
Abstract
Background:
Numerous randomized controlled trials (RCTs) have reported the benefits of external diaphragm pacing combined with conventional rehabilitation therapies (EDP-CRTs) on pulmonary function and exercise capacity in patients with chronic obstructive pulmonary disease (COPD). However, evidence-based regarding its effects remains unclear.
Objectives:
This systematic review and meta-analysis aimed to evaluate the effects of EDP-CRTs versus CRTs on patients with COPD.
Design:
Systematic review and meta-analysis.
Data sources and methods:
We performed a systematic review and meta-analysis, searching PubMed, Embase, Cochrane Central Register of Controlled Trials, Scopus, China Biology Medicine Disc, Chinese National Knowledge Infrastructure, Wan-Fang Database, and Chinese Scientific Journal Database from inception to 10 September 2023. RCTs investigating the effects of EDP-CRTs versus CRTs on COPD patients were included. The primary outcome was pulmonary function, including forced expiratory volume in 1 s (FEV1), the percentage of predicted values of FEV1 (FEV1%pred), and FEV1/forced vital capacity (FVC)%. Secondary outcomes included arterial blood gas analysis [the partial pressure of arterial oxygen (PaO2) and the partial pressure of arterial carbon dioxide (PaCO2)]; dyspnea [modified Medical Research Council Dyspnea Scale (mMRC)]; exercise capacity [6-min walking distance (6MWD)]; and quality of life [COPD assessment test (CAT)]. RevMan 5.3 software was used for meta-analysis. The quality of the included studies was assessed using the revised Cochrane Risk of Bias tool for randomized trials (RoB 2.0). The certainty of the evidence was evaluated with the Grading of Recommendations Assessment, Development, and Evaluation system.
Results:
In total, 13 studies/981 participants were included. The pooled results revealed significant benefits of EDP-CRTs versus CRTs on the FEV1 [standardized mean difference (SMD) = 1.07, 95% confidence interval (CI) = 0.58–1.56], FEV1%pred [weighted mean difference (WMD) = 6.67, 95% CI = 5.69–7.64], the FEV1/FVC% (SMD = 1.24, 95% CI = 0.48–2.00), PaO2 (SMD = 1.29, 95% CI = 0.74–1.84), PaCO2 (SMD = −1.88, 95% CI = −2.71 to −1.04), mMRC (WMD = −0.55, 95% CI = −0.65 to −0.45), 6MWD (SMD = 1.63, 95% CI = 0.85–2.42), and CAT (WMD = −1.75, 95% CI = −3.16 to −0.35), respectively. Planned subgroup analysis suggested that EDP-CRTs had a better effect on FEV1, FEV1/FVC%, 6MWD, and CAT in the duration of 2–4 weeks.
Conclusion:
EDP-CRTs have better effects on pulmonary function, PaCO2, dyspnea, exercise capacity, and quality of life in COPD patients than CRTs, and the duration to achieve the most effective treatment is 2–4 weeks.
Trial registration:
This systematic review and meta-analysis protocol was prospectively registered with PROSPERO (No. CRD42022355964).
Keywords
Introduction
Currently, chronic obstructive pulmonary disease (COPD) is a global public health disease that seriously affects people from all countries, socioeconomic classes, and age groups. 1 COPD is a heterogeneous lung condition characterized by chronic respiratory symptoms due to abnormalities of the airways and/or alveoli that cause persistent, often progressive, airflow obstruction. 2 COPD not only affects the airways, alveoli, and pulmonary vessels but also has many extrapulmonary adverse effects, 3 among which diaphragm dysfunction is one of the prominent clinical manifestations and is present at all stages of COPD development. 4 Diaphragmatic dysfunction mainly manifests as diaphragmatic atrophy, decreased muscle tone, and reduced muscle endurance, 5 which can cause impaired respiratory function, limited exercise capacity, and decreased quality of life in COPD patients.6,7 Briefly, diaphragm dysfunction directly affects the functional rehabilitation of COPD patients and interact with each other.
For rehabilitation of diaphragm function, many conventional rehabilitation therapies (CRTs) such as diaphragmatic breathing, and diaphragm-related manual therapy, are used to improve diaphragm dysfunction of COPD patients. 8 Nevertheless, limited by the specific physiological structure location and the pathological changes that predispose the diaphragm to fatigue, some CRTs find it hard to stimulate the diaphragm directly and to engage COPD patients actively and consistently in pulmonary rehabilitation training. 9 As a complement to CRTs, diaphragm electrical stimulation has been used in recent years as an emerging and promising treatment for diaphragmatic dysfunction that can effectively improve the therapeutic effect of COPD patients, which includes internal diaphragm pacing (IDP) and external diaphragm pacing (EDP). 8 IDP necessitates an invasive operation with several potential risks, for example, the phrenic nerve can be damaged by surgery or chemical stimulation, so it is rarely used clinically. Contrary to IDP, EDP stimulates the phrenic nerve via surface electrodes, causing the diaphragm to contract, and it is simple to perform, safe, non-invasive, and easily accepted by patients (Figure 1). 10 Based on the current literature review of EDP combined with CRTs (EDP-CRTs) in COPD, data from numerous randomized controlled trials (RCTs) suggest the effectiveness of EDP-CRTs versus CRTs, which can improve diaphragmatic dysfunction, pulmonary ventilation, exercise capacity, and dyspnea in patients with COPD.11,12 However, evidence-based regarding its effects remains unclear. Furthermore, to our knowledge, no meta-analysis to quantitatively evaluate the clinical outcomes of EDP-CRTs in patients with COPD has been published to date.
