
Abstract
Objective
In this multicenter retrospective study, we evaluated the prognostic role of blood eosinophil count on clinical outcomes in hospitalized patients with exacerbations of chronic obstructive pulmonary disease (COPD).
Methods
We included patients aged 20 to 90 years with a COPD diagnosis. Patients were divided into groups with blood eosinophil count ≤300 or >300 cells/μL and then further classified into 1–99, 100–300, or >300 cells/μL. We compared sociodemographic features and clinical outcomes between groups and identified risk factors associated with mortality in hospitalized patients with COPD and blood eosinophil count ≤300 cells/μL.
Results
In total, 217 patients were included (82% men, average age 64.3±10.3 years). Patients with eosinophil counts ≤300 cells/μL had significantly longer hospital stays, more admissions to the intensive care unit (22.2% vs. 4.3%), and more frequent mechanical ventilation (21.6% vs. 4.3%) than those with eosinophil counts >300 cells/μL. Mortality only occurred in the group with ≤300 cells/μL; patients with COPD who had eosinophil counts >300 cells/μL had significantly better survival rates (17.0% vs. 0%).
Conclusion
High blood eosinophil counts at admission were associated with improved short-term outcomes. Our findings reveal the importance of considering eosinophil counts in clinical decision-making to manage hospitalized patients with COPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease that is characterized by progressive airflow obstruction. 1 Acute exacerbations of COPD involve acute deteriorations in airway function and respiratory symptoms, which may require hospitalization. 2 Frequent episodes of COPD exacerbation are associated with rapid disease progression and increased mortality. 3
COPD is a major public health challenge in low-income countries. 4 A recent meta-analysis revealed that over three-quarters of global COPD cases occur in low and middle-income countries. 5 Syria is estimated to have the highest prevalence of COPD among Middle Eastern countries.6,7 Nevertheless, a recent cross-sectional study demonstrated low awareness of COPD and a high prevalence of its risk factors within the Syrian population. 8 Despite these concerning figures, there is a notable lack of research on COPD in Syria, specifically studies focusing on the characteristics and outcomes of hospitalized patients with COPD.
Blood eosinophils have gained attention as a prognostic factor among hospitalized patients with COPD exacerbations. 9 Several studies have linked higher blood eosinophil counts to a better prognosis, including shorter hospital stays.10,11 Furthermore, patients with lower blood eosinophil counts experience higher rates of intensive care unit (ICU) admission and an increased need for mechanical ventilation compared with patients who have higher blood eosinophil counts.12–14 In contrast, multiple studies have shown no difference in ICU admissions or the need for mechanical ventilation between patients with lower and higher blood eosinophil counts.15,16
Regarding mortality among hospitalized patients with COPD, studies have reported higher mortality rates among patients with COPD who have lower blood eosinophil counts9,17 whereas other studies have found no significant differences in mortality rates between these groups.15,18 Recent studies indicate that patients with COPD and an eosinophilic inflammation phenotype tend to experience more frequent exacerbations and higher rates of hospital readmission in comparison with patients who have a non-eosinophilic inflammation phenotype.19,20 However, recent clinical trials have shown that high blood eosinophil counts are associated with a better response to inhaled corticosteroids (ICS), which can help prevent further exacerbations. 21 Smoking, however, may interfere with this beneficial response by reducing eosinophil counts in the small airways. 22 This reduction in intraepithelial eosinophils among smokers could diminish the effectiveness of therapy with ICS, thereby impacting its ability to control exacerbations in patients with COPD.
