
Abstract
Objectives
The efficacy of omega-3 fatty acids in the treatment of sepsis is controversial. We conducted an updated meta-analysis to clarify the efficacy of omega-3 fatty acids in patients with sepsis.
Methods
PubMed, EMBASE, and the Cochrane Library were searched for randomized clinical trials (RCTs) on omega-3 fatty acid supplementation in adults with sepsis.
Results
Twenty eligible RCTs involving 1514 patients were included in the meta-analysis. Omega-3 fatty acid supplementation was linked to reductions of mortality (I2 = 0, relative risk [RR] = 0.82, 95% confidence interval [CI] = 0.69–0.97), the duration of mechanical ventilation (DMV; I2 = 74%, weighted mean difference [WMD] = −2.20, 95% CI = −4.00 to −0.40), and intensive care unit (ICU) length of stay (LOS; I2 = 91%, WMD = −3.86, 95% CI = −5.72 to −2.01). Subgroup analysis illustrated that mortality was significantly reduced in patients with sepsis and gastrointestinal dysfunction (RR = 0.5, 95% CI = 0.29–0.86, I2 = 0).
Conclusion
Omega-3 fatty acid supplementation might be associated with reduced mortality in patients with sepsis, especially those with gastrointestinal dysfunction. Furthermore, omega-3 fatty acid administration could shorten DMV and ICU LOS.
Keywords
Introduction
Sepsis describes critical organ dysfunction that is caused by an uncontrolled host response to infection. 1 Despite advances in basic sciences and clinical treatment, the mortality rate of sepsis remains at 28% to 40%, and sepsis is a leading cause of death in the intensive care unit (ICU). 2 New alternative treatments must be developed to increase the survival rate of patients with sepsis. Recently, some reviews suggested that re-establishing the intestinal microenvironment and targeting the microbiota might effectively address sepsis.3–5 Omega-3 fatty acids including eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and α-linolenic acid, which have been revealed to improve critical conditions by modulating the composition of the intestinal microbiota, increasing the production of pro-resolving mediators and anti-inflammatory factors, inhibiting nuclear factor receptor (NF-κB) activation, and altering membrane lipid rafts.6–10 Thus, omega-3 fatty acids may benefit patients with sepsis by altering the gut microbiome and increasing the production of anti-inflammatory mediators.
Although multiple randomized clinical trials attempted to explore the efficacy of supplementation with omega-3 fatty acids in patients with sepsis, the results were not consistent.11–30 A previous meta-analysis 31 of 17 studies suggested that supplementation with omega-3 fatty acids did not reduce sepsis-related mortality, whereas another meta-analysis 32 of 12 studies demonstrated that parenteral supplementation with omega-3 fatty acids reduced mortality in patients with sepsis. Therefore, by incorporating the data on patients with sepsis, we conducted an updated meta-analysis to clarify the effects of omega-3 fatty acids on morality, the duration of mechanical ventilation (DMV), and ICU length of stay (LOS). Furthermore, we investigated whether with the association between omega-3 fatty acid supplementation and mortality was linked with the stage of sepsis, which was not addressed by previous meta-analyses.
Materials and methods
The present meta-analysis was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. We did not register our study with PROSPERO, but we will do so in future studies.
Search strategy
We attempted to identify all published studies exploring the efficacy of omega-3 fatty acid supplementation in patients with sepsis. We searched for all relevant trials in the Cochrane Library, EMBASE, and PubMed databases published through 30 September 2019. The search strategies are detailed in Appendices 1–3. We also meticulously checked the references of related systematic reviews to avoid missing other eligible studies.
Study selection
The eligibility of studies was first assessed independently by two authors by reading titles and abstracts. Then, the same two authors further evaluated the eligible studies by reading the full text. Any disagreement concerning eligibility was resolved by comparing notes. The inclusion criteria were as follows: (1) randomized clinical trials (RCTs); (2) adult patients diagnosed with sepsis or septic shock; (3) the intervention groups received omega-3 fatty acids (parenteral or enteral route) alone or in combination with other nutritional components; and (4) the evaluated outcomes were mortality (primary outcome), DMV, and ICU LOS (secondary outcomes). The exclusion criteria were as follows: (1) studies other than RCTs; (2) patients without sepsis or septic shock; (3) insufficient data; and (4) relevant outcomes were not reported. No language limitation was applied.