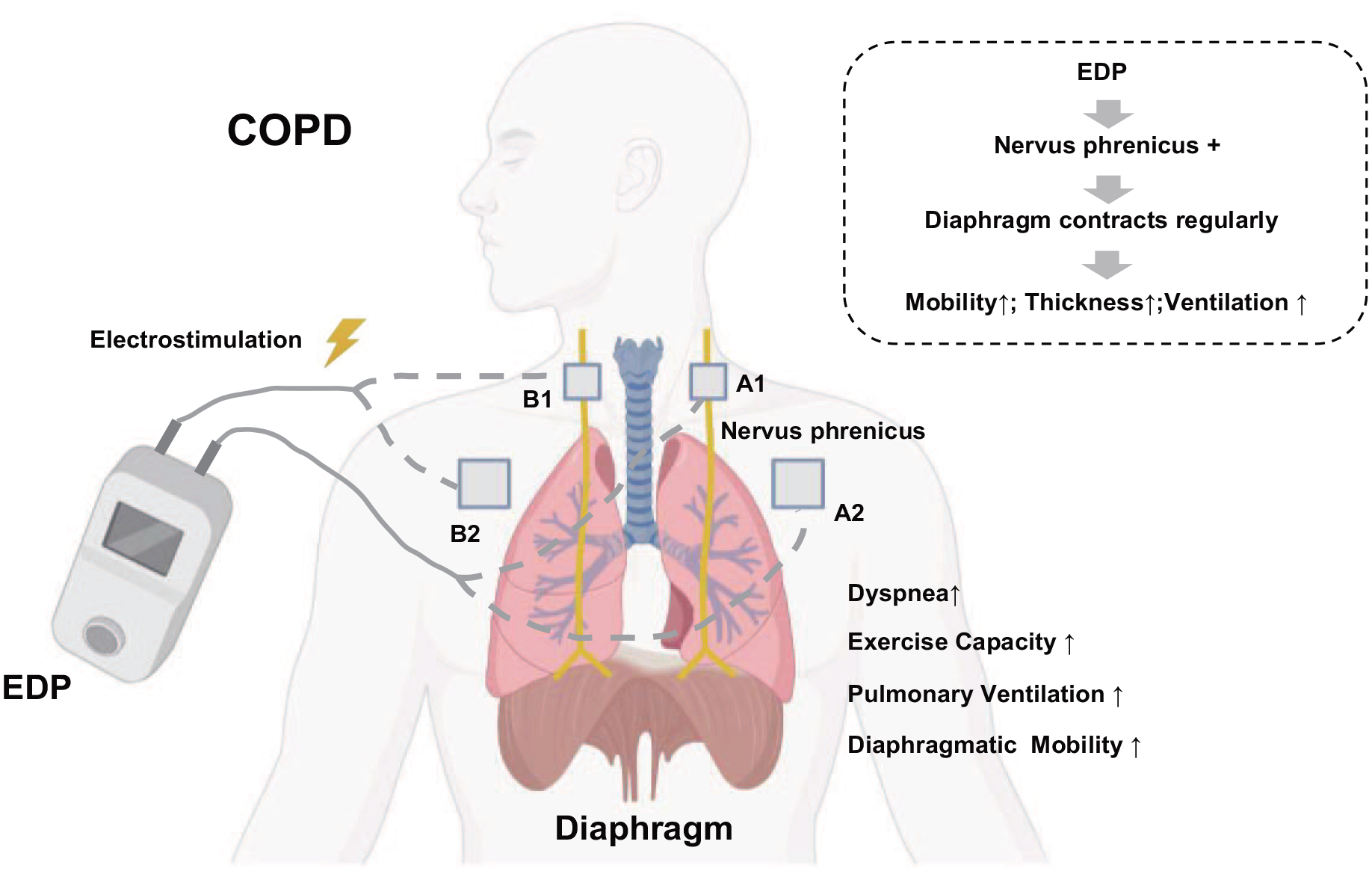
Effects and mechanisms of EDP.
In the current systematic review and meta-analysis, we searched for and included RCTs by searching databases that aimed to investigate the effects of EDP-CRTs versus CRTs on the therapeutic effect of COPD patients and to promote clinical decision-making regarding EDP-CRTs.
Materials and methods
Protocol and registration
We performed and reported this review by following the PRISMA guidelines. 13 This study protocol was registered on PROSPERO, ID number CRD42022355964.
Search strategy
Electronic searches of PubMed, Embase, Cochrane Central Register of Controlled Trials, Scopus, China Biology Medicine Disc, Chinese National Knowledge Infrastructure, Wan-Fang Database, and Chinese Scientific Journal Database were performed from database inception to 10 September 2023. We applied a combination of Medical Subject Heading terms and free-text keywords in each electronic database, and the specific retrieval methods are described in Supplemental Appendix 1. Searches were limited to the English and Chinese languages. Furthermore, we also searched for literature reviews related to this topic to screen whether their included studies met the inclusion criteria for this meta-analysis.
Eligibility criteria
RCTs investigating the effects of EDP-CRTs versus CRTs on COPD patients were included. Studies were selected for inclusion according to the Population, Intervention, Comparison, Outcome, and Study design parameters.
The exclusion criteria were as follows: (1) duplicate publications, case reports, reviews, retrospective studies, conferences, and meta-analyses; (2) data could not be extracted from the original literature; and (3) full text was not available.
Population
Adults with COPD are diagnosed based on their clinical history, physical examination, chest radiograph, and pulmonary function tests according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) clinical criteria for the diagnosis and severity of COPD. The included patients with moderate to very severe COPD, and there is no limitation of sex, nationality, race, etc.
Intervention
EDP combined with CRTs, which were used for intervention. Drug therapy (including anti-inflammatory agents, expectorant and anti-asthmatic, etc.), breathing training, and physical exercise training were considered CRTs.
Comparison
A comparable control group treated with CRTs was selected.