Blood eosinophils have become a useful biomarker for the management of acute exacerbations in patients with COPD. These patients are categorized into two clinical phenotypes: those with an eosinophilic exacerbating phenotype and those with a predominantly neutrophilic, non-eosinophilic phenotype. This classification helps in identifying specific molecular targets for new therapies. For instance, in phase III clinical trials, the use of monoclonal antibodies such as mepolizumab (an anti-interleukin [IL]-5 monoclonal antibody) and dupilumab (an anti-IL-13 and IL-4 monoclonal antibody) has shown promising results for patients with COPD and an eosinophilic exacerbating phenotype. These trials demonstrate a reduction in the incidence of exacerbations, improved lung function, enhanced health status, and fewer severe respiratory symptoms compared with placebo. 23 Furthermore, a recent randomized clinical trial from the United Kingdom found that using blood eosinophils as a biomarker to guide prednisolone therapy at the time of an acute COPD exacerbation does not increase the rate of treatment failure and can safely reduce systemic glucocorticoid use. 24
Considering these inconsistencies, we conducted a retrospective multicenter study to evaluate the prognostic role of blood eosinophil counts at admission in hospitalized patients with COPD exacerbations. In this observational study, we aimed to determine whether patients with COPD and lower blood eosinophil levels at admission 1) experience a longer length of hospital stay, 2) have a greater risk of requiring mechanical ventilation and ICU admission, and 3) exhibit higher mortality rates compared with patients in the higher eosinophilic group.
Methods
Study design, setting, and participants
We conducted a retrospective observational multicenter study between 1 June and 30 June 2023 at Damascus Hospital (Al-Mujtahid) and Al-Mouwasat Hospital. Damascus Hospital is affiliated with the Syrian Ministry of Health and Al-Mouwasat Hospital is affiliated with the Syrian Ministry of Higher Education and Scientific Research. Both hospitals are public university hospitals serving major areas of the capital, Damascus. We used a convenience sampling strategy; during the study period, all patients with acute COPD exacerbation admitted to the hospital and meeting the inclusion criteria were enrolled in the study (Figure 1). Each patient was followed for 1 month after admission to track survival or death. Follow-ups were conducted via telephone calls, text messages, or emails using the contact details provided by each patient or their relatives. Data were collected from the hospitals’ medical records. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 25
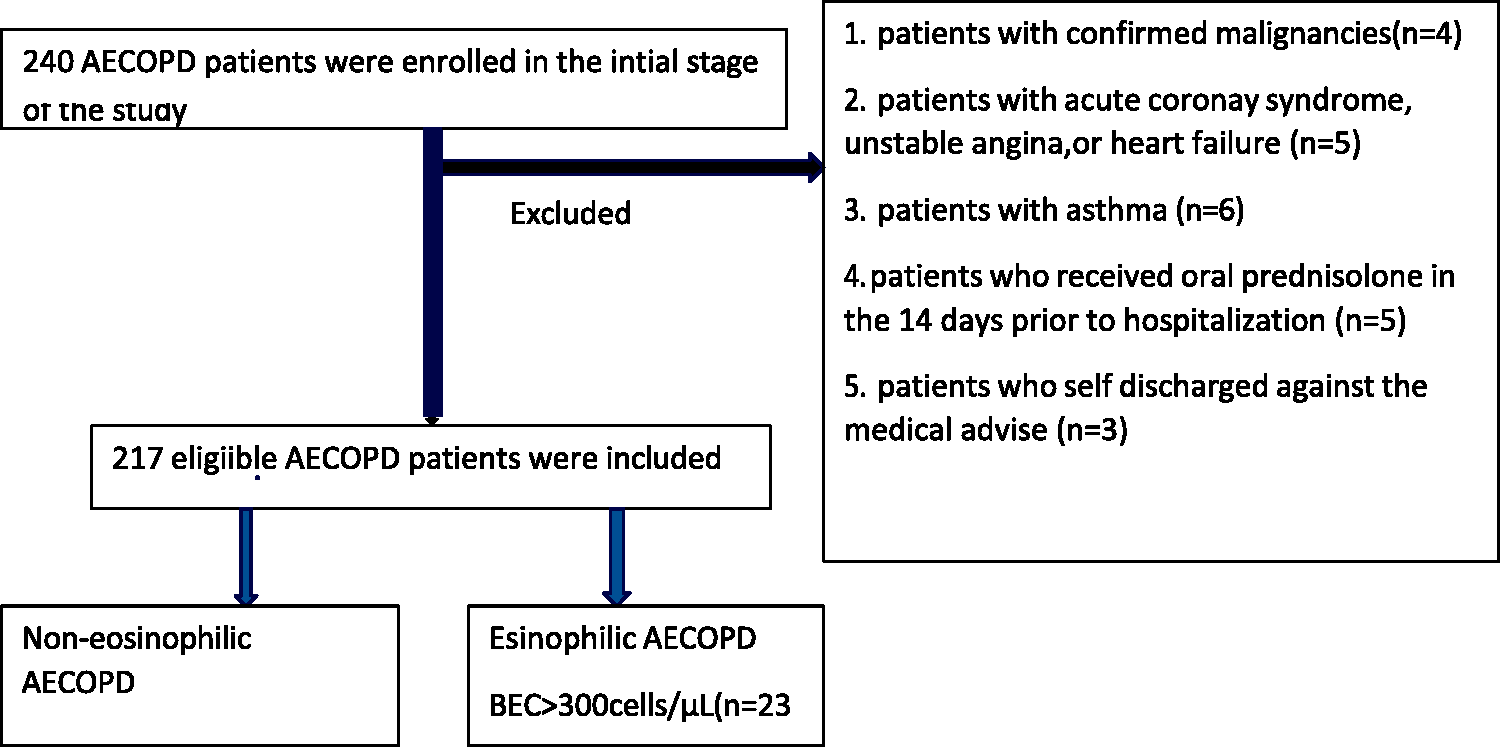
Flowchart of hospitalized patients with chronic obstructive pulmonary disease (COPD) and exacerbations in this study