Data extraction
Two investigators independently extracted related data from eligible studies, and any dispute was resolved via discussion. The extracted information included author, publication year, country, sample size, the route of administration, details about the administration, and pertinent outcomes.
Assessment of risk of bias
Two investigators independently employed the Cochrane Collaboration tool to evaluate each study for risk of bias. 33
Statistical analysis
The RevMan software package (version 5.3.5, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) was used for all statistical analyses. Dichotomous outcomes were expressed as the relative risk (RR), and continuous outcomes were expressed as the weighted mean difference (WMD). Both variables were reported with 95% confidence intervals (CIs). We calculated the standard deviation (SD) using the formula recommended by the Cochrane Collaboration 34 when the value was not directly reported in a study. We also combined low-dose and high-dose intervention groups from one clinical trial into a single omega-3 fatty acid intervention group by following the formula provided in the Cochrane Handbook 34 to calculate the combined means and SDs of pertinent outcomes. The heterogeneity of the included studies was evaluated using the chi-squared test and I2 statistic. 35 I2 > 50% or P < 0.05 indicated homogeneity among the studies, and a random-effects model was used for the analysis. I2 ≤ 50% or P ≥ 0.05 indicated that there was no homogeneity among the studies, and a fixed-effects model was used for the analysis. To clarify the stability of the results and identify potential sources of heterogeneity, sensitivity analysis was conducted. In addition, publication bias for mortality was evaluated using funnel plots. Differences were considered statistically significant at P < 0.05.
Results
Search results
Our search strategies yielded 232 potentially relevant articles from PubMed (82), EMBASE (79), the Cochrane Library (65), and other sources (6). After eliminating duplicates, 172 studies remained. Further reading of titles and abstracts eliminated another 138 studies. The remaining 34 studies were subjected to a full-text assessment, and 14 more studies were excluded for various reasons as explained in Figure 1. Eventually, 20 RCTs involving 1514 patients with sepsis were included in the meta-analysis.

Flow diagram of article selection for meta-analysis.
Features of the included studies
The 20 RCTs 11–30 were published from 1995 to 2018. They were conducted principally in Asia (China, Turkey, Japan), North America (USA), South America (Brazil), Europe (Spain, Romania, Portugal, Switzerland, United Kingdom), and Africa (Egypt). The study populations were patients diagnosed with sepsis, early sepsis, abdominal sepsis, severe sepsis or septic shock, sepsis with acute lung injury (ALI) or acute respiratory distress syndrome (ARDS), and sepsis with gastrointestinal dysfunction. Eight studies11,12,14,19,21,23,27,30 used the enteral route for omega-3 fatty acid supplementation, and the other 12 studies13,15–18,20,22,24–26,28,29 employed the parenteral route. The risk of bias assessment is presented in Figure 2 and Figure 3. The main details of the 20 eligible studies are summarized in Table 1.

Risk of bias assessment of all included studies.

Risk of bias assessment of each individual study.
Characteristics of the included randomized controlled trials.