Outcomes
The primary outcome was pulmonary function, including forced expiratory volume in 1 s (FEV1), the percentage of predicted values of FEV1 (FEV1%pred), and FEV1/forced vital capacity (FVC)%; secondary outcomes included arterial blood gas analysis [the partial pressure of arterial oxygen (PaO2) and the partial pressure of arterial carbon dioxide (PaCO2)]; dyspnea [modified Medical Research Council Dyspnea Scale (mMRC)]; exercise capacity [6-min walking distance (6MWD)]; and quality of life [COPD assessment test (CAT)].
Study design
All RCTs investigating the effects of EDP-CRTs versus CRTs on patients with COPD were included.
Study selection
To determine the eligibility of identified studies, the first screening of the records was conducted by two independent reviewers. EndNote 20 was used to remove duplicate and irrelevant studies by screening abstracts and titles. Next, the two reviewers critically evaluated full-text versions of articles by applying further selection criteria to the available evidence and assessed whether a quantitative analysis could be performed. In the case of disagreement between the first screening and the full-text evaluation between two reviewers, the subject was discussed with a third author.
Data extraction
A data extraction form was created and applied by two independent reviewers. Extracted data included participant characteristics, study design, participants, intervention, frequency and duration, and interest outcomes. We involved a third reviewer in the case of a disagreement that could not be resolved by discussion.
Quality assessment
We assessed the quality of evidence and the strength of recommendations for outcomes using Grading of Recommendations Assessment, Development, and Evaluation (GRADE) recommendations. The GRADE pro 3.6 software was used for evaluating the following five items 14 : (1) risk of bias, (2) imprecision, (3) inconsistency, (4) indirectness, and (5) publication bias. Each item was graded as follows: no, serious (−1), or very serious (−2). The quality of evidence was classified into the following four categories: very low, low, moderate, and high.
The risk of bias in the studies was assessed using the revised Cochrane Risk of Bias tool for randomized trials (RoB 2.0),15,16 which covers the domains of D1 (bias arising from the randomization process), D2 (bias due to deviations from intended intervention), D3 (bias due to missing outcome data), D4 (bias in the measurement of the outcome), and D5 (bias in the selection of the reported result). Each item was judged as having a low, high, or some concerns. The entire appraisal was independently evaluated by two reviewers. Any disagreements were resolved by involving a third reviewer.
Data synthesis and statistical analysis
Review Manager (RevMan) 5.3 software (Cochrane Collaboration) was used for data synthesis, and meta-analysis for each outcome measure using post-intervention values. Weighted mean differences (WMDs) with 95% confidence intervals (CIs) were calculated when outcomes were measured with the same unit, and standardized mean differences (SMDs) with 95% CIs were calculated if the studies used different scales or units. The effect size was classified as small (SMD ⩽ 0.2), moderate (SMD = 0.21–0.79), or large (SMD ⩾ 0.8). 17
Statistical heterogeneity was assessed using the I2 statistic. We identified statistical heterogeneity of the outcomes as low (I2 < 50%), moderate (I2 = 50–75%), or high (I2 > 75%). 18 Random-effects models were applied when the pooled data had moderate or high heterogeneity, and fixed-effects models were used for low-heterogeneity comparisons. Due to differences in duration of intervention between included studies, subgroup analyses were performed in cases of high heterogeneity based on duration of intervention to explore the source of heterogeneity. If data from the studies could not be pooled to perform an effective analysis, the results were analyzed descriptively. Sensitivity analysis was performed by the sequential removal of each study to evaluate the individual study’s impact on the overall pooled effect size as an indicator of the stability of that result. Funnel plots were used to visually assess publication bias for outcomes included in more than or equal to 10 studies. 19
Results
Literature selection
A total of 674 studies were retrieved from the aforementioned databases. Eventually, 13 studies20–32 that met the inclusion criteria were selected for this meta-analysis. The processes of article screening and selection are shown in Figure 2.

Flow diagram of included studies.
Description of studies
Overall, 13 studies20–32 were identified that met the included criteria and were all from China. A total of 981 participants were included in this meta-analysis, which investigated the effects of EDP-CRTs versus CRTs on COPD. Participants were in the age range of 53–76 years. For a more comprehensive investigation, the effects of EDP-CRTs on COPD, and patients with COPD of different severity and stage were included. In this systematic review, one study 26 reported COPD participants in the acute phase, seven studies20,23,25,27,28,30,32 in the stable phase, and the remaining five studies21,22,24,29,31 did not mention. Furthermore, one study 23 reported COPD participants in the GOLD 2, two studies26,27 in the GOLD 2–3, one study 32 in the GOLD 2–4, and the remaining nine studies20–22,24,25,28–31 did not mention. As to the intervention, seven studies20,21,24,25,27,28,31 reported the control group was treated with drug therapy and breathing training, and the intervention group additionally received EDP. Four studies22,23,26,29 showed the use of drug therapy in the control group, and the intervention group was additionally treated with EDP. Two studies30,32 reported the control group received drug therapy and physical exercise training, and the intervention group additionally received EDP. More details are described in Table 1.
Characteristics of the included studies.