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2013. Ethical approval was granted by the Institutional Review Board (IRB) at the Syrian Private University (SPU) on 29 October 2022. The IRB at SPU did not provide us with an approval number/ID. All participant data were de-identified by the investigators to ensure patient confidentiality and compliance with the Declaration of Helsinki. All participants or their legally authorized representative provided their written consent by answering a yes/no question. Participation in the study was voluntary. Participants or their legally authorized representatives were assured that they had the right to decide whether to participate in the study and that there were no repercussions if they decided to withdraw after providing their consent. All information collected in the study was kept strictly confidential.
Inclusion criteria
Patients meeting the following criteria were included in the study: 1) a confirmed diagnosis of COPD, as indicated by a post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity ratio of <70%, 2) hospitalized owing to COPD exacerbations, and 3) between the ages of 20 and 90 years.
Exclusion criteria
Patients were excluded from the study if they had confirmed malignancies. Additionally, we excluded patients if their acute ICU admission was related to a cardiac event, including heart failure, unstable angina, or acute coronary syndrome, as confirmed by a cardiologist. We also did not include patients with a history of asthma or those being treated for asthma at the time of clinical evaluation. Moreover, we excluded patients who received oral prednisolone in the 14 days prior to hospitalization for an acute exacerbation of COPD to eliminate cases of chronic exacerbations. To identify these conditions, the authors reviewed participants’ medical histories and X-ray findings. We also excluded patients who missed their outpatient follow-up owing to being self-discharged from the hospital against medical advice (Figure 1).
Data collection
The authors reviewed all participants’ clinical records, laboratory results, and X-ray findings. In cases where data from the files were incomplete, the authors contacted the patients via telephone. The data collected included sociodemographic characteristics such as age, sex, body mass index (BMI), and smoking history; the presence of comorbidities including hypertension, diabetes, and ischemic heart diseases; and laboratory results such as blood eosinophil counts, hemoglobin, creatinine, D-dimer, and FEV1 percent predicted on admission. Additional data included the presence of acidosis on admission and a history of previous hospital admissions owing to COPD exacerbation in the past year. Treatment regimens covering bronchodilators, antibiotics, and corticosteroids were also included. Additionally, clinical outcomes, including the length of hospital stay, need for admission to the intensive care unit, mechanical ventilation (both invasive and non-invasive), full recovery, or death were also recorded.