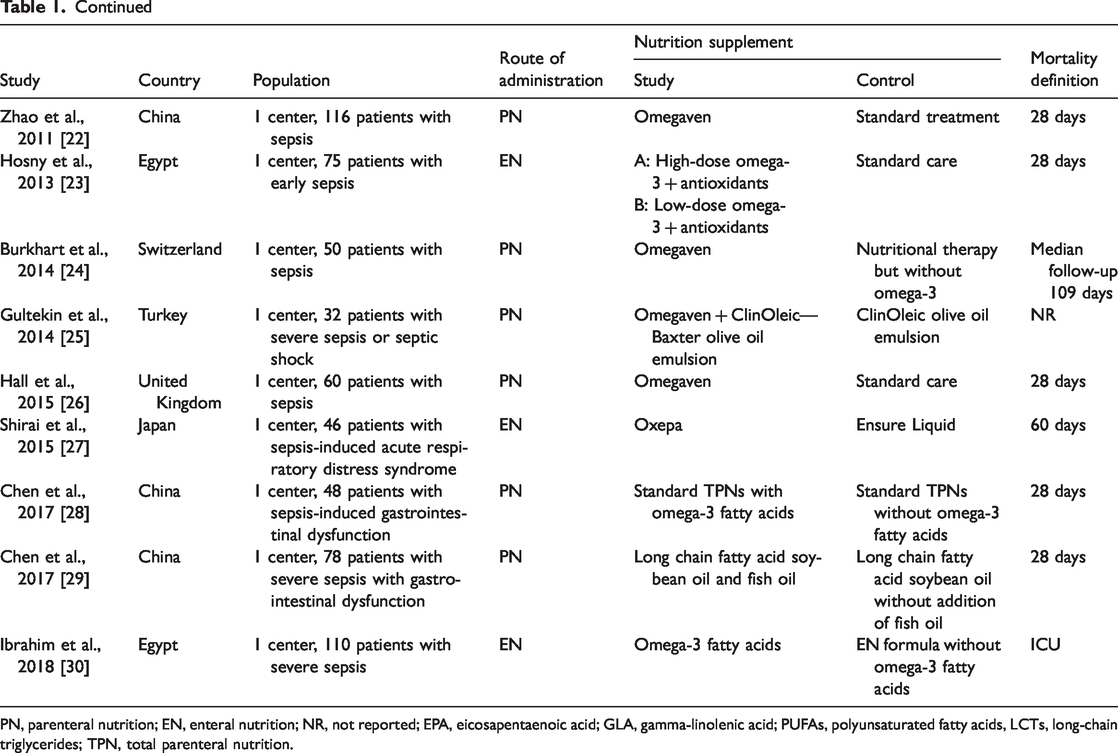
PN, parenteral nutrition; EN, enteral nutrition; NR, not reported; EPA, eicosapentaenoic acid; GLA, gamma-linolenic acid; PUFAs, polyunsaturated fatty acids, LCTs, long-chain triglycerides; TPN, total parenteral nutrition.
Primary outcome: mortality
The mortality analysis covered the aforementioned 20 studies11–30 involving 1514 patients. No heterogeneity was detected among the trials (I2 = 0%, P = 0.56). Therefore, we used a fixed-effects model for the analysis. The results indicated that omega-3 fatty acid supplementation could lower mortality in patients with sepsis (RR = 0.82, 95% CI = 0.69 to 0.97, P = 0.02, Figure 4).

Forest plot of mortality.
Secondary outcomes: DMV and ICU LOS
Effects of omega-3 fatty acids on DMV
Eight eligible12,13,17,19,21,23,27,30 studies reported DMV as an outcome. Significant heterogeneity was detected among the trials (I2 = 74%, P = 0.0003), and thus, we used a random-effects model for the analysis. The results demonstrated that supplementation with omega-3 fatty acids reduced DMV (WMD = −2.20, 95% CI = −4.00 to −0.40, P = 0.02, Figure 5). To identify possible sources of heterogeneity, sensitivity analysis was performed. After excluding trials17,19,21,23,27 that did not report SDs directly, no heterogeneity was detected among the remaining trials (I2 = 0%, P = 0.41). In addition, the effect of omega-3 fatty acids on DMV was altered after excluding the aforementioned studies (WMD = −1.29, 95% CI = −2.76 to 0.18, P = 0.09, Appendix 4). Thus, the result should be accepted with some caution.

Forest plot of the duration of mechanical ventilation.