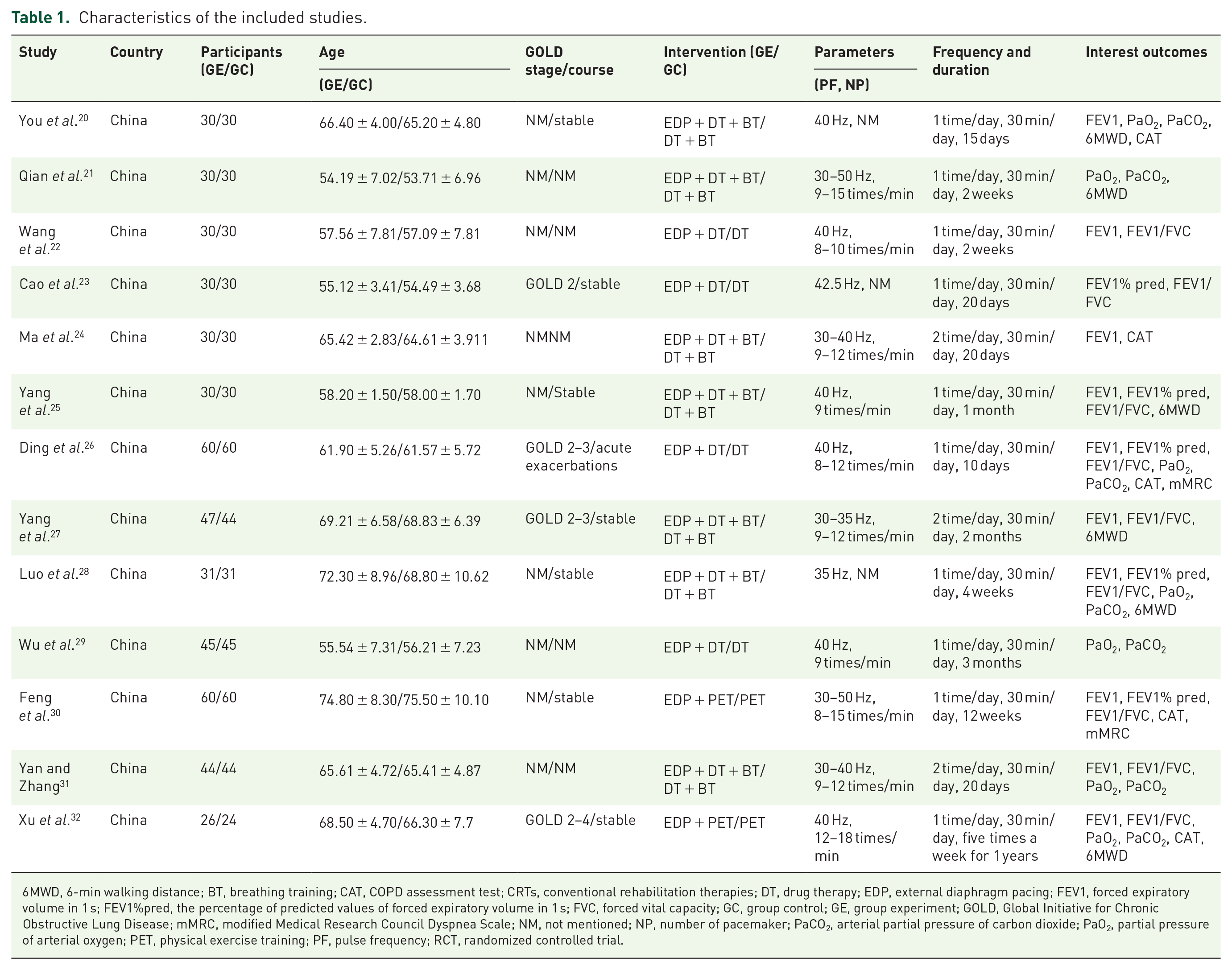
6MWD, 6-min walking distance; BT, breathing training; CAT, COPD assessment test; CRTs, conventional rehabilitation therapies; DT, drug therapy; EDP, external diaphragm pacing; FEV1, forced expiratory volume in 1 s; FEV1%pred, the percentage of predicted values of forced expiratory volume in 1 s; FVC, forced vital capacity; GC, group control; GE, group experiment; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, modified Medical Research Council Dyspnea Scale; NM, not mentioned; NP, number of pacemaker; PaCO2, arterial partial pressure of carbon dioxide; PaO2, partial pressure of arterial oxygen; PET, physical exercise training; PF, pulse frequency; RCT, randomized controlled trial.
Risk of bias assessment
The RoB assessment was performed using the Cochrane RoB 2 tool. Three different symbols were used to indicate the judgment, as follows: ‘+’ (Low), ‘–’ (Some concerns), and ‘×’ (High). All included studies20–32 had a low RoB of the randomization process, missing outcome data, measurement of the outcome, and selection of the reported result. Regarding the domain of D2 (bias of deviations from intended intervention), 12 studies20–31 presented a judgment of some concerns, one study 32 showed a judgment of low. The result of the RoB assessment is presented in Figure 3.

Risk of bias summary.
Quality of evidence
The overall quality of the evidence presented in this meta-analysis was low to moderate based on the GRADE system. We prepared ‘summary of findings’ tables for the main comparisons, which are presented in Supplemental Appendix 3.
Publication bias
The publication bias of the FEV1 result (including 10 studies22,24–28,30,31,32) was assessed. A visual analysis of the FEV1 result showed funnel plot asymmetry (Supplemental Appendix 2; Figure 1).
Primary outcome
Effect of EDP-CRTs versus CRTs on pulmonary function
FEV1
Ten studies22,24–28,30,31,32 used FEV1 to assess 749 participants. Low-quality evidence of the pooled results for EDP-CRTs versus CRTs demonstrated statistically significant differences in FEV1, and the effect size was large (SMD = 1.07, 95% CI = 0.58–1.56, p < 0.0001), with high heterogeneity (I2 = 90%) [Figure 4(a); Supplemental Appendix 3].

Forest plot showing the effects of EDP-CRTs versus CRTs on pulmonary function. (a) Forest plot of FEV1. (b) Forest plot of FEV1%pred. (c) Forest plot of FEV1/FVC%.
Subgroup analysis
Ten studies22,24–28,30,31,32 were divided into three subgroups: duration (<2 weeks), duration (2–4 weeks), and duration (>4 weeks). Statistical significance was observed favoring the EDP-CRTs group. We found a large effect size in the subgroup (duration: 2–4 weeks), with SMD = 1.67. Those results were presented in Supplemental Appendix 4: Supplemental Figure 1.
Sensitivity analysis
With high heterogeneity (I2 = 94%) in the subgroup (duration: 2–4 weeks), we performed further sensitivity analysis to remove the highly heterogeneous study and assess the stability of this result. The parameters of EDP in three studies20,22,28 were different from other studies,24,31 when we removed three studies,20,22,28 the results showed low heterogeneity (I2 = 0%), and the overall p effect was still positive (Supplemental Appendix 5: Supplemental Table 1).
