaning groups, respectively (p < 0.001) (Table 2). At the time of the first SBT, the proportion of tracheostomized patients in the prolonged weaning group was higher than in the non-prolonged weaning group (36.6% versus 16.8%, p < 0.001). Before SBT, 89% of the patients were receiving pressure support ventilation. The level of positive end-expiratory pressure was similar in both groups, but peak inspiratory pressure (17 cmH2O versus 16 cmH2O, p = 0.001) and fraction of inspired oxygen (FiO2) (35% versus 30%, p < 0.001) were higher in the prolonged weaning group. The prolonged weaning group not only had a lower ratio of arterial oxygen partial pressure (PaO2) to FiO2 (257 versus 302, p < 0.001), but it also had more severe extrapulmonary organ dysfunction (sequential organ failure assessment score of 6 versus 5, p = 0.024). Furthermore, 15.1% of the studied patients required vasoactive drugs, and 14.8% received renal replacement therapy. Steroids were more frequently used in the prolonged weaning group (52.4% versus 43.1%, p = 0.031).
Clinical and treatment characteristics at the day of first separation attempt.

FiO2, fraction of inspired oxygen; MV, mechanical ventilation; PaCO2, partial pressure of carbon dioxide in arterial blood; PaO2, partial pressure of oxygen in arterial blood; PBW, predicted body weight; PEEP, positive end-expiratory pressure; SaO2, arterial oxygen saturations; SIMV, synchronized intermittent mandatory ventilation; SOFA, sequential organ failure assessment; RASS, Richmond Agitation–Sedation Scale; Vt, tidal volume.
Values are interquartile range or n (%).
Risk factors for prolonged weaning
Univariable logistic regression analysis indicated that 14 variables were associated with prolonged weaning (Table 3). In multivariable analysis, the duration of MV before the first SBT (adjusted odds ratio (aOR) = 1.14, 95% CI = 1.06–1.22, p < 0.001), tracheostomy state (aOR = 1.95, 95% CI = 1.04–3.63, p = 0.036), PaO2/FiO2 ratio (aOR = 1.00, 95% CI = 0.99–1.00, p = 0.023), and use of renal replacement therapy (aOR = 2.68, 95% CI = 1.16–6.19, p = 0.021) continued to be risk factors for prolonged weaning (Table 3). In the subgroup analysis excluding the tracheostomized patients (n = 188, 20.5%), the duration of MV before the first SBT, PaO2/FiO2 ratio, and the use of renal replacement therapy were still significantly associated with prolonged weaning (Table 4).
Predictors of prolonged weaning in patients who received mechanical ventilation.

CI, confidence interval; FiO2, fraction of inspired oxygen; MV, mechanical ventilation; OR, odds ratio; PaO2, partial pressure of oxygen in arterial blood; RASS, Richmond Agitation–Sedation Scale; SOFA, sequential organ failure assessment.
The reference group is endotracheal tube.
The reference group is RASS −1–+1.
Predictors of prolonged weaning in patients who received mechanical ventilation excluding tracheostomized patients.