Two investigators independently verified the data collection process to ensure accuracy. Initially, patients were categorized into two groups based on their blood eosinophil counts. The first group comprised patients with a blood eosinophil count >300 cells/μL, and the second group included those with a blood eosinophil count ≤300 cells/μL. For a more detailed analysis, we further divided patients into three groups: those with a blood eosinophil counts between 1 and 99 cells/μL, patients with a count between 100 and 300 cells/μL, and those with counts >300 cells/μL.
Study definitions
Acute exacerbation of COPD (AECOPD) was defined as sustained worsening of a patient’s symptoms from their usual state beyond typical day-to-day variations. This includes increased cough, breathlessness, and sputum production over the previous 48 hours. 2 Acute respiratory acidosis was diagnosed using blood gas findings, defined as a partial pressure of carbon dioxide (PCO2) greater than 45 mmHg, a bicarbonate level exceeding 30 mEq/L, and a pH below 7.35. Typically, the bicarbonate level increases by 1 mEq/L for each 10 mmHg increase in PCO2 soon after admission. 26 The severity of airflow limitation was classified using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria upon patient admission. 27 The GOLD criteria classify COPD severity using post-bronchodilator FEV1 as a percentage of the predicted value, as follows: mild (stage 1): FEV1 ≥80% of predicted; moderate (stage 2): FEV1 50% to 79% of predicted; severe (stage 3): FEV1 30% to 49% of predicted; very severe (stage 4): FEV1 <30% of predicted. Mechanical ventilation was defined as the use of any form of non-invasive or invasive mechanical ventilation support during hospitalization. Noninvasive mechanical ventilation was defined as the application of ventilatory support through an external interface, such as a face mask, which delivers oxygen and facilitates carbon dioxide removal without invasive procedures. Invasive mechanical ventilation involves the insertion of an endotracheal tube through the patient's mouth or nose into the trachea. 28 The length of hospital stay was defined as the total number of days a patient remains hospitalized, from admission to discharge. The mortality rate was defined as the occurrence of death either during the hospital stay or within 1 month after discharge.
Statistical analysis
Categorical variables are presented as frequency and percentage (descriptive statistics); continuous variables are presented as mean with standard deviation (SD) for Gaussian-distributed data and as median with interquartile range for non-normally distributed data. The independent samples t-test was used to compare the means of Gaussian-distributed continuous variables, and the Mann–Whitney U test was applied for variables that were not normally distributed. The chi-square test and Fisher’s exact test were used to compare categorical outcomes against sociodemographic characteristics, treatment regimens, and clinical outcomes such as length of hospital stay, need for ICU admission, use of mechanical ventilation, and mortality between patients with COPD and blood eosinophil counts >300 cells/μL and those with counts ≤300 cells/μL. Multivariable logistic regression was used to detect factors associated with mortality among patients with blood eosinophil counts ≤300 cells/μL. Selected factors included sex (male vs. female), comorbidities (hypertension vs. no hypertension, diabetes vs. no diabetes, ischemic heart disease vs. no ischemic heart disease, obesity vs. no obesity), smoking history (positive smoking history vs. negative smoking history), presence of acute respiratory acidosis on admission (present vs. absent), severity of airflow limitation based on GOLD criteria (very severe vs. other), and history of two or more previous hospital admissions for COPD exacerbations in the past year (present vs. absent). All statistical analyses were conducted using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA), with a p-value <0.05 considered statistically significant.