FEV1%pred
Moderate-quality evidence of the pooled results of five studies21,23,25,26,28 (enrolling 400 participants) on EDP-CRTs versus CRTs demonstrated statistically significant differences in FEV1%pred (WMD = 6.67, 95% CI = 5.69–7.64, p < 0.00001) with low heterogeneity (I2 = 23%) [Figure 4(b); Supplemental Appendix 3].
Subgroup analysis
All studies21,23,25,26,28 were included in the subgroup analysis of the influence of duration on FEV1%pred, and statistical significance was observed favoring the EDP-CRTs group. A large effect size was observed in the subgroup (duration: 2–4 weeks), with SMD = 8.70. Those results were presented in Supplemental Appendix 4: Supplemental Figure 2.
FEV1/FVC%
Nine studies20,23,25–28,30,31,32 enrolling a total of 689 participants were included in the FEV1/FVC% analysis. Moderate-quality evidence of the results showed that the FEV1/FVC% of COPD patients in the EDP-CRTs group was significantly higher than that in the CRTs group, and the effect size was large (SMD = 1.24, 95% CI = 0.48–2.00, p = 0.001), with high heterogeneity (I2 = 95%) [Figure 4(c); Supplemental Appendix 3].
Subgroup analysis
We assessed the influence of the duration on FEV1/FVC%. Nine studies20,23,25–28,30,31,32 were divided into three subgroups (Supplemental Appendix 4: Supplemental Figure 3). Statistical significance was observed favoring the EDP-CRTs group. We found a large effect size in the subgroup (duration: <2 weeks), with SMD = 4.35.
Sensitivity analysis
When we performed a further sensitivity analysis of the subgroup (duration: 2–4 weeks), the result was still showed high heterogeneity and instability (Supplemental Appendix 5; Supplemental Table 2).
Descriptive analysis
Due to high heterogeneity in the subgroup (duration: 2–4 weeks), the results were analyzed descriptively. Cao et al. 23 in a study of 60 participants reported that the FEV1/FVC% were significantly greater in the EDP-CRTs group than in the CRTs group. Luo et al. 28 and Yan et al. 31 showed that pulmonary function in the EDP-CRTs group was significantly greater than that in the CRTs group. Wang et al. 22 reported statistically significant differences in FEV1 and FEV1/FVC% between the experimental and control groups.
Secondary outcomes
Effect of EDP-CRTs versus CRTs on arterial blood gas analysis
PaO2
Eight studies19,20,26–29,31,32 (621 participants) were pooled to examine the effect of providing EDP-CRTs versus CRTs on the PaO2, and the overall quality of the evidence was moderate (Supplemental Appendix 3). The effect was statistically significant and the effect size was large (SMD = 1.29, 95% CI = 0.74–1.84, p < 0.00001). However, the heterogeneity of the included studies was high (I2 = 90%) [Figure 5(a)].
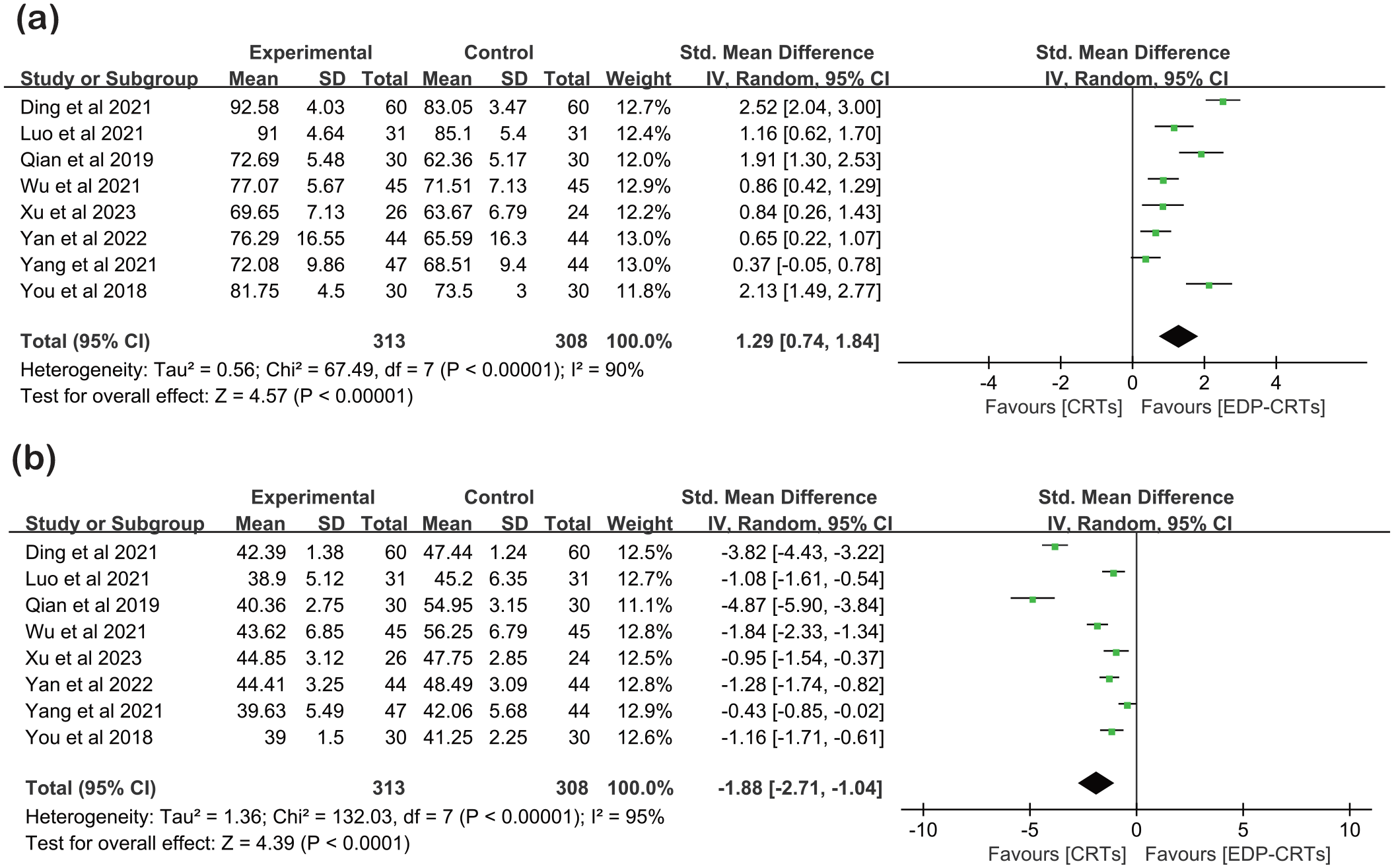
Forest plot showing the effects of EDP-CRTs versus CRTs on arterial blood gas analysis. (a) Forest plot of PaO2. (b) Forest plot of PaCO2.