CI, confidence interval; FiO2, fraction of inspired oxygen; MV, mechanical ventilation; OR, odds ratio; PaO2, partial pressure of oxygen in arterial blood; RASS, Richmond Agitation–Sedation Scale; SOFA, sequential organ failure assessment.
The reference group is RASS −1–+1.
Discussion
This study evaluated the clinical characteristics and outcomes of medical patients with prolonged weaning using the WIND classification and sought for the predictive factors that could be evaluated at the time of the first separation attempt from MV. We found that tracheostomy, a longer duration of MV before the first separation attempt, decreased oxygenation, and the use of renal replacement therapy were associated with increased risks of prolonged weaning. These findings were maintained after the tracheostomized patients were excluded.
Previous studies reported that the proportion of prolonged MV or prolonged weaning among patients receiving MV varied from 5% to 20% depending on the definition used in each study.5,7,8,14–16,20–22 Similarly, in this study, patients classified as prolonged weaning were common and accounted for approximately one-fifth of the patients who attempted separation from MV at least once. The prolonged MV was expected to increase, however, 23 and the proportion of prolonged weaning in patients who received MV in our medical ICUs also increased by 5% compared with the proportion 5 years ago. 16 Therefore, the ability to accurately identify patients who will require prolonged MV would allow clinicians to modify risk factors and improve outcomes.
We identified four patient characteristics related to prolonged weaning, one of which was the PaO2/FiO2 ratio. The PaO2/FiO2 ratio is a major parameter that represents lung function of oxygenation, which could be associated with the duration of MV in patients with acute respiratory distress syndrome. 24 It has not been found to be an independent risk factor for prolonged weaning or prolonged MV in the previous studies, however. 10 Contrary to other studies that showed that acidosis and hypercapnia are predictors of prolonged weaning,25,26 no significant differences were found between the prolonged and non-prolonged weaning groups in this study. These rather intriguing findings could be attributed to the different timings of assessment between this study – which conducted evaluations at the time of recovery when MV separation was being attempted – and other studies, which conducted evaluations at the time of initiation of MV or at ICU admission. 10
Second, the MV duration before the first separation attempt was associated with prolonged weaning. Because respiratory care practitioners evaluated every patient’s readiness for SBT on a daily basis according to the standard protocol in our hospital, prolonged periods from the initiation of MV to the first separation attempt may have been affected by delayed resolution of the major cause of MV support. In addition, prolonged MV before first separation attempt may lead to the increased risk of several adverse events such as ventilator-induced lung injury and ventilator-induced diaphragmatic dysfunction, which may adversely affect successful weaning from MV.27,28
Third, renal failure requiring renal replacement therapy was associated with prolonged weaning. The interaction between lung and kidney is well known. Hypoxemia or hypercapnia in various lung diseases can cause kidney injury, and renal dysfunction can lead to the deterioration of lung function by causing lung edema or lung inflammation, thereby creating a vicious cycle. 29 In addition, acid–base imbalance accompanying renal dysfunction may increase the effort required for breathing for the compensation of metabolic acidosis, and adequate renal compensation may not be achieved for hypercapnia that occurs in lung disease.30,31 Reflecting the lung–kidney cross-talk, several studies have also indicated that renal dysfunction is a risk factor for prolonged weaning.25,32,33
Finally, we found that tracheostomy status at the first separation attempt was also associated with prolonged weaning. Tracheostomy is often considered in patients perceived to be difficult to wean. 34 In this study, although we could not obtain data on the cause of tracheostomy, tracheostomy was considered when the patients were expected to need artificial airways, such as for insufficient ability to clear secretion or for prolonged MV. Kollef et al. 35 showed that the duration of MV was longer in patients who underwent tracheostomy at the physician’s discretion compared with patients who did not receive a tracheostomy, suggesting that physicians have the ability to select patients for whom prolonged weaning can be predicted. Therefore, we analyzed the subgroup after the exclusion of tracheostomized patients to confirm risk factors for prolonged weaning; however, the remaining three factors were still significantly associated with an increased risk of prolonged weaning.
This study has contributed to the research on predictive factors associated with an increased risk of prolonged weaning using the WIND classification; however, there are several limitations that should be acknowledged. First, the significance of our findings might have been influenced by the inherent selection bias of this observational study. The data were collected prospectively from all the consecutive patients who had been admitted to the medical ICU from patients who were on MV support for more than 24 h and who were screened daily for weaning readiness based on the standardized weaning protocol, however. Although patients were primarily managed by attending physicians with responsibility for patient care, the weaning process and general care in the ICU were provided based on the institutional protocols and general guidelines. In addition, we used multivariable regression model to control for potential confounders. The possible existence of bias owing to unmeasured risk factors remains, however. Second, this study was conducted at a single institution with a protocol-based weaning program, which may limit the generalizability of our findings to other centers in which no specific programs are available for weaning. Third, tracheostomy was performed in one-fifth of patients, which is higher than the rates (11–15%) in an international multicenter study 36 and may improve aspects of care of patients on MV. 37 Subgroup analysis (excluding the tracheostomized patients) revealed that the remaining three factors were associated with increased risks of prolonged weaning, however.
In conclusion, longer duration of MV before weaning trials, tracheostomy status, poor oxygenation, and need for renal replacement therapy at the time of the first separation attempt of MV could be predictive for prolonged weaning. Further studies should be conducted to identify risk factors for prolonged weaning in patients with various respiratory pathophysiologies and extrapulmonary medical conditions to establish treatment strategies to improve the clinical outcomes and reduce the socioeconomic burden of prolonged weaning, however.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221117005 – Supplemental material for Factors associated with prolonged weaning from mechanical ventilation in medical patients
Supplemental material, sj-docx-1-tar-10.1177_17534666221117005 for Factors associated with prolonged weaning from mechanical ventilation in medical patients by Soo Jin Na, Ryoung-Eun Ko, Jimyoung Nam, Myeong Gyun Ko and Kyeongman Jeon in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.