Results
Sociodemographic features and treatment regimens related to blood eosinophilic counts in hospitalized patients with COPD exacerbations
A total of 217 patients with COPD exacerbations were enrolled in this study, with mean age 64.3 years (SD 10.3). There were 178 men (82.0%) in the cohort and 39 women (18.0%). A total of 212 (97.7%) patients were current or former smokers. The overall mean blood eosinophil count for the 217 patients with COPD was 115.9 cells/μL (SD 118.4). Among them, 194 patients with a blood eosinophil count ≤300 cells/μL had a mean count of 80.9 cells/μL (SD 59.0); the 23 patients with a blood eosinophil count >300 cells/μL had a mean count of 411.3 cells/μL (SD 70.7). Patients with a blood eosinophil count ≤300 cells/μL more frequently had a positive smoking history compared with those who had a blood eosinophil count >300 cells/μL (99.0% vs. 87.0%, χ2 = 13.181, p < .001). Furthermore, patients with COPD and a blood eosinophil count ≤300 cells/μL were more likely to be current smokers than those with counts >300 cells/μL (85.6% vs. 78.3%, χ2 = 13.360, p = 0.001). The average BMI for all hospitalized patients with COPD was 24.5 kg/m2, with no significant difference between patients with blood eosinophil counts >300 cells/μL and those with counts ≤300 cells/μL (24.4 kg/m2 vs. 24.7 kg/m2). Patients with COPD and a blood eosinophil count >300 cells/μL were more likely to be overweight (34.8% vs. 32.5%, χ2 = 0.50) and obese (13.0% vs. 10.3%, χ2 = 0.162) compared with those who had a blood eosinophil count ≤300 cells/μL; however, these differences were not statistically significant. Hypertension was the most common comorbidity, diagnosed in 71 (32%) participants. Patients with COPD who had a blood eosinophil count ≤300 cells/μL exhibited a higher prevalence of hypertension compared with those having higher eosinophil counts (34.0% vs. 21.7%, χ2 = 1.409). Of the 217 hospitalized patients with COPD included in the study, 114 (52%) had no hospital admissions owing to COPD exacerbations in the previous year. The prevalence of no previous admissions was similar between groups, with 52.2% in the eosinophilic COPD exacerbation group and 52.6% in the non-eosinophilic COPD exacerbation group (χ2 = 0.180). Furthermore, patients with COPD and a blood eosinophil count ≤300 cells/μL demonstrated a higher prevalence of two or more previous hospital admissions for COPD exacerbations compared with patients with COPD and a blood eosinophil count >300 cells/μL, but the difference was not statistically significant (24.7% vs. 21.7%, χ2 = 0.180).
Regarding laboratory results and clinical investigation upon admission, the mean FEV1% predicted for the entire cohort was 49.1 (SD 15.1). Patients with COPD and a blood eosinophil count >300 cells/μL demonstrated a higher FEV1% predicted than patients with COPD who had a blood eosinophil count ≤300 cells/μL (51.6, SD 19.2 vs. 48.8, SD 14.6). As for COPD stages, patients with COPD and a blood eosinophil count >300 cells/μL demonstrated a higher prevalence of mild airflow limitation (GOLD stage 1) compared with those having counts ≤300 cells/μL (13.0% vs. 9.8%, χ2 = 0.481). Conversely, patients with a blood eosinophil count ≤300 cells/μL exhibited a higher prevalence of very severe airflow limitation (GOLD stage 4) compared with patients with a blood eosinophil count >300 cells/μL (16.0% vs. 13.0%, χ2 = 0.481). Upon admission, 49 (25.3%) patients with COPD and a blood eosinophil count ≤300 cells/μL were diagnosed with acute respiratory acidosis whereas only two patients (8.7%) with a blood eosinophil count >300 cells/μL were diagnosed with this condition (χ2 = 3.137). Regarding treatment regimens, 194 (89.4%), 190 (87.6%), and 133 (61.3%) patients were treated with bronchodilators, antibiotics, and corticosteroids, respectively. Patients with a blood eosinophil count ≤300 cells/μL were more likely to be treated with antibiotics compared with patients having a blood eosinophil count >300 cells/μL (91.8% vs. 52.2%, χ2 = 29.566, p < 0.001). Among patients with a blood eosinophil count ≤300 cells/μL, 174 (89.7%) received bronchodilators, compared with 20 (87.0%) patients with a blood eosinophil count ≥300 cells/μL, with no statistical significance (χ2 = 0.162). Additionally, corticosteroid treatment was administered to 119 (61.3%) patients with blood eosinophil count ≤300 cells/μL and to 14 patients (60.9%) in the ≥300 cells/μL group (χ2 = 0.002) (Table 1).