Subgroup analysis
Eight studies19,20,26–29,31,32 were pooled into subgroup analysis, in which studies were in three different durations. Statistical significance was observed favoring the EDP-CRTs group. We found a large effect size in the subgroup (duration: <2 weeks), with SMD = 2.52 (Supplemental Appendix 4; Supplemental Figure 4).
Sensitivity analysis
High heterogeneity was still present in the subgroup (duration: 2–4 weeks) (I2 = 85%), and we performed further sensitivity analysis to remove the highly heterogeneous study and assess the stability of this result. With the duration of intervention in Luo et al. 28 and Yan and Zhang 31 was longer than other included studies,20,31 when we removed the two studies, the results of the subgroup (duration: >4 weeks) showed low heterogeneity (I2 = 0%), and the overall p effect was still positive (Supplemental Appendix 5; Supplemental Table 3).
PaCO2
Moderate-quality evidence of the results (eight studies20,21,26–28,31,32 with 621 participants) showed that the PaCO2 of COPD patients in the EDP-CRTs group was significantly higher than that in the CRTs group, and the effect size was large (SMD = −1.88, 95% CI = −2.71 to −1.04, p < 0.0001), with high heterogeneity (I2 = 95%) [Figure 5(b); Supplemental Appendix 3].
Subgroup analysis
All included studies20,21,26–28,31,32 were divided into three subgroups (Supplemental Appendix 4; Supplemental Figure 5). Statistical significance was observed favoring the EDP-CRTs group. However, it found no significant difference in the subgroup (duration: >2 weeks). In addition, we found a large effect size in the subgroup (duration: <2 weeks), with SMD = −3.82.
Sensitivity analysis
Due to high heterogeneity in the subgroup (duration: 2–4 weeks) (I2 = 93%) and subgroup (duration: >4 weeks) (I2 = 89%), we conducted a sensitivity analysis to remove the highly heterogeneous study and assess the stability of this result. In the subgroup (duration: 2–4 weeks), the mean age of participants in Qian et al. 21 was lower than other included studies,20,21,31 when we eliminated Qian et al., 21 the results of the subgroup showed low heterogeneity (I2 = 0%), and the overall p effect was still positive. In the subgroup (duration: >4 weeks), on account of the participants’ mean age in Wu et al. 29 was lower than other included studies,27,32 when Wu et al. 29 was eliminated, the results of the subgroup demonstrated moderate heterogeneity (I2 = 50%); meanwhile, the overall p effect was still positive. The above results are shown in Supplemental Appendix 5 and Supplemental Table 4.
Effect of EDP-CRTs versus CRTs on dyspnea
Two studies26,30 with 188 participants showed that the mMRC in the CRTs group was significantly higher than that in the EDP-CRTs group (WMD = −0.55, 95% CI = −0.65 to −0.45, p < 0.00001), while the statistical heterogeneity was low (I2 = 0%) [Figure 6(a); Supplemental Appendix 3] and the evidence was of moderate quality.