Effects of omega-3 fatty acids on ICU LOS
Fifteen eligible studies12,13,15,17–24,26–28,30 investigated the effects of omega-3 fatty acids on ICU LOS. Significant heterogeneity was found across the studies (I2 = 91%, P < 0.00001), and we used a random-effects model for the analysis. The results suggested that supplementation with omega-3 fatty acids decreased ICU LOS in patients with sepsis (WMD = −3.86, 95% CI =−5.72 to −2.0, P < 0.0001, Figure 6). Sensitivity analysis was performed to identify the possible sources of heterogeneity. After eliminating several studies,13,15,18,20,21,27 heterogeneity decreased among the remaining studies (I2 = 40%, P = 0.1), and the conclusion was not altered (WMD = −2.63, 95% CI = −3.86 to −1.40, P < 0.0001, Appendix 5).

Forest plot of the intensive care unit length of stay.
Subgroup analysis
We conducted a subgroup analysis to explore whether the stages of sepsis were associated with the effects of omega-3 fatty acid supplementation on mortality in various subgroups. In this study, nine trials11,12,15–18,22,24,26 enrolled patients diagnosed with sepsis, two trials21,23 enrolled patients diagnosed with early sepsis, four trials14,21,25,30 involved patients diagnosed with severe sepsis or septic shock, two trials19,27 included patients diagnosed with sepsis and ALI or ARDS, and in three trials,13,28,29 patients with sepsis also presented with gastrointestinal dysfunction. Mortality was significantly reduced in patients with sepsis and gastrointestinal dysfunction (RR = 0.5, 95% CI = 0.29 to 0.86, P = 0.01, I2 = 0, Appendix 6). The result suggested that omega-3 fatty acid supplementation might benefit patients with sepsis and gastrointestinal dysfunction.
Publication bias
The funnel plots indicated that there was no conspicuous publication bias in the meta-analysis (Appendix 7).
Discussion
Twenty eligible RCTs involving 1514 patients were included in this meta-analysis. The results revealed that supplementation with omega-3 fatty acids might be associated with reduced mortality and shortened DMV and ICU LOS in patients with septic. Nonetheless, these results were impaired by heterogeneity. Caution should be exercised when interpreting our findings.
Concerning mortality, a previous meta-analysis 31 of 17 studies indicated that supplementation with omega-3 fatty acid did not reduce mortality in patients with sepsis. However, our meta-analysis suggested otherwise. An important difference was that three newly published studies were included in our meta-analysis. Additionally, two newly added studies enrolled patients with sepsis and gastrointestinal dysfunction. Furthermore, the studies in our meta-analysis included patients with various stages of sepsis. The subgroup analysis indicated that omega-3 fatty acids might act as positive modulators in patients with sepsis and gastrointestinal dysfunction. Hence, the effects of omega-3 fatty acid supplementation on mortality in patients with sepsis could vary by the stage of sepsis, and patients with sepsis tend to have several complications.
A previous meta-analysis 32 covering 12 RCTs indicated that parenteral supplementation with omega-3 fatty acids did not significantly shorten DMV in patients with sepsis. The discrepancy between their findings and our data might be ascribed to the exclusion of RCTs in which omega-3 fatty acids were supplied enterally. However, additional nutrients, such as anti-oxidant vitamins and amino acids (arginine or glutamine), were supplemented with omega-3 fatty acids via the enteral route, whereas concerning parenteral supplementation, only omega-3 fatty acids were given. The addition of other nutrients may have affected the results.
Our meta-analysis, which included 15 RCTs, indicated that supplementation with omega-3 fatty acids could decrease ICU LOS in patients with sepsis, contradicting a previous meta-analysis 36 involving 11 studies. Because the heterogeneity was high among our included studies, more trials are needed to further support our findings.