Sociodemographic features and treatment regimens of hospitalized patients with COPD and blood eosinophil counts ≤300 cells/μL and ≥300 cells/μL.

COPD, chronic obstructive pulmonary disease; BMI, body mass index; FEV1, forced expiratory volume in 1 second; GOLD: Global Initiative for Chronic Obstructive Lung Disease; SD, standard deviation; IQR, interquartile range.
Impact of eosinophil counts on length of hospital stay and clinical outcomes in hospitalized patients with COPD exacerbations
The mean length of stay in the hospital for all hospitalized patients with COPD was 5.5 days (SD 3.0). Additionally, the median length of hospital stay for all patients was 5 days, with an interquartile range of 5 days and a range from 1 to 13 days.
Patients with a blood eosinophil count >300 cells/μL were more likely to have a shorter hospital stay of only 1 day compared with those having counts ≤300 cells/μL (26.1% vs. 7.2%, χ2 = 8.868, p = 0.012). In contrast, 130 patients (67.0%) with a blood eosinophil count ≤300 cells/μL were hospitalized for a longer duration, ranging from 2 days to 1 week, compared with 13 patients (56.6%) with a blood eosinophil count >300 cells/μL (χ2 = 8.868, p = 0.012). Furthermore, 50 patients (25.8%) with blood eosinophil count ≤300 cells/μL remained in the hospital for more than 1 week, versus 4 patients (17.4%) with a blood eosinophil count >300 cells/μL (χ2 = 8.868, p = 0.012).
Regarding the clinical outcomes of hospitalized patients with COPD exacerbations, 44 patients (20.3%) among the total cohort were admitted to the ICU, and 43 patients (19.8%) required mechanical ventilation. Thirty-three patients (15.2%) died.
The clinical outcomes also showed significant disparities between both groups. Patients with a blood eosinophil count ≤300 cells/μL were more likely to require ICU admission than patients with counts >300 cells/μL (2.2% vs. 4.3%, χ2 = 4.038, p = 0.04). Additionally, patients with a blood eosinophil count ≤300 cells/μL were more likely to require mechanical ventilation (21.6%) than those with a blood eosinophil count >300 cells/μ (4.3%) (χ2 = 3.874, p = 0.04). Moreover, patients with blood eosinophil count ≤300 cells/μL had a greater likelihood of death resulting from COPD exacerbation (17.0%) compared with patients with blood eosinophil counts >300 cells/μL (0.0%) (χ2 = 4.614, p = 0.03) (Table 2).
Length of hospital stay and clinical outcomes of hospitalized patients with COPD and blood eosinophil counts ≤300 cells/μL and ≥300 cells/μL.

COPD, chronic obstructive pulmonary disease; SD, standard deviation.
Distribution of blood eosinophil counts in relation to clinical outcomes of hospitalized patients with COPD exacerbations
Patients were divided into three groups based on their blood eosinophil count: 1 to 99 cells/μL, 100 to 300 cells/μL, and >300 cells/μL, representing 78.3%, 11.1%, and 10.6% of the study sample, respectively. Among patients admitted to the ICU, 39 (88.6%) had a blood eosinophil count between 1 and 99 cells/μL, four patients (9.1%) had a blood eosinophil count between 100 and 300 cells/μL, and one patient (2.3%) had a blood eosinophil count >300 cells/μL. Similarly, among those requiring mechanical ventilation, 38 patients (88.4%) had a blood eosinophil count between 1 and 99 cells/μL, four (9.3%) had a blood eosinophil count between 100 and 300 cells/μL, and one patient (2.3%) had a blood eosinophil count >300 cells/μL. In terms of mortality, 31 patients (93.9%) who died had a blood eosinophil count between 1 and 99 cells/μL and two patients (6.1%) who died had a blood eosinophil count between 100 and 300 cells/μL; no patients died who had a blood eosinophil count >300 cells/μL. Hence, patients with a blood eosinophil count between 1 and 99 cells/μL exhibited a higher proportion of ICU admissions, a greater need for mechanical ventilation, and a higher mortality rate in comparison with the two other groups (Figure 2, Supplementary Table 1).