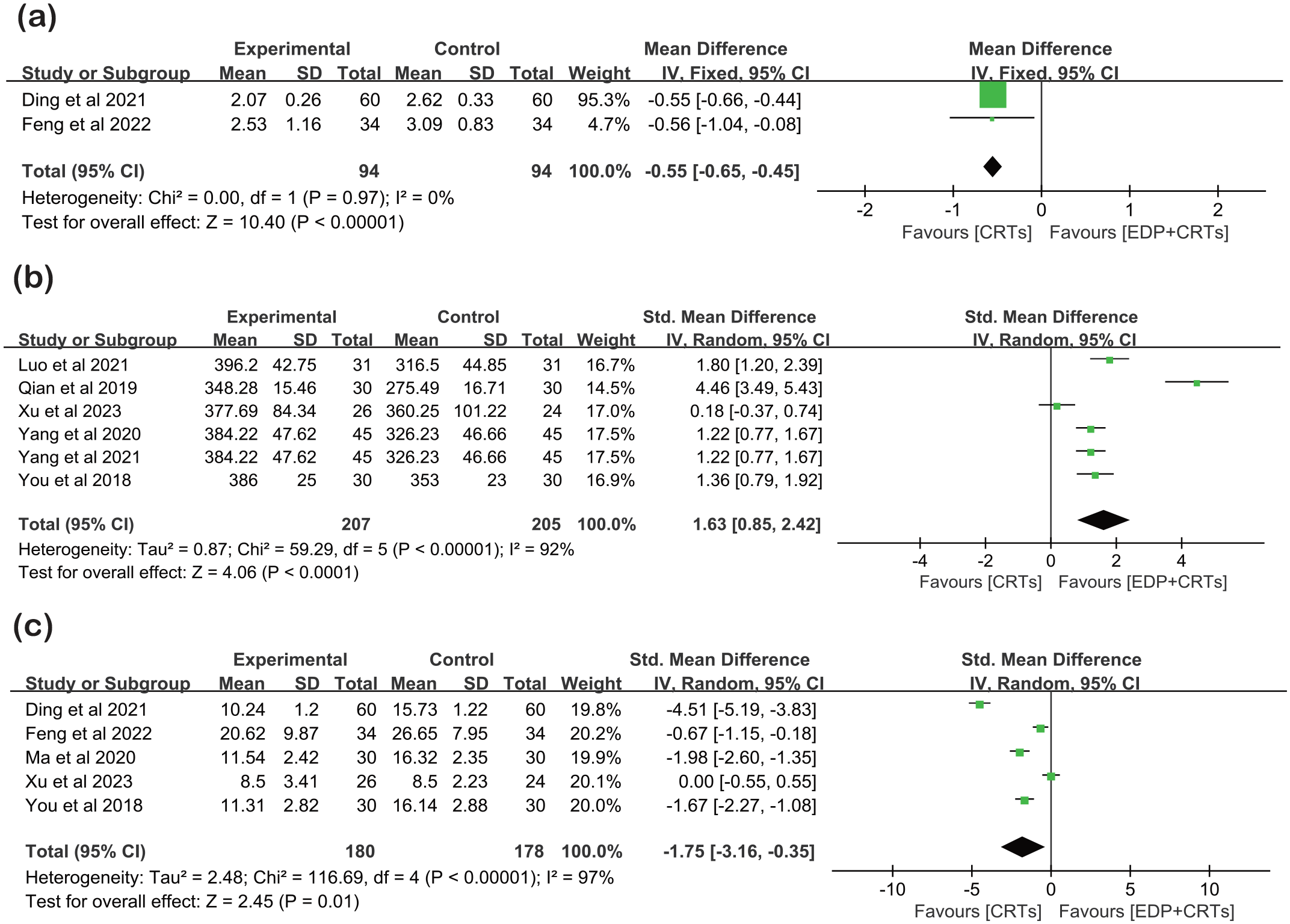
Forest plot showing the effects of EDP-CRTs versus CRTs on dyspnea, exercise capacity, and quality of life. (a) Forest plot of mMRC. (b) Forest plot of 6MWD. (c) Forest plot of CAT.
Subgroup analysis
Two studies26,30 were divided into two subgroups: duration (<2 weeks) and duration (>4 weeks). Statistical significance was observed favoring the EDP-CRTs group. We found a moderate effect size in the subgroup (duration: >4 weeks), with SMD = −0.56. Those results are presented in Supplemental Appendix 4 and Supplemental Figure 6.
Effect of EDP-CRTs versus CRTs on exercise capacity
Six studies20,21,25,27,28,32 with a total of 412 participants were included in the 6MWD analysis. Moderate-quality evidence of the results showed that the 6MWD of COPD patients in the EDP-CRTs group was significantly higher than that in the CRTs group, and the effect size was large (SMD = 1.63, 95% CI = 0.85–2.42, p < 0.0001), with high heterogeneity (I2 = 92%) [Figure 6(b); Supplemental Appendix 3].
Subgroup analysis
Six studies20,21,25,27,28,32 were divided into two subgroups: duration (2–4 weeks) and duration (>4 weeks). Statistical significance was observed favoring the EDP-CRTs group. We found a large effect size in the subgroup (duration: 2–4 weeks), with SMD = 2.49. Those results are presented in Supplemental Appendix 4 and Supplemental Figure 7.
Sensitivity analysis
With high heterogeneity in the subgroup (duration: 2–4 weeks) (I2 = 93%) and subgroup (duration: >4 weeks) (I2 = 80%), we conducted a sensitivity analysis to remove the highly heterogeneous study and assess the stability of this result. In the subgroup (duration: 2–4 weeks), the mean age of participants in Qian et al. 21 was lower than in other included studies,20,28 when we eliminated Qian et al. 21 the results of the subgroup showed low heterogeneity (I2 = 10%), and the overall p effect was still positive (Supplemental Appendix 4; Supplemental Table 5). In the subgroup (duration: >4 weeks), on account of the duration in Xu et al. 32 was longer than other included studies,25,27 when Xu et al. 32 were eliminated, the results of the subgroup demonstrated low heterogeneity (I2 = 0%); meanwhile, the overall p effect was still positive. The above results are shown in Supplemental Appendix 5 and Supplemental Table 5.
Effect of EDP-CRTs versus CRTs on quality of life
We pooled five studies20,24,26,30,32 (enrolling 358 participants) offering data on CAT results. Moderate-quality evidence of the results showed that the CAT results of COPD patients in the CRTs group were significantly greater than those in the EDP-CRTs group (WMD = −1.75, 95% CI = −3.16 to −0.35, p < 0.00001), with high heterogeneity (I2 = 97%) [Figure 6(c); Supplemental Appendix 3].
Subgroup analysis
Five studies20,24,26,30,32 were included in the subgroup analysis (Supplemental Appendix 4; Supplemental Figure 8). Statistical significance was observed favoring the EDP-CRTs group. We found a large effect size in the subgroup (duration: <2 weeks), with SMD = −4.51.
Discussion
In the present study of 13 studies including 981 participants, our overall findings supported the fact that EDP-CRTs versus CRTs can improve pulmonary function, arterial blood gas analysis, dyspnea, exercise capacity, and quality of life of COPD patients. The overall quality of the evidence is low to moderate based on the GRADE system.