Several mechanisms might explain the beneficial effects of omega-3 fatty acids on sepsis. Presumably, critical illness may well disturb the intestinal microenvironment, thereby upsetting the balance among intestinal flora and further leading to immunosuppression and other undesired consequences in patients with sepsis. 4 A recent study 37 demonstrated that the gut microbiome could alter the immunophenotype and survival rate of septic mice and might serve as a therapeutic target for sepsis. In addition, Watson et al. 6 demonstrated that omega-3 fatty acid supplementation could induce a reversible increase in the counts of bacteria that produce short-chain fatty acids, such as Bifidobacterium, Lactobacillus, and Roseburia. Additionally, an animal study by Kaliannan et al. 38 revealed that omega-3 fatty acid supplementation in mice could decrease the counts lipopolysaccharide-producing bacteria (enterobacteria) and increase those of lipopolysaccharide-suppressing bacteria (Bifidobacterium), thereby altering the gut microbiota and alleviating endotoxemia. Thus, omega-3 fatty acids might act as positive modulators in patients with sepsis by altering the gut microbiome and increasing the production of anti-inflammatory mediators, such as short-chain fatty acids. Moreover, omega-3 fatty acids could affect inflammation by increasing the production of anti-inflammatory factors and pro-resolving mediators as well as inhibiting the activation of NF-κB.39,40
In fact, the target organ of omega-3 fatty acid treatment remains unclear. Previous studies in schoolchildren with asthma revealed improved lung function after the administration of omega-3 fatty acids.41,42 Another meta-analysis involving 17 trials indicated that omega-3 fatty acids reduced joint pain, the duration of morning stiffness, and the dosage of nonsteroidal anti-inflammatory drugs in patients with rheumatoid arthritis. 43 Additionally, several studies yielded inconsistent results regarding the role of omega-3 fatty acids in inflammatory bowel disease.44,45 Our subgroup analysis demonstrated that omega-3 fatty acids might act as positive modulators in patients with sepsis and gastrointestinal dysfunction. Future efforts should be directed at identifying the target organs of omega-3 fatty acids.
Some factors such as the dose of omega-3 fatty acids, the proportions of n-3 and n-6 fatty acids, and the proportions of EPA and DHA might alter the effects of omega-3 fatty acids in patients with sepsis. The major studies included in the current meta-analysis used an omega-3 fatty acid dose of 0.2 g/kg/day, and previous studies illustrated that high-dose omega-3 fatty acids in patients with sepsis appear safe, and they may have a key role in treatment. 23 The proportions of EPA and DHA in the included studied ranged 0.86 to 2.3 g/day, and the different proportions may affect the evaluation of efficacy. Previous studies indicated that ratios of 1:2 to 1:4 might be optimal for n-3 and n-6 fatty acids to reduce inflammation. 46 Currently, high-quality trials with a large number of patients with sepsis are needed to further explore the optimal dosage and components of omega-3 fatty acids to improve patient outcomes.
Our meta-analysis had several limitations. First, the patients included in our meta-analysis had various stages of sepsis, and the patient background should be considered when evaluating the efficacy of omega-3 fatty acids. Second, the high heterogeneity in the ICU LOS and DMV analyses could affect the interpretation of treatment efficacy. Third, although most RCTs administered a placebo solution to the control group, two RCTs23,26 provided control groups with only standard sepsis care. One strength of this meta-analysis consisted was that it included more eligible studies than previous meta-analyses. To our knowledge, the present study is the largest meta-analysis to systemically examine the efficacy of omega-3 fatty acid supplementation in patients with sepsis. Additionally, no obvious publication bias was found in our analysis.
Conclusions
Omega-3 fatty acid supplementation might be associated with reduced mortality in patients with sepsis, especially those with gastrointestinal dysfunction. Furthermore, the administration of omega-3 fatty acids appeared to shorten DMV and ICU LOS. High-quality trials with a large number of patients with sepsis are needed to further support our findings. Future studies should further identify the organs targeted by omega-3 fatty acids.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520953684 - Supplemental material for Omega-3 fatty acid supplementation is associated with favorable outcomes in patients with sepsis: an updated meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_0300060520953684 for Omega-3 fatty acid supplementation is associated with favorable outcomes in patients with sepsis: an updated meta-analysis by Chenyang Wang, Dong Han, Xiaojing Feng and Jing Wu in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.