Clinical outcomes of hospitalized patients with chronic obstructive pulmonary disease (COPD) and blood eosinophil counts 1–99 cells/μL, 100–300 cells/μL, or >300 cells/μL.
Multivariate logistic regression analysis of factors associated with mortality among hospitalized patients with COPD and eosinophil count ≤300 cells/μL
Multiple logistic regression analysis revealed that acute respiratory acidosis at admission (odds ratio [OR] = 6.979, p = 0.02) and very severe COPD according to the GOLD criteria at admission (OR = 52.879, p < 0.001) were associated with an increased risk of mortality among hospitalized patients with COPD and a blood eosinophil count ≤300 cells/μL. However, having a history of two or more previous hospital admissions (OR = 2.997) and a smoking history (OR = 1.256) were not statistically significant (Table 3).
Multivariate logistic regression analysis of factors associated with mortality among hospitalized patients with COPD and eosinophil counts ≤300 cells/μL.

COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; CI, confidence interval.
Discussion
In this retrospective multicenter observational study, we determined that hospitalized patients with COPD and blood eosinophil count ≤300 cells/μL had a worse short-term prognosis. These patients experienced more severe exacerbations and were more likely to require antibiotics compared with patients having a blood eosinophil count ≥300 cells/μL (91.8% vs. 52.2%, χ2 = 29.566, p < 0.001). This may explain patients’ poor prognosis and weak response to systemic corticosteroids. A previous review in The Lancet highlighted different phenotypes of COPD exacerbations and emphasized the role of eosinophil counts in therapy guidance. 29 Infection is more probable in patients with low eosinophil counts and severe exacerbations.30,31 In these cases, antibiotics are necessary whereas corticosteroids are less effective, although their use is still recommended.32,33 Furthermore, 61.3% of patients with a blood eosinophil count ≤300 cells/μL in our study received corticosteroid treatment, which might have contributed to their worse outcomes. The inappropriate use of corticosteroids in these patients might not effectively address the underlying infectious etiology of exacerbations, leading to inadequate control of exacerbations and higher complication rates. 34 Additionally, corticosteroids may aggravate other comorbid conditions, such as diabetes mellitus, which may worsen the overall prognosis of hospitalized patients with COPD. 35 However, in our study, the decision to use antibiotics and systemic corticosteroids was made by respiratory physicians based on their clinical judgment.
Our findings showed that a blood eosinophil count ≥300 cells/μL was associated with a shorter hospital stay (χ2 = 8.868, p = 0.012). This was consistent with previous studies.11,17,36,37 In a post-hoc analysis, randomized clinical trials have demonstrated a strong association between higher eosinophil counts and a positive response to corticosteroids. 38 These findings suggest that higher eosinophil counts might indicate a steroid-responsive phenotype, which might lead to quicker resolution of exacerbations and shorter hospital stays. Additionally, hospitalized patients with COPD and a blood eosinophil count ≤300 cells/μL were more likely to require ICU admission than patients with a blood eosinophil count ≥300 cells/μL (22.2% vs. 4.3%, χ2 = 4.038, p = 0.04). The former patients also had a greater requirement for mechanical ventilation (21.6% vs. 4.3%, χ2 = 3.874, p = 0.04). A cohort multicenter study in China found that non-eosinophilic AECOPD was associated with higher rates of invasive mechanical ventilation and longer hospital stays. 39 Another study in the Republic of Korea revealed that patients with eosinophil counts >300 cells/μL had lower rates of ICU admission. 12 A retrospective study in Denmark found that the eosinophilic group had less need for non-invasive ventilation. 37 These findings suggest that non-eosinophilic patients tend to have more severe exacerbations, likely owing to weaker pulmonary function and considerable airway restriction. 40 These patients often exhibit more severe clinical symptoms and a higher inflammation index. 41