Targeted rehabilitation methods for diaphragmatic dysfunction in COPD patients mainly include diaphragmatic breathing, manual therapy, and phrenic nerve stimulation, which have been shown to improve diaphragm function, pulmonary ventilation function, dyspnea, and exercise capacity. 8 However, for those COPD patients who are limited by the effects of reduced exercise capacity and fatigue-prone respiratory muscles, the implementation of diaphragmatic breathing and manual therapy is greatly limited; meanwhile, the disadvantage of these rehabilitation training is that they are slow to be effective and not easily adhered to by patients, resulting in reduced patient compliance and clinical effects.9,24 Non-invasive phrenic nerve stimulation, which is passive, safe, and easy to perform, can provide a valuable complementary method to improve diaphragm dysfunction. Previous studies have shown that it can prevent diaphragm atrophy in patients with respiratory failure on mechanical ventilation 33 and avoid ventilator-induced diaphragm dysfunction in critical care. 34 In recent years, EDP as a non-invasive phrenic nerve stimulation, which is widely used in respiratory dysfunction in COPD patients. A previous literature review reported that EDP can be used as an effective tool for clinicians to improve the therapeutic effect of COPD patients, 11 and the basic principle of EDP is to improve respiratory function by stimulating the phrenic nerve through electrodes on the body surface, causing the diaphragm to move with regular contraction and increasing ventilation. 35
To our knowledge, this is the first meta-analysis to quantitatively assess the effectiveness of EDP-CRTs for rehabilitation in COPD patients. Our study provides a more comprehensive assessment of EDP-CRTs, the clinical practice suggestion that can be recommended to clinicians is EDP as an effective complementary rehabilitation strategy to CRTs. In addition, based on the results of subgroup analysis, our finding suggested that for the duration (2–4 weeks), EDP-CRTs could provide a greater effect size on FEV1, FEV1/FVC%, 6MWD, and CAT. Noteworthy, there was only one study or two studies in the subgroup (duration: <2 weeks) of FEV1%pred, PaO2, and PaCO2, and subgroup (duration: >4 weeks) of mMRC; thus, we did not produce useful findings with the subgroup analysis of those outcomes and clinicians should be cautious in making clinical suggestions based on the subgroup analysis. Overall, in the application of EDP-CRTs in clinical practice, our study recommended setting the duration of 2–4 weeks, which had a greater impact on the effects of patients with COPD.
Speculatively, some potential issues need to be considered when promoting clinical decision-making regarding EDP-CRTs. Considering the RoB of the included studies, 12 studies20–31 showed a judgment of some concerns on the domain in D2 (bias of deviations from intended intervention); specifically, the implementation of the allocation concealment was poor or not mentioned in the above-mentioned studies. We downgraded the certainty of the evidence of all the outcomes based on the GRADE system. The overall quality of evidence was low to moderate quality. We found high RoB across all included studies mainly due to the lack of a blinding method (blinding of subjects, therapists, or outcome assessors); thus, we downgraded one level for RoB (performance bias and detection bias). Furthermore, we downgraded one level for risk of bias (publication bias) on the FEV1 due to its potential publication bias. In general, our findings suggest the need for further high-quality RCTs of EDP-CRTs versus CRTs in COPD patients.
Results based on this systematic review, there are some clinical recommendations for parameters, frequency, and duration of EDP were as follows: (1) the pulse frequency set to 30–40 Hz and the number of pacemakers set to 9–12 times/min; (2) the frequency is one to two times a day for 30 min; and (3) the duration to achieve the most effective treatment is 2–4 weeks. Importantly, clinicians should comprehensively consider the use of EDP in the context of specific clinical practice and the condition of COPD patients.
Limitations
The present study has some limitations. First, all included studies were from China, and no other country’ studies met the inclusion criteria; thus, the pooled results of this study are at risk of country bias. Second, this systematic review included COPD patients of varying severity and stage who might have different effects of rehabilitation, further driving the subgroup analysis of severity or stage of COPD, which might be better to guide clinical practice. Third, COPD as a chronic disease requires long-term management and follow-up; however, the included studies did not report follow-up data of intervention of EDP-CRTs and showed difficulty observing the development of COPD. Fourth, the limited number of included studies made it difficult to produce useful findings with the planned subgroup analysis (i.e. 10 studies for the outcome measure analyzed according to the Cochrane Handbook); thus, clinicians should be cautious in making clinical suggestions based on the subgroup analysis of this systematic review.
Conclusion
Low to moderate quality of evidence-supported EDP-CRTs has a better effect on the recovery of pulmonary function, arterial blood gas analysis results, dyspnea, exercise capacity, and quality of life of COPD patients than CRTs, and duration to achieve the most effective treatment is 2–4 weeks.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231218086 – Supplemental material for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tar-10.1177_17534666231218086 for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Linhong Jiang, Pingping Sun, Peijun Li, Weibing Wu, Zhenwei Wang and Xiaodan Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666231218086 – Supplemental material for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-2-tar-10.1177_17534666231218086 for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Linhong Jiang, Pingping Sun, Peijun Li, Weibing Wu, Zhenwei Wang and Xiaodan Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-3-tar-10.1177_17534666231218086 – Supplemental material for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-3-tar-10.1177_17534666231218086 for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Linhong Jiang, Pingping Sun, Peijun Li, Weibing Wu, Zhenwei Wang and Xiaodan Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-4-tar-10.1177_17534666231218086 – Supplemental material for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-4-tar-10.1177_17534666231218086 for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Linhong Jiang, Pingping Sun, Peijun Li, Weibing Wu, Zhenwei Wang and Xiaodan Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-5-tar-10.1177_17534666231218086 – Supplemental material for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-5-tar-10.1177_17534666231218086 for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Linhong Jiang, Pingping Sun, Peijun Li, Weibing Wu, Zhenwei Wang and Xiaodan Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-6-tar-10.1177_17534666231218086 – Supplemental material for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, sj-docx-6-tar-10.1177_17534666231218086 for Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Linhong Jiang, Pingping Sun, Peijun Li, Weibing Wu, Zhenwei Wang and Xiaodan Liu in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.