Another significant finding was that no patients with a blood eosinophil count ≥300 cells/μL died in our study, compared with patients having counts ≤300 cells/μL (χ2 = 4.614, p = 0.03). This was consistent with previous studies.14,42–44 More specifically, lower eosinophil counts were associated with worse outcomes: 93.9% of hospitalized patients with COPD who died had a blood eosinophil count between 1 and 99 cells/μL. A prospective multicenter study in Greece observed that patients with low (<50 cells/μL) blood eosinophil levels during admission had a higher risk of 30-day and 1-year mortality than those with higher levels. 17 In contrast, a meta-analysis found no significant difference regarding in-hospital mortality between groups with eosinophilic and non-eosinophilic COPD exacerbations. However, that study noted that patients in the eosinophilic group experienced better outcomes, including shorter hospital stays and improved pulmonary function, compared with patients in the non-eosinophilic group. 45 Our multivariable logistic regression indicated a statistically significant association between being diagnosed with acute respiratory acidosis on admission and an increased risk of death among hospitalized patients with COPD who had a blood eosinophil count ≤300 cells/μL (OR = 6.979, p = 0.02). In a comprehensive audit from 13 European countries, it was reported that the presence of acidotic respiratory failure is a risk factor for in-hospital mortality among these patients. 46 The high mortality linked to severely impaired respiratory function in COPD has long been recognized.47,48 Although respiratory acidosis is a modifiable condition that can often be effectively managed with non-invasive mechanical ventilation, the decision to use non-invasive mechanical ventilation is typically dependent on the physician's discretion. In this study, GOLD stage 4, representing very severe respiratory airflow limitation, was associated with an increased risk of death in hospitalized patients with COPD and a blood eosinophil count ≤300 cells/μL (OR = 52.879, p < 0.001). A recent review showed that patients with COPD who had low blood eosinophil counts, particularly <100 cells/μL, and those with GOLD stage 4, exhibit greater disease progression and higher mortality rates.49,50 Another systematic review highlighted similar findings, identifying disease-specific severity markers like FEV1 and GOLD stage 4 as strong predictors of short-term mortality among hospitalized patients with COPD. 50 The higher mortality in patients with GOLD stage 4 stems from frequent and severe exacerbations along with substantial functional impairments, severe symptoms, and a high risk of acute episodes. These factors lead to more profound and recurrent effects on patients’ health, escalating the likelihood of mortality. 51
This study has several limitations. First, the retrospective nature of the study means that unmeasured confounding factors may have influenced the results. Second, the relatively short follow-up period prevented us from exploring long-term outcomes. Furthermore, we did not include CRP measurements, which are essential in explaining the etiology of exacerbations. These factors should be considered when interpreting the results because they may influence the study conclusions.
Conclusion
The findings of this study supported the observation that patients with COPD and eosinophil counts ≤300 cells/μL have poor outcomes of COPD exacerbations, including an increased need for mechanical ventilation and ICU admission and a higher mortality rate. Therefore, our findings further validate the use of blood eosinophil counts upon admission as a prognostic biomarker for hospitalized patients with COPD. Longer follow-up studies are highly recommended to investigate the long-term prognosis of blood eosinophils in patients with COPD.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241299943 - Supplemental material for Impact of blood eosinophil count on clinical outcomes in hospitalized Syrian patients with COPD exacerbation
Supplemental material, sj-pdf-1-imr-10.1177_03000605241299943 for Impact of blood eosinophil count on clinical outcomes in hospitalized Syrian patients with COPD exacerbation by Sara Albuaini, Michel Najjar, Dania Tulaiba and Hussam Al Bardan in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank Marianne Maghamez for proofreading this research study.
Authors’ contributions
SA and MN conceptualized the study, participated in the design, performed the statistical analysis, interpreted the results, performed a literature search, drafted the manuscript, and revised the final draft of the paper. DT participated in data collection and data coding. HB participated in the study design and conceptualized the study. All authors read and approved the final draft.
Data availability
The datasets supporting the conclusions of this study are included within the